

Summary
This article discusses results from the REgistry on Cardiac rhythm disORDers: an international observational prospective survey assessing the control of Atrial Fibrillation (RecordAF) registry that confirmed and complemented results from previous controlled randomized trials.
- Arrhythmias Clinical Trials
The clinical outcomes that are associated with rate control versus the restoration and maintenance of normal sinus rhythm in the treatment of atrial fibrillation (AF) have been explored in a number of large-scale clinical trials [Wyse DG et al. N Engl J Med 2002; Van Gelder et al. N Engl J Med 2002]. No advantages for either treatment strategy with respect to major cardiovascular (CV) outcomes have been reported. John Camm, MD, St. George's Hospital Medical School, London, UK, reported results from a reallife, international, observational, prospective, longitudinal cohort study that confirmed and complemented results from these previous controlled randomized trials.
The RecordAF (REgistry on Cardiac rhythm disORDers: an international observational prospective survey assessing the control of Atrial Fibrillation) registry was established to trace the influence of a physician's choice of a rate versus rhythm control strategy on clinical outcome for patients with first onset or recent recurrent AF. Patients (n=5604) aged 18 years and older with a <1-year history of AF were selected from 532 randomly chosen general cardiology practices in 21 countries. Patients with permanent or transient AF were not eligible. The primary study endpoint was the rate of therapeutic success of AF management (in sinus rhythm or at rate control target with no major CV event and no change in strategy) at 12 months. The co-primary endpoint was the rate of major CV events (eg, CV death, myocardial infarction, stroke, transient ischemic attack [TIA], and hospitalizations).
At baseline, 45.1% (n=2528) of patients in the registry were being treated with a rate control strategy and 54.9% (n=3076) were treated with a rhythm control strategy. Patients in the rhythm control group were an average of 3 years younger than those on rate control (64 vs 67 years; p<0.001) and had a significantly (p<0.001) lower resting heart rate (76.6 vs 80.6 beats per minute). Body mass index and systolic blood pressure were slightly but significantly (p=0.008 and p=0.02, respectively) greater in the rhythm control group.
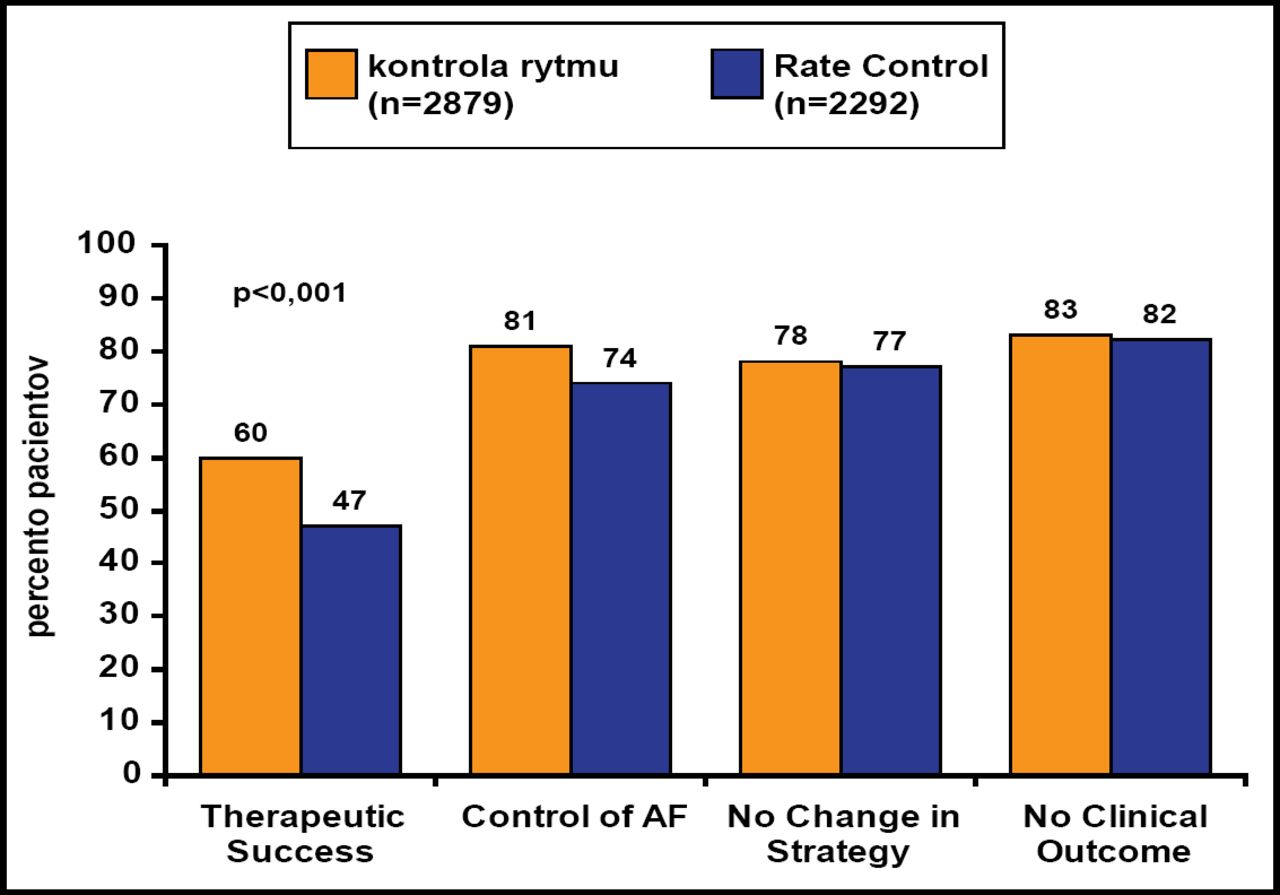
Data for 92.3% of patients were available after 1 year of follow-up, at which time more patients in the rhythm control group were in sinus rhythm (81% vs 33%). Approximately 50% of patients had a change in pharmacological treatment and 20% had a change in therapeutic strategy in both groups. Therapeutic success was achieved significantly (p<0.001) more frequently in patients who were treated by rhythm control (60% vs 47%), which was driven by control of AF (Figure 1). For the co-primary endpoint, there was no difference (p=0.35) between the two strategies in terms of overall clinical events (18% in rate control vs 17% in rhythm control groups). Multivariate analysis showed that the occurrence of cardiovascular clinical events was more dependent on comorbidity (coronary artery disease, heart failure, age >75 years, renal disease, prior stroke/TIA) than the choice of strategy. Hospitalizations for arrhythmia were more common in the rhythm (11%) versus rate control group (7%), and hospitalizations for heart failure management were more common in the rate (5%) versus rhythm control group (2%).
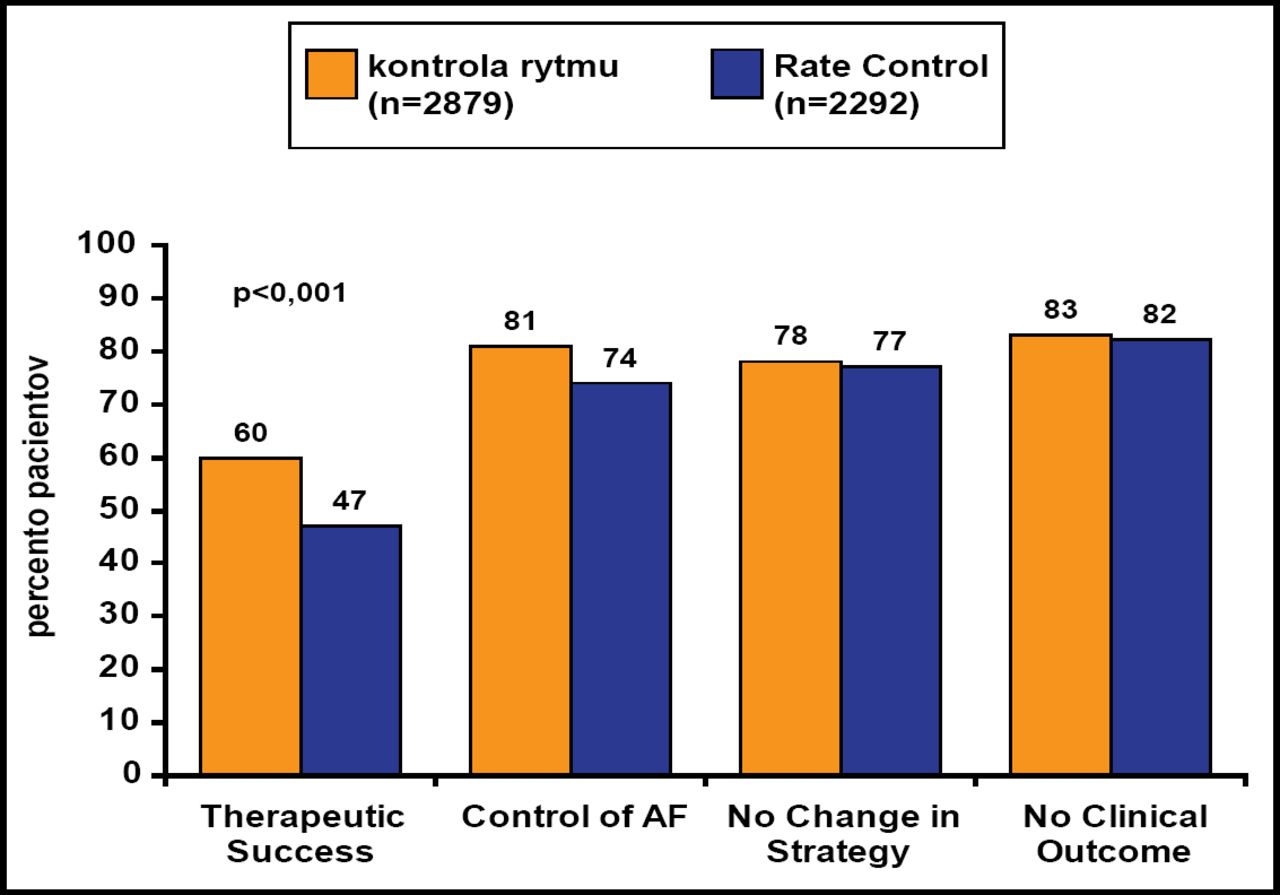
Primary Endpoint at One Year.
Reproduced with permission by J. Camm, MD.
Prof. Camm concluded that although successful management of AF was achieved more often with rhythm control, this did not translate into better outcomes.
- © 2009 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.