

Summary
Despite ongoing challenges in the management of acute coronary syndrome (ACS), researchers have made considerable advances in the treatment of patients with non-ST-segment elevation myocardial infarction (NSTEMI) and in those with ST-segment elevation myocardial infarction (STEMI). This article highlights some of the most important ACS research findings from 2008 and described ongoing trials that will expand our understanding of optimal patient management.
- thrombotic disorders
- myocardial infarction
Despite ongoing challenges in the management of acute coronary syndrome (ACS), researchers have made considerable advances in the treatment of patients with non-ST-segment elevation myocardial infarction (NSTEMI) and in those with ST-segment elevation myocardial infarction (STEMI). In this session, presenters highlighted some of the most important ACS research findings from 2008 and described ongoing trials that will expand our understanding of optimal patient management.
Advances in STEMI Management
Paul W. Armstrong, MD, University of Alberta, Edmonton, Alberta, Canada, described the implications of several recent studies that have investigated the clinical utility of pharmacoinvasive reperfusion therapy. For example, the FAST-MI (French Registry on Acute ST-elevation Myocardial Infarction) trial emphasized the importance of early fibrinolysis in followed by routine angiography and a liberal use of percutaneous coronary intervention (PCI) [Danchin N et al. Circulation 2008]. This pharmacoinvasive approach achieved similar results to primary PCI (PPCI) in FAST-MI, whereas, prior studies of fibrinolytic therapy alone had demonstrated higher rates of reinfarction, intracranial hemmorrhage and a trend toward higher mortality, compared with PPCI. In contrast, to the findings for FAST-MI the ASSENT-4 PCI (Assessment of the Safety and Efficacy of a New Treatment Strategy for Acute Myocardial Infarction) trial, had shown that a fibrinolysis-facilitated PCI strategy was harmful in patients who presented later than 3 hours from symptom onset [McDonald MA et al. Eur Heart J 2008], thus underscoring the need for further research to identify the optimal role for a pharmacoinvasive approach.
The FINESSE (Facilitated Intervention with Enhanced Reperfusion Speed to Stop Events) trial was designed to evaluate whether PCI that was facilitated with abciximab and reduced-dose reteplase or abciximab alone would be more effective than primary PCI in which abciximab was administered immediately before the procedure in the catheterization laboratory. In this trial, neither abciximab alone nor in combination with reteplase that was given to facilitate PCI improved clinical outcomes compared with abciximab that was administered at the time of PCI [Ellis SG et al. N Engl J Med 2008].
Future trials will evaluate the optimal approach for managing STEMI patients who present less than 3 hours from symptom onset but who cannot reliably undergo primary PCI in less than 60 minutes. In the STREAM (Strategic Reperfusion Early After Myocardial Infarction; NCT00623623) trial, approximately 2000 prehospital patients seen within 3 hours of symptom onset will be randomly assigned to an early (prehospital) strategy of lysis with tenecteplase or to primary PCI. The STREAM trial began in 2008 and is anticipated to be completed in 2010.
Advances in the Pharmacological Treatment of Atherothrombosis
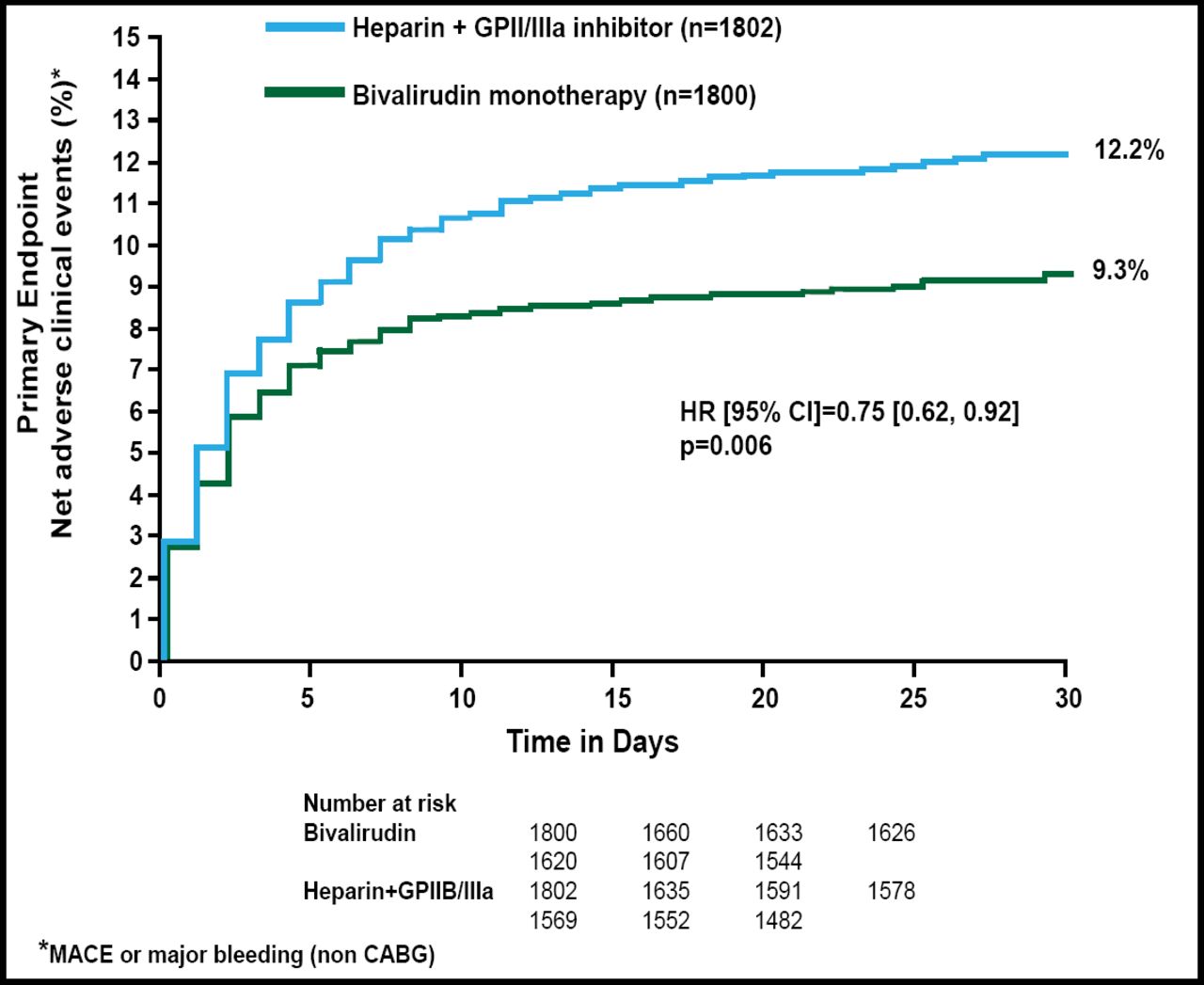
Stefan James, MD, PhD, Uppsala University Hospital, Uppsala, Sweden, discussed recent developments in the pharmacological treatment of atherothrombosis. One of the most important trials that examined the ideal use of currently available antithrombotic therapy was the HORIZONS-AMI (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction) trial. In HORIZONS-AMI, anticoagulation with bivalirudin alone, as compared with heparin plus glycoprotein IIb/IIIa inhibitors (abciximab or eptifibatide), significantly reduced 30-day rates of major bleeding and net adverse clinical events in STEMI patients undergoing primary PCI (HR, 0.75; 95% CI, 0.62 to 0.92; p=0.006; Figure 1) [Stone GW et al. N Engl J Med 2008].
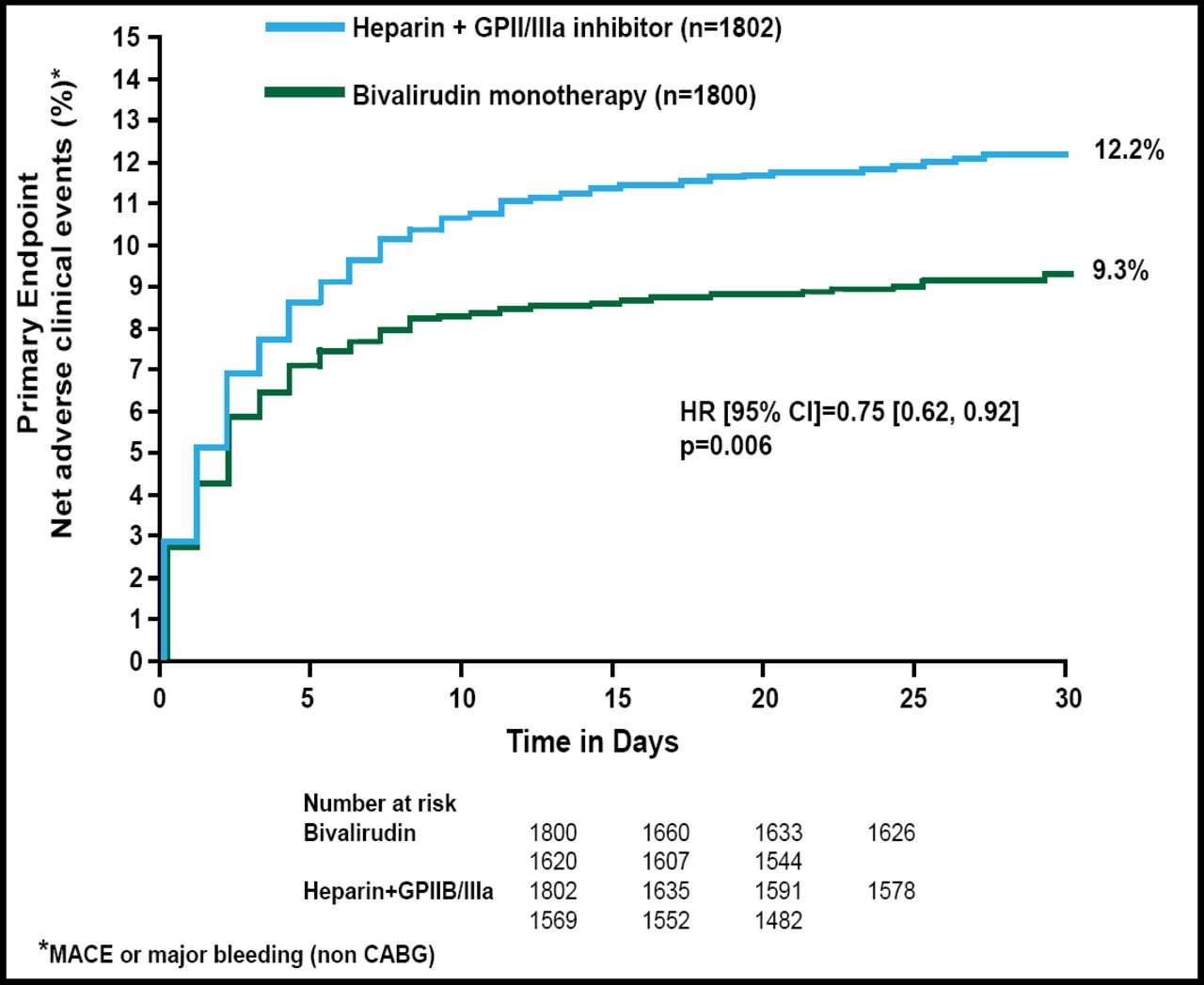
Bivalirudin Monotherapy in Primary PCI.
Copyright © 2008 Massachusetts Medical Society. All rights reserved.
In contrast with standard therapy (aspirin, clopidogrel, heparin, glycoprotein IIb/IIIa inhibitors), new treatment options include more potent oral antiplatelet agents that have superior efficacy but increase bleeding rates, as well as intravenous and subcutaneous anticoagulants that have similar efficacy but lower bleeding rates, Dr. James said. For example, compared with standard clopidogrel, intensive antiplatelet therapy with the novel thienopyridine prasugrel reduced the risk of ischemic events, including stent thrombosis, regardless of stent type in TRITON-TIMI 38 (Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel - Thrombolysis in Myocardial Infarction 38) [Wiviott SD et al. Lancet 2008].
In addition to prasugrel, several new antiplatelet agents and anticoagulants have shown promising benefits in phase 2 and 3 trials in patients with ACS, Dr. James said. These include:
-
Ticagrelor, an oral P2Y12 antagonist
-
Cangrelor, an intravenous P2Y12 antagonist
-
Rivaroxaban, an oral factor Xa inhibitor
-
Apixaban, an oral factor Xa inhibitor
-
Dabigatran, an oral thrombin inhibitor
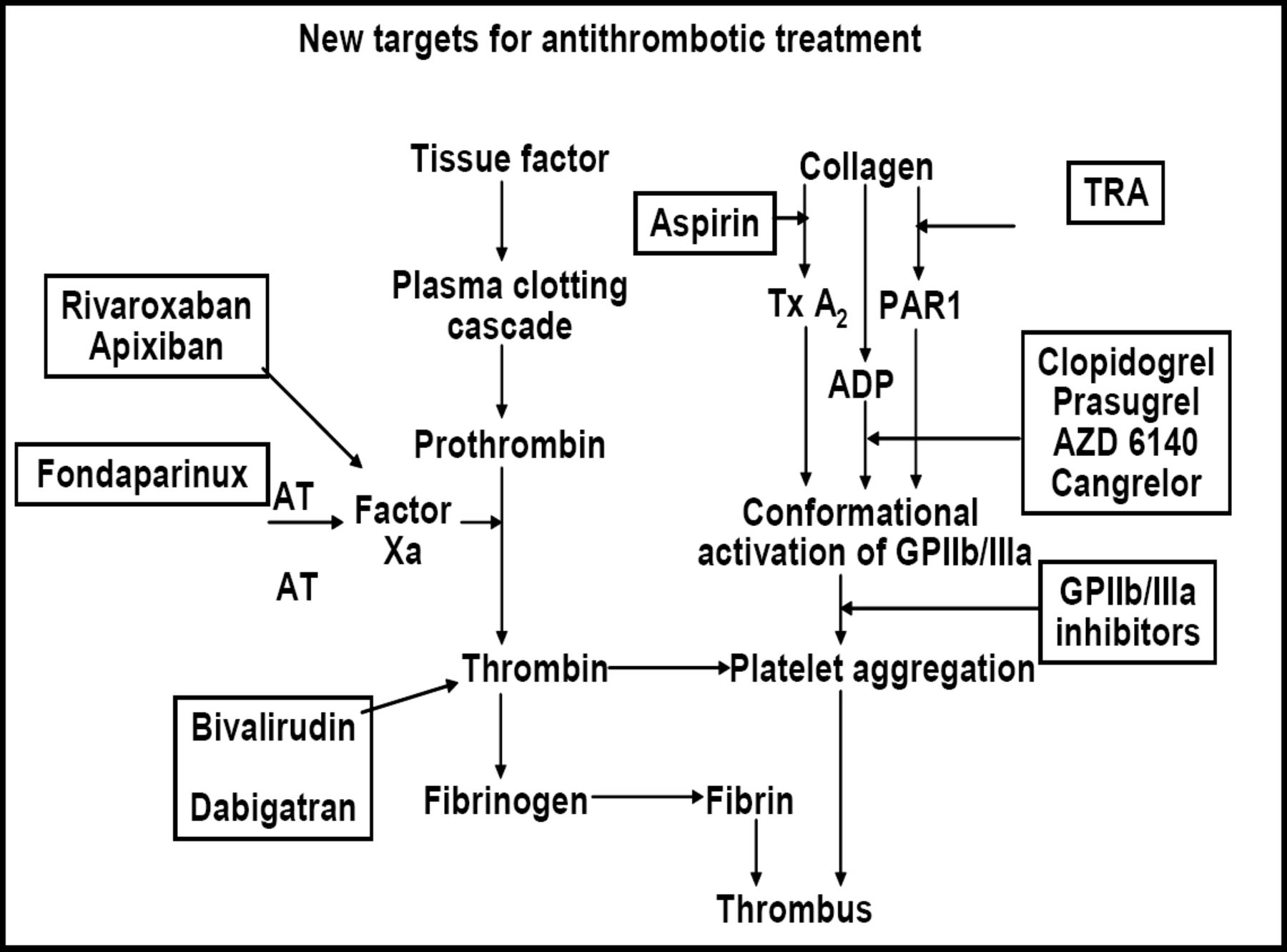
Another oral agent, SCH 530348, is a selective thrombin receptor antagonist (TRA) that exerts potent antithrombotic effects without increasing bleeding when added to standard antiplatelet therapy in patients undergoing PCI. The phase 3 TRA-CER (Trial to Assess the Effects of SCH 530348 in Preventing Heart Attack and Stroke in Patients With Acute Coronary Syndrome; NCT00527943) study will evaluate TRA that is added to antiplatelet therapy in approximately 10,000 patients with ACS. The phase 3 TRA 2P-TIMI 50 trial (Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events; NCT00526474) will compare antiplatelet therapy with or without TRA in 19,500 patients with established peripheral artery disease or a history of MI or stroke (Figure 2).
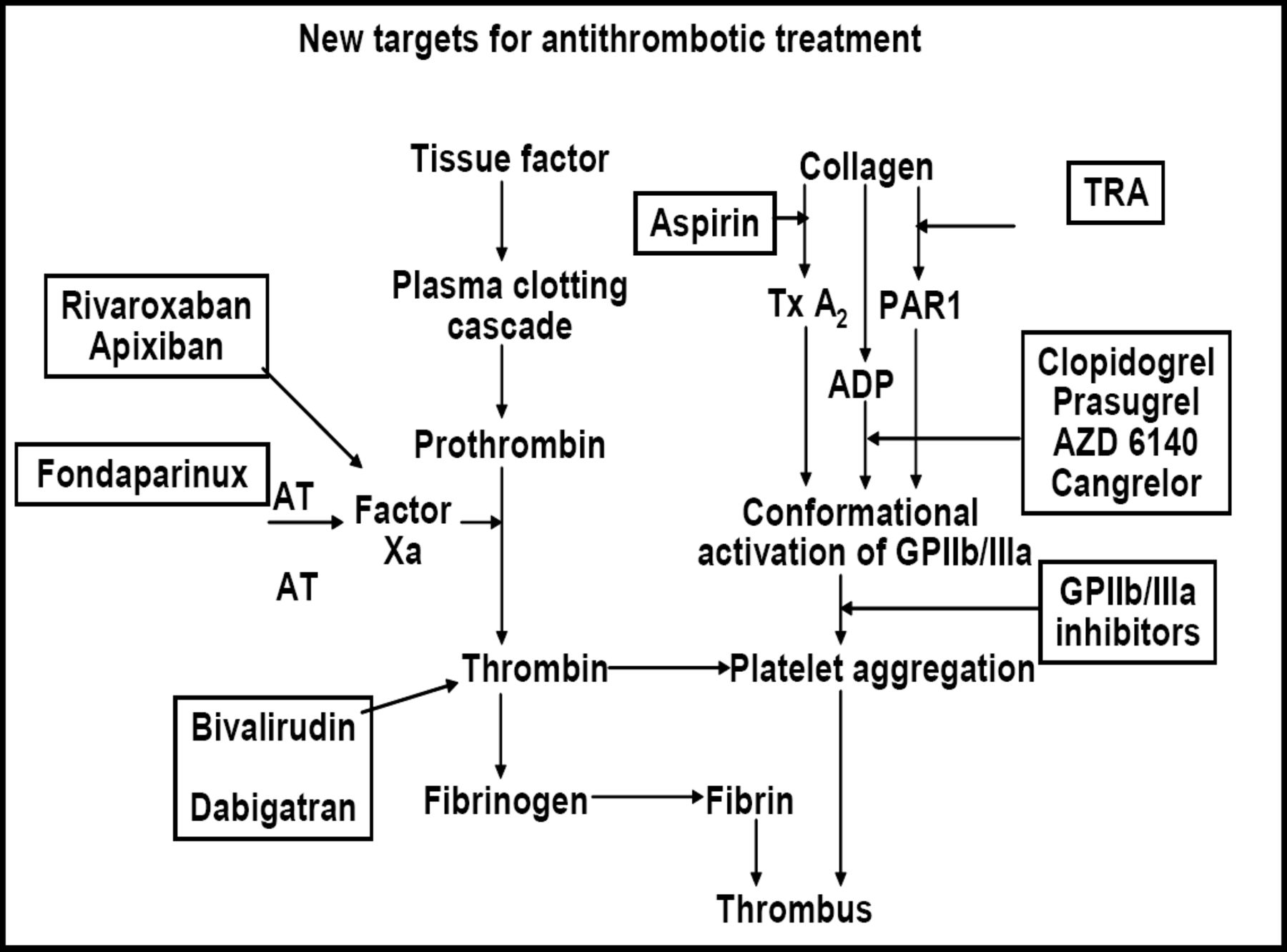
New Targets for Antithrombotic Treatment.
Future research will evaluate combination regimens with the goal of further controlling bleeding rates to allow broader use in clinical practice, Dr. James said. In addition, more trials may examine the utility of individualized therapy based on the risk of bleeding, as assessed by pretreatment platelet and coagulation activity.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.