

Summary
This article discusses some of the open issues in implantable cardioverter-defibrillator and cardiac resynchronization therapy.
- Interventional Techniques & Devices
- Heart Failure
Professor Pangiotis Vardas, MD, Heraklion University Hospital, Crete, Greece, discussed some of the open issues in implantable cardioverter-defibrillator (ICD) and cardiac resynchronization therapy (CRT). Commenting on the concern about the high number of patients who must be treated (NNT) to save 1 life with ICD implantation and CRT, Prof. Vardas reminded the audience that “this number is highly dependent on the time window over which the benefit is assessed.” Pointing to the MADIT-II trial, he noted that while the NNT in Year 1 was 133 patients, it was only 17 in Year 2 and 11 in Year 3. Another important issue for ICDs and CRT therapy is the criteria for patient evaluation, which Prof. Vardas believes should be updated with a particular need for additional, more reliable markers. Technical issues that he believes need to be addressed include device longevity, inappropriate shocks, lead reliability, and follow-up for ICDs and lead stability, easier device programming, and follow-up for CRT. In concluding, Prof. Vardas suggested that existing guidelines need to be modified, particularly for patients with mild heart failure (HF), in light of the recent study results.
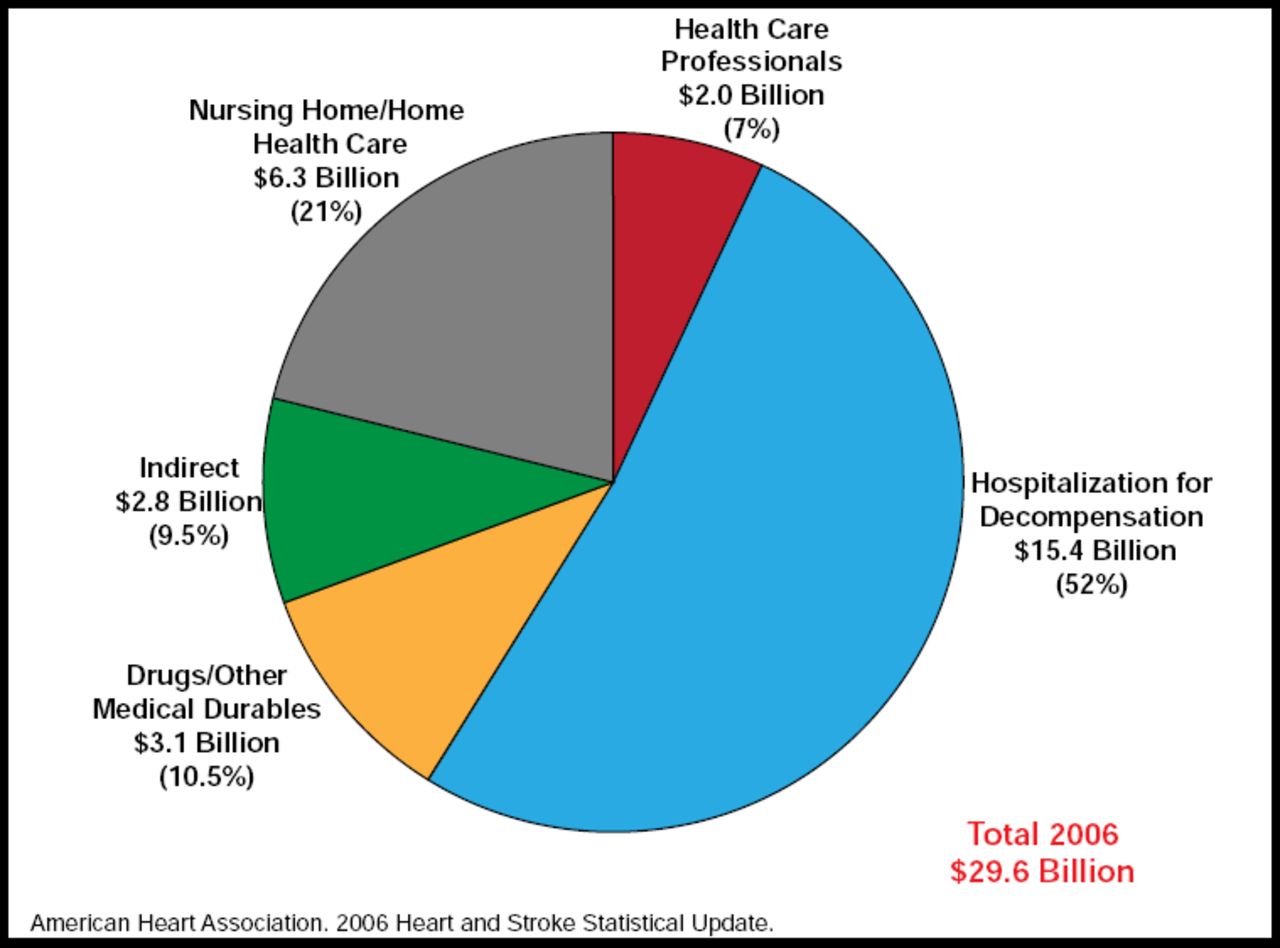
HF is the most common cause of hospitalization due to cardiovascular disease in patients aged over 65 years, and it has a considerable impact on health care costs (Figure 1) [AHA. Heart and Stroke Statistical Update 2006], noted Professor Luigi Tavazzi, MD, GVM Care and Research, Cotignola, Italy.
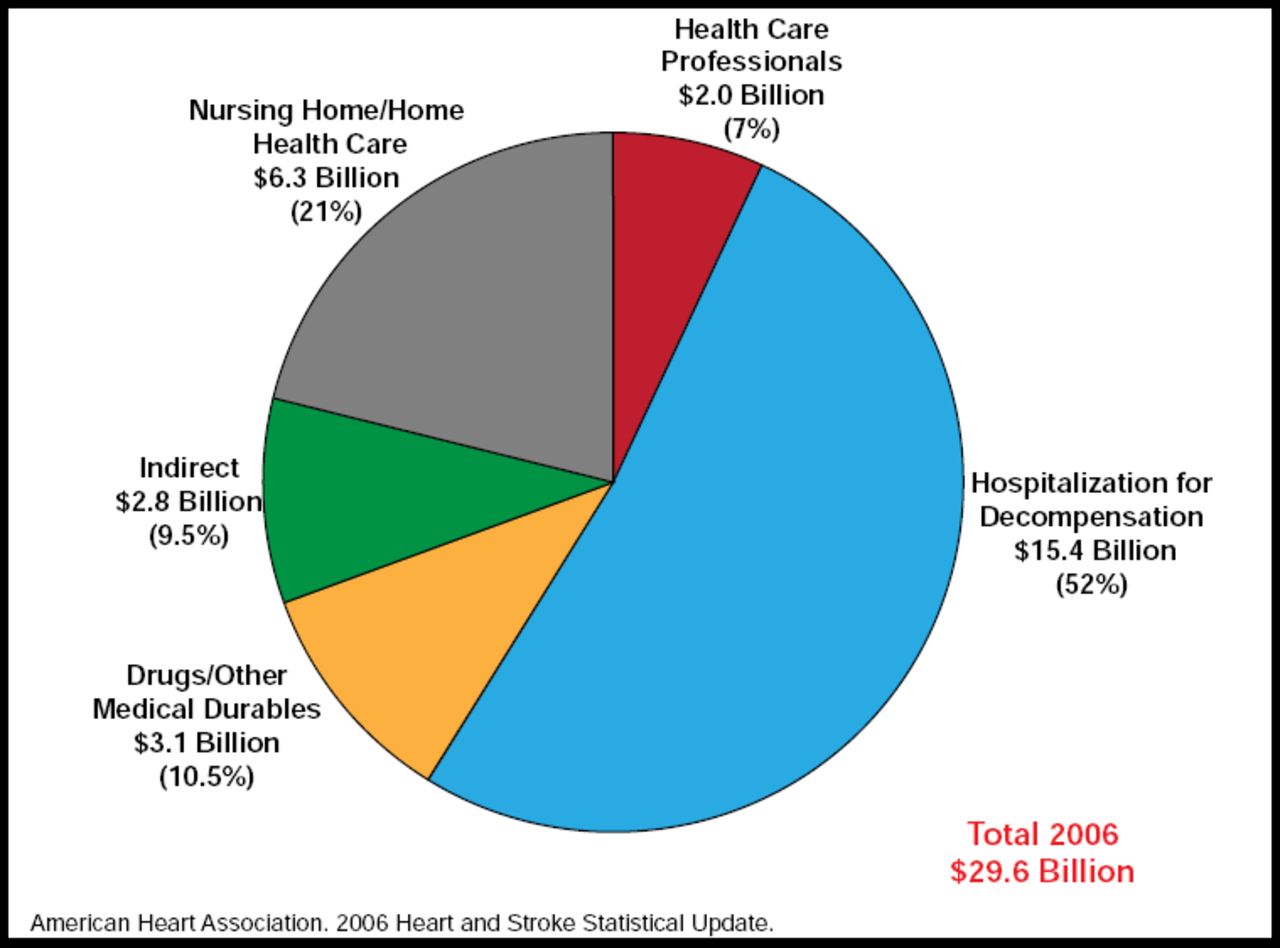
Impact of HF Hospitalizations in Patients Aged Over 65 Years on Health Care Costs.
Reproduced with permission by L. Tavazzi.
Prof. Tavazzi discussed some of the recent technological advancements that raise the possibility that remotely acquired physiological data from permanently implanted CRT/ICD devices may contribute to the management of HF patients by allowing for timely treatment. Several devices are currently being tested in clinical trials, including the PARADYM™-8770 sonR™ cardiac resynchronization therapy defibrillator (CRT-D), which is designed to adjust CRT delivery based on hemodynamic response. Another device in testing is the InSync Sentry, a CRT-D device with automatic intrathoracic fluid status monitoring (OptiVol™ Fluid Status Monitoring) that assesses a patient's fluid status by measuring, tracking, and reporting intrathoracic impedance. Prof. Tavazzi said that the combination of multiple diagnostics is feasible and may increase the clinical utility of device monitoring.
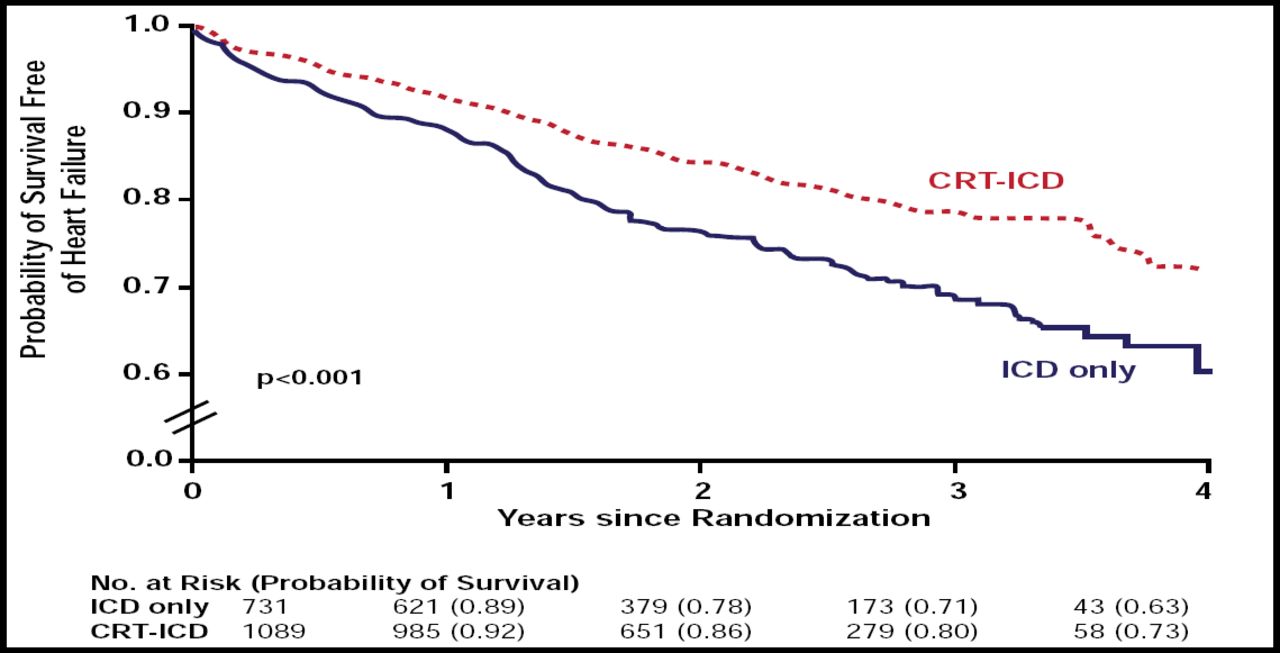
Results from the MADIT-CRT (Multicenter Automatic Defibrillator Implantation Trial with Cardiac Resynchronization Therapy; NCT00180271) study, presented by Arthur J. Moss, MD, University of Rochester, Rochester, NY, showed that asymptomatic or mildly symptomatic cardiac patients who are treated with CRT-D have a significant 34% (p=0.001) lower risk of HF or death than those who receive a standard ICD only.
MADIT-CRT was a randomized, multicenter, international trial that comprised 1820 patients (∼53% aged ≥65 years; 75% men) with New York Heart Association Class I or II (no or mild symptoms) who had either ischemic or nonischemic heart disease with LVEF <30% and QRS duration of >130 ms on ECG. Subjects were randomized to receive either CRT-D (n=1089) or ICD (n=731) along with optimal medical therapy. Subjects were followed for an average of 24 months. The primary study endpoint was all-cause mortality or an HF event, whichever occurred first.
CRT-Dtherapywas superior on the primary endpoint (Figure 2) and in all patient subgroups. The benefit was driven by a 41% reduction in HF events. CRT-D was more effective in women (HR, 0.37; 95% CI, 0.22 to 0.61) versus men (HR, 0.76; 95% CI, 0.59 to 0.97) and in subjects who had wider (HR, 0.48; 95% CI, 0.37 to 0.64) versus narrower (HR, 1.06; 95% CI, 0.74 to 1.52) QRS complexes. Full article: http://content.nejm.org/cgi/content/full/NEJMoa0906431v1.
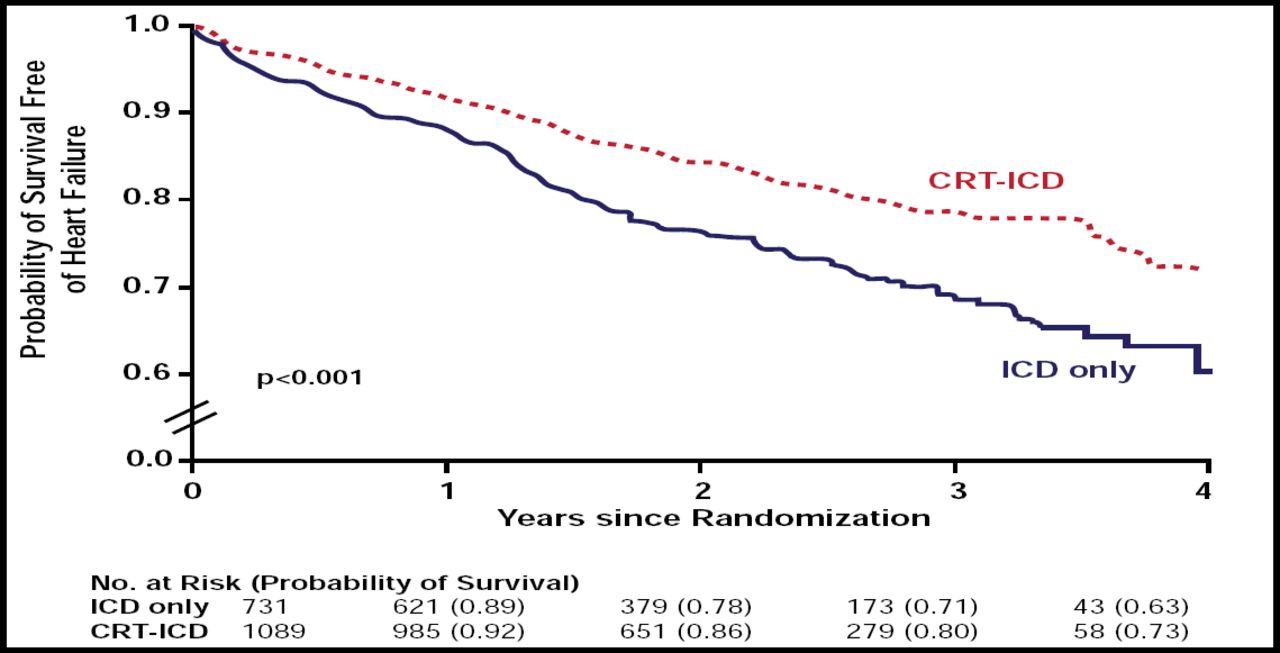
Kaplan-Meier Estimates of the Probability of Survival Free of HF.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.