

Summary
This article discusses the therapeutic challenges that are associated with the combination of coronary artery disease (CAD) and diabetes mellitus. The link between CAD and dysglycemia is that the release of stress hormones and peptides due to a myocardial infarction is associated with insulin resistance and increased glucose or free fatty acid levels.
- Coronary Artery Disease
- Diabetes Mellitus
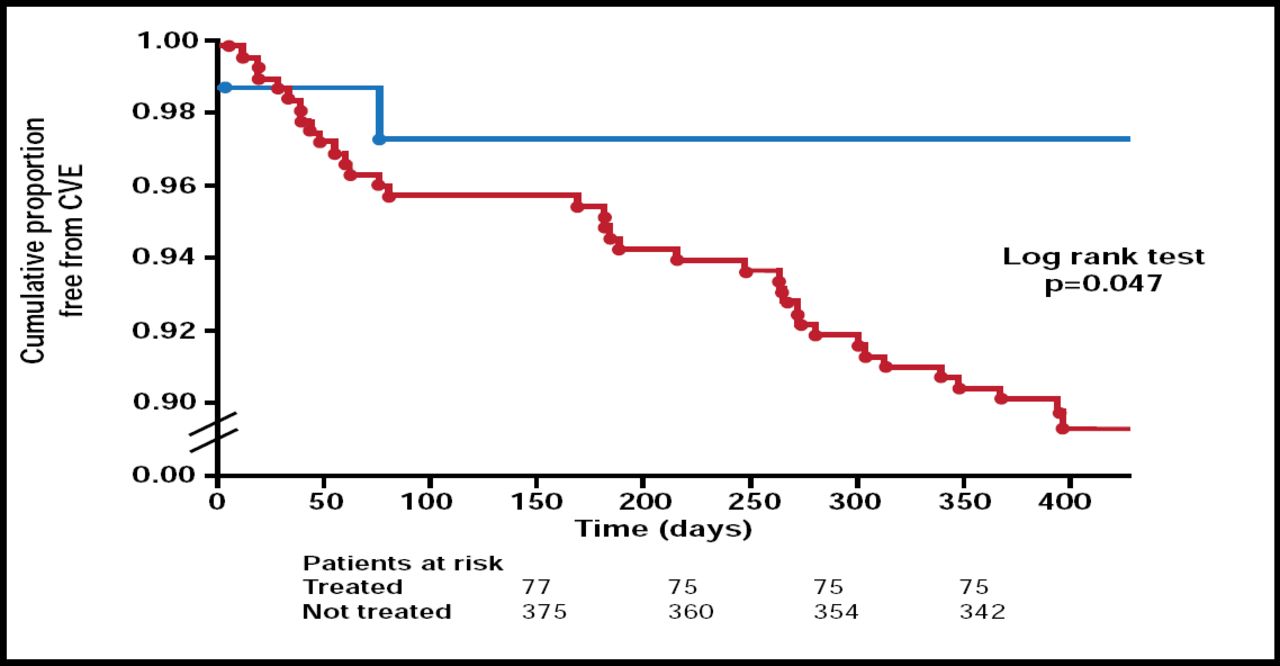
Hyperglycemia is common but often undiagnosed in patients with coronary artery disease (CAD) in Europe and Asia; yet, patients with abnormal glucose tolerance have a significantly (p=0.002) higher probability of having a cardiovascular (CV) event compared with those with normal glucose tolerance [Bartnik M et al. Eur Heart J 2004]. This risk can be significantly (p=0.041) reduced with glucose-lowering drugs (Figure 1) [Anselmino M et al. Eur Heart J 2008]. In a study that assessed the relationship between impaired fasting glucose and impaired glucose tolerance, as well as diabetes mellitus (DM) and all-cause and cardiovascular disease (CVD) mortality, 65% of patients who died of CVD had known DM, newly diagnosed DM, impaired fasting glucose, or impaired glucose tolerance at baseline.
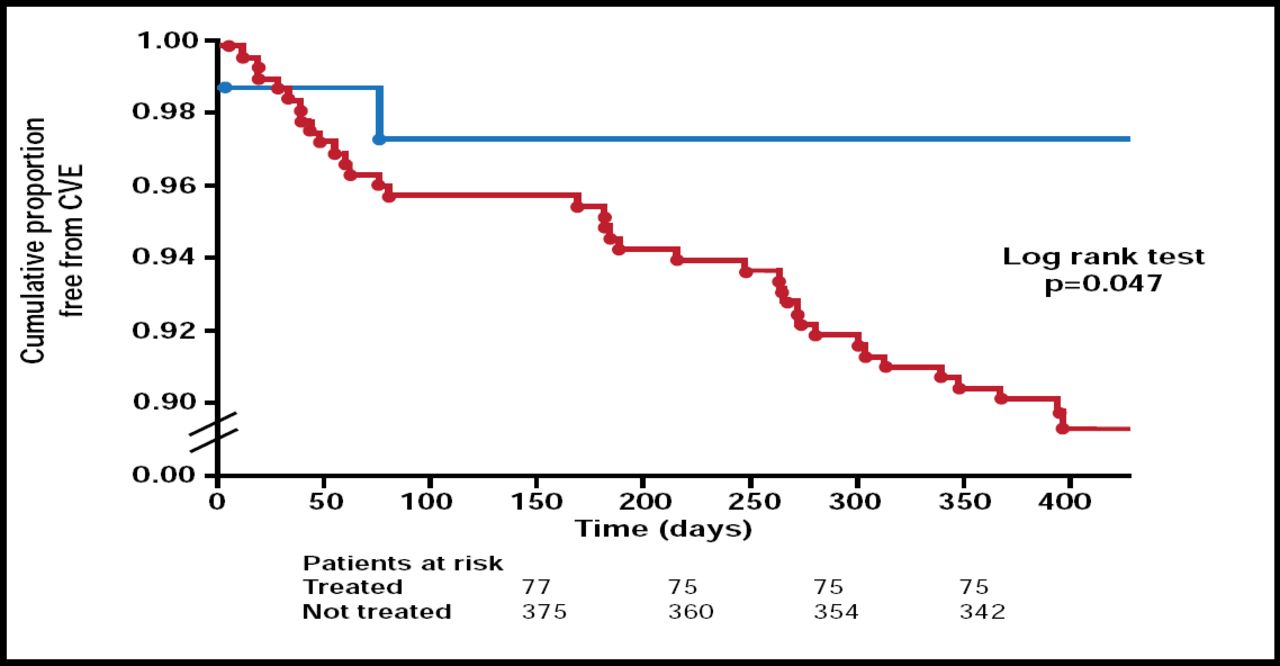
Euro Heart Survey: Improved CV Outcomes in Patients with Newly Detected Diabetes and Implementation of Diabetes Pharmacotherapy.
Anselmino M et al. Eur Heart J 2008; 29:177–184. By permission of Oxford University Press.
Professor Linda Mellbin, MD, Karolinska Institute, Stockholm, Sweden, discussed the therapeutic challenges that are associated with the combination of CAD and DM. She said that a possible link between CAD and dysglycemia is that the release of stress hormones and peptides due to a myocardial infarction is associated with insulin resistance and increased glucose or free fatty acid levels. They may induce oxidative stress and endothelial dysfunction, which in turn lead to inflammation, thrombus formation, and ischemia. The use of beta-blockers and glucose-lowering agents in the acute setting may limit these harmful reactions. Data have shown that intensive multifactorial therapy, in a long-term perspective, with glucose regulation and the use of renin-angiotensin system blockers, aspirin, and lipid-lowering agents is associated with a lower risk of death from CV causes (HR, 0.43; 95% CI, 0.19 to 0.94; p=0.04) and of cardiovascular events (HR, 0.41; 95% CI, 0.25 to 0.67; p<0.001) [Gaede P et al. N Engl J Med 2008].
Prof. Mellbin stressed the need for aggressive, guideline-based treatment to control blood pressure, lower serum cholesterol, and abolish cigarette smoking for diabetic patients with CAD.
Professor Lars Ryden, MD, Karolinska University Hospital, Stockholm, Sweden, listed the following 10 most important recommendations from the guidelines, jointly issued by the European Society of Cardiology and European Association for the Study of Diabetes, for adult patients with diabetes, prediabetes, and CAD (full-text document freely available at http://wwwescardio.org or http://www.easd.org):
-
To reach all treatment targets, including glycemic control
-
To screen for DM and impaired glucose tolerance by means of an OGTT in all patients with CAD and other high-risk individuals
-
To see lifestyle counseling as a cornerstone in preventing DM and CVD
-
To offer patients with DM and acute coronary syndrome standard, guideline-based treatment and early angiographic and mechanical revascularization
-
To apply strict, when needed insulin-based, glucose control in acutely ill DM patients.
-
To favor coronary artery bypass graft over percutaneous coronary intervention (PCI) when revascularizing DM patients
-
To use drug-eluting stents in PCI with stent implantation
-
To include investigations for cardiac autonomic dysfunction, heart failure, arrhythmias, hypotension, peripheral vascular disease (Doppler index), and (micro)albuminuria in routine follow-up
-
To use a multifactorial (no smoking; tight glucose, blood pressure, and lipid control; and antiplatelet therapy) approach
-
To establish collaboration between cardiologists and diabetologists in the management team
- © 2009 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.