

Summary
Reperfusion therapy with IV rt-PA and recanalization produces good outcomes in patients with acute stroke, but challenges remain. It is estimated that 85% of all ischemic strokes are not treated with thrombolysis; thus, improved and early access to treatment is needed. It is suggested that the 3 to 6-hour time window for treatment may be extended by better patient selection criteria using transcranial Doppler markers of the diffusion-perfusion mismatch method [Restrepo L et al. J Neuroimaging 2006] and combination therapies, such as reduced-dose rt-PA plus eptifibatide [Pancioli AM et al. Stroke 2008] or rt-PA plus GPIIb/IIIa antagonists.
- Cerebrovascular Disease
- Interventional Techniques & Devices
Reperfusion therapy with IV rt-PA and recanalization produces good outcomes in patients with acute stroke, but challenges remain. Carlos A. Molina, MD, Hospital Vall d'Hebron, Barcelona, Spain, estimates that 85% of all ischemic strokes are not treated with thrombolysis; thus, improved and early access to treatment is needed. He suggested that the 3 to 6-hour time window for treatment may be extended by better patient selection criteria using transcranial Doppler markers of the diffusion-perfusion mismatch method [Restrepo L et al. J Neuroimaging 2006] and combination therapies, such as reduced-dose rt-PA plus eptifibatide [Pancioli AM et al. Stroke 2008] or rt-PA plus GPIIb/IIIa antagonists.
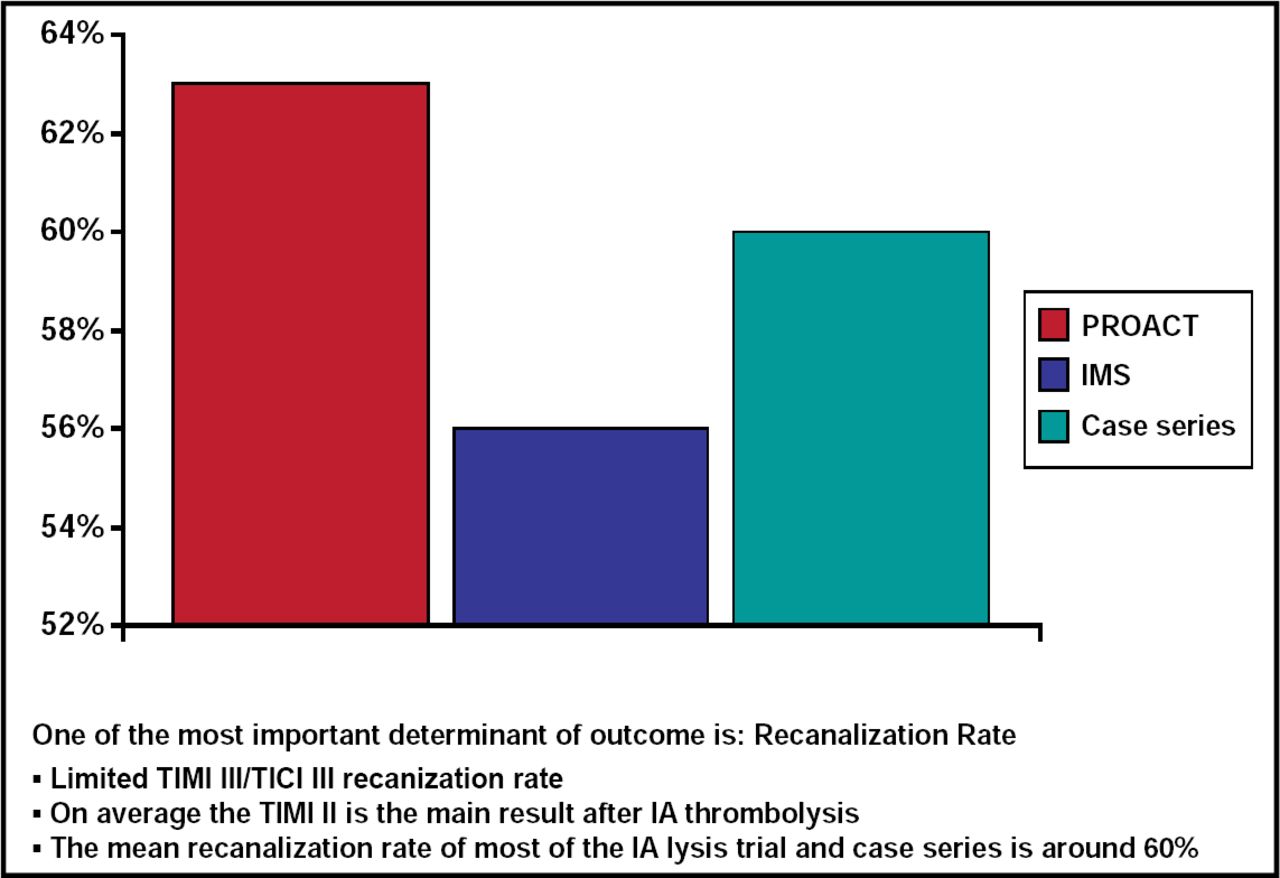
Although thrombolytic therapy has revolutionized treatment of acute ischemic stroke (AIS), its utilization is limited due to the short time window for use, poor specificity for the site of arterial occlusion, and suboptimal recanalization rates. Osama O. Zaidat, MD, MS, Vascular and Interventional Neurology, Medical College of Wisconsin, Milwaukee, WI, discussed the advantages and disadvantages of circumventing these problems by using intra-arterial (IA) thrombolysis. Two pivotal studies, Prolyse in Acute Cerebral Thromboembolism (PROACT) and the Interventional Management of Stroke (IMS), provided evidence for the effectiveness of IA thrombolysis. One of the most important determinants of outcome is recanalization rate, which is about 60% in IA lysis trials (Figure 1). The degree of recanalization and good clinical outcome are directly related to time to therapy [Zaidat OO et al. Am J Neuroradiol 2005]. Limitations of IA lysis may be related to clot characteristics, wherein white platelet-rich clots are more resistant to lytics and fresh red blood cell-rich clots are more responsive to lytics. The use of synthetic inhibitors (eg, monoclonal antibodies, such as abciximab; the peptide eptifibatide; and nonpeptides, such as tirofiban, lamifiban, xemilofiban, etc.) may overcome these limitations. IA pharmacological thrombolysis therapy is fast and relatively easy to administer, but it is slow to work, and frequently it does not work at all, concluded Dr. Zaidat. However, currently it is the best treatment that we have.

Recanalization Rates for PROACT, IMS, and Case Series.
Sixty percent of stroke centers report treating IV tPA “failures” with IA. When stroke centers were surveyed regarding their intervention strategies, 43% reported using IA rt-PA as initial strategy, 43% moved to the MERCI® retriever as a second choice, and 35% used angioplasty as a third choice when the other two failed. Italo Linfante, MD, Baptist College and Vascular Institute, Miami, FL, stated that the IA approach to acute large vessel occlusion (mechanical or pharmacological) is here to stay and continues to grow. Thus, we need more evidence-based IA trials that take into consideration the rapidly emerging device technology.
Approaches to vascular protection after acute stroke were discussed in a forum that followed the main session. Recovery from a vascular injury may be facilitated by neuroprotection but neuroprotection can only be achieved with a functioning vasculature, stated Susan C. Fagan, PharmD, University of Georgia College of Pharmacy, Augusta, GA. Pharmacological agents and therapeutic interventions that are designed to target specific pathological and protective processes that affect the vasculature during the acute (hours), subacute (hours to days), and chronic (days to months) phases need to be developed [Fagan SC et al. Stroke 2004]. Inhibition of proteases, free radicals and inflammatory cytokines (to name a few) have been shown to be effective for vascular protection after stroke in experimental models. In addition, signaling molecules and NADPH and xanthine oxidase pathways that are involved in vascular injury may be putative targets for vascular protection, stated Rhian M. Touyz, MD, University of Ottawa, Canada.

The editors would like to thank the many members of the 2009 International Stroke Conference presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.