

Summary
The global impact of stroke is significant both in terms of death (5.5 million annually) and disability (5 million individuals annually) [World Health Organization. The Atlas of Heart Disease and Stroke 2004]. The presence of atrial fibrillation (AF) increases the risk of stroke approximately 5-fold, and increasing age is associated with an increase in risk (1.5% in the 50–59-year age group vs 23.5% in the 80–89-year age group) [Wolf PA et al. Stroke 1991]. Current projections are that by 2020, approximately 9 million individuals in the Unites States alone will be diagnosed with AF [Miyasaka Y et al. Circulation 2006].
- arrhythmias
The global impact of stroke is significant both in terms of death (5.5 million annually) and disability (5 million individuals annually) [World Health Organization. The Atlas of Heart Disease and Stroke 2004]. The presence of atrial fibrillation (AF) increases the risk of stroke approximately 5-fold, and increasing age is associated with an increase in risk (1.5% in the 50–59-year age group vs 23.5% in the 80–89-year age group) [Wolf PA et al. Stroke 1991]. Current projections are that by 2020, approximately 9 million individuals in the Unites States alone will be diagnosed with AF [Miyasaka Y et al. Circulation 2006].
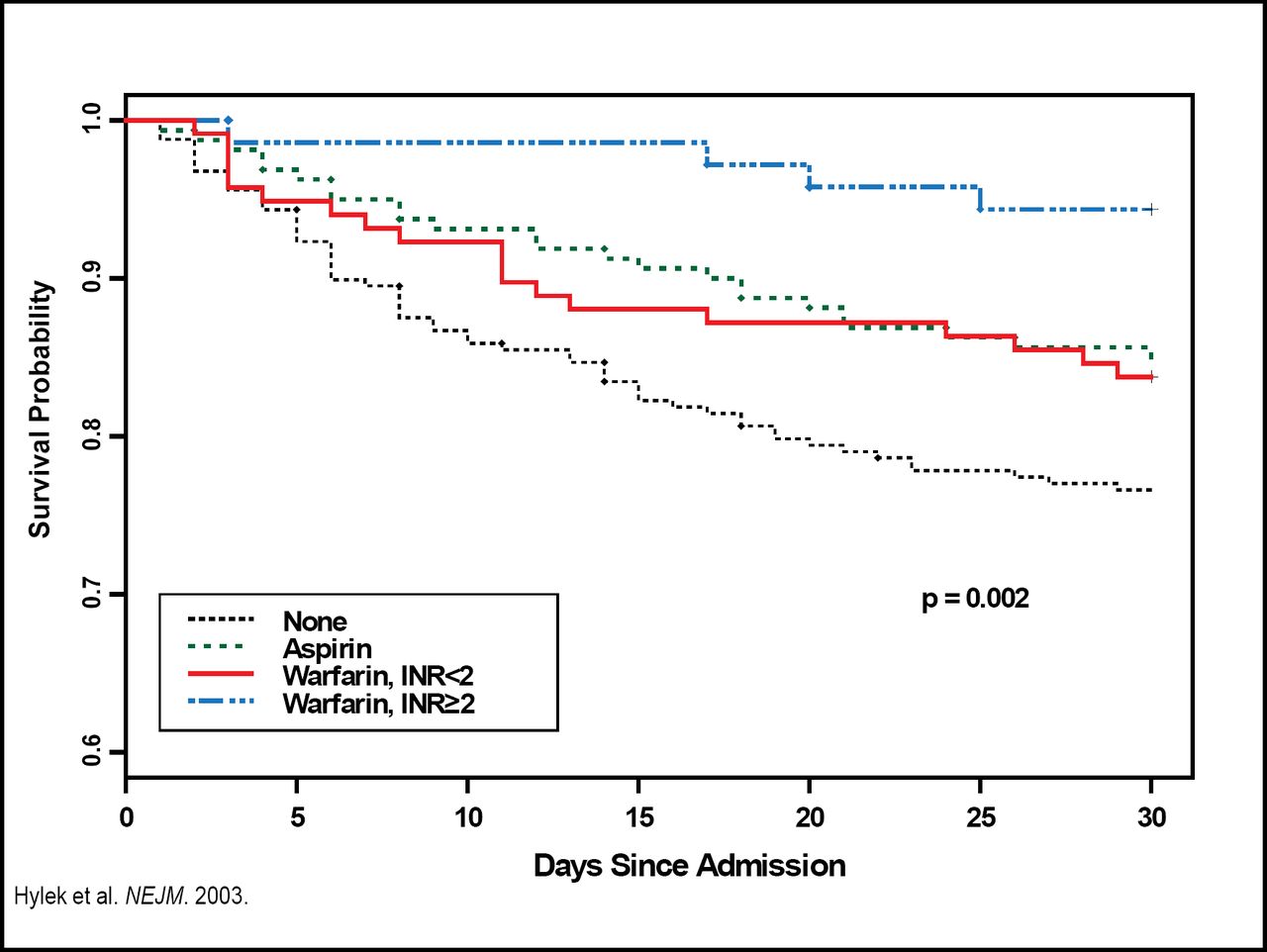
Warfarin is highly effective in preventing stroke in patients with AF. It also has been shown that in patients with AF, treatment with warfarin that results in an international normalized ratio (INR) ≥2.0 reduces the frequency, severity, and risk of death from ischemic stroke (Figure 1) [Hylek EM et al. N Engl J Med 2003]. “Despite its proven success, warfarin is underutilized,” said Elaine M. Hylek, MD, Boston University School of Medicine, Boston, MA [Waldo AL et al. J Am Col Cardiol 2005].
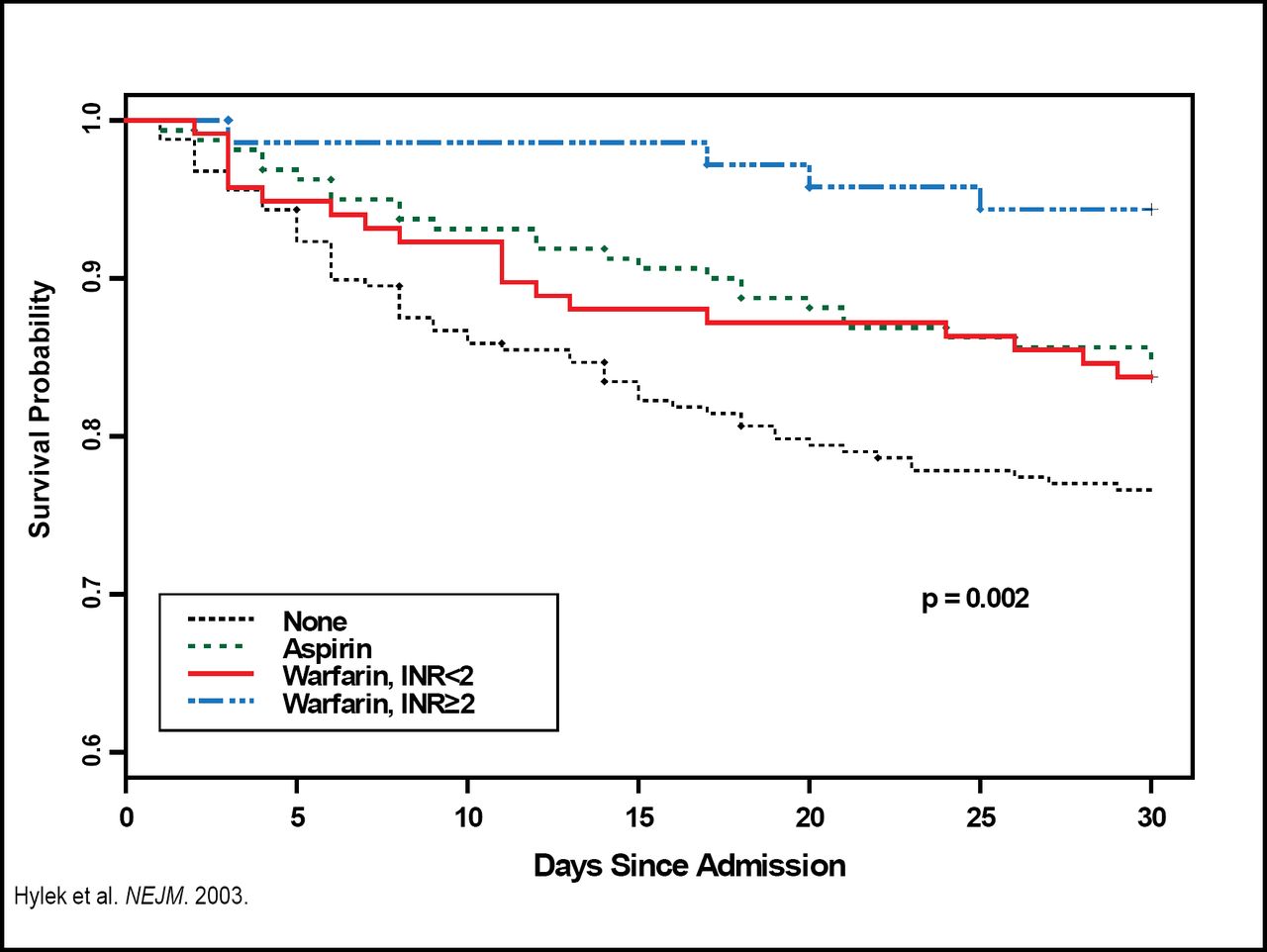
Kaplan-Meier Estimates of Survival in the 30 Days After an Ischemic Stroke Among Patients With Nonvalvular AF, According to Antithrombotic Medication Status at Admission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
Dr. Hylek cited several factors that were associated with decreased use of warfarin, including older age (≥80 years), perceived bleeding risk, and the innate difficulties with warfarin. We know that the optimal INR target for warfarin is 2 to 3; however, response to warfarin is affected by numerous factors, including drug interference, dietary vitamin K, comorbid disease states, and gender, all of which need to be considered. Dr. Hylek emphasized that major bleeding can be decreased through intensive efforts to optimize anticoagulant therapy and that vigilant blood pressure control (to 130/80 mm Hg) has been shown to decrease both ischemic and hemorrhagic stroke.
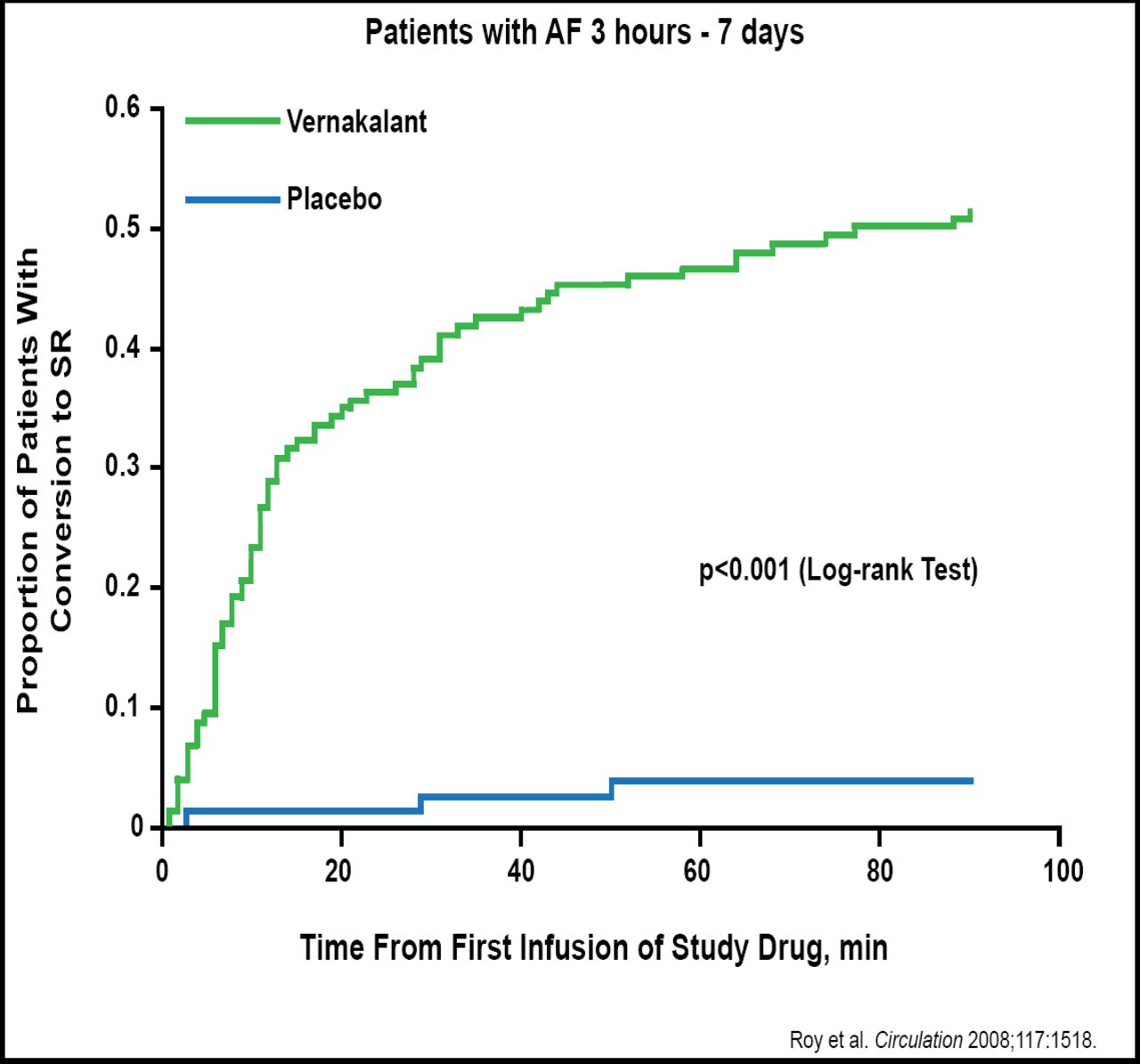
Richard L. Page, MD, University of Washington, Seattle, WA, discussed recent trials that have evaluated medical therapy options for AF, including one that showed that the investigational compound vernakalant hydrochloride, can rapidly convert short-duration AF (3 hours to 7 days) to sinus rhythm. In that study, 51.7% (75/145) of vernakalant-treated patients converted to sinus rhythm within 90 minutes (median time, 11 minutes) versus 4% (3/75) of the placebo patients (p<0.001; Figure 2) [Roy D et al. Circulation 2008].
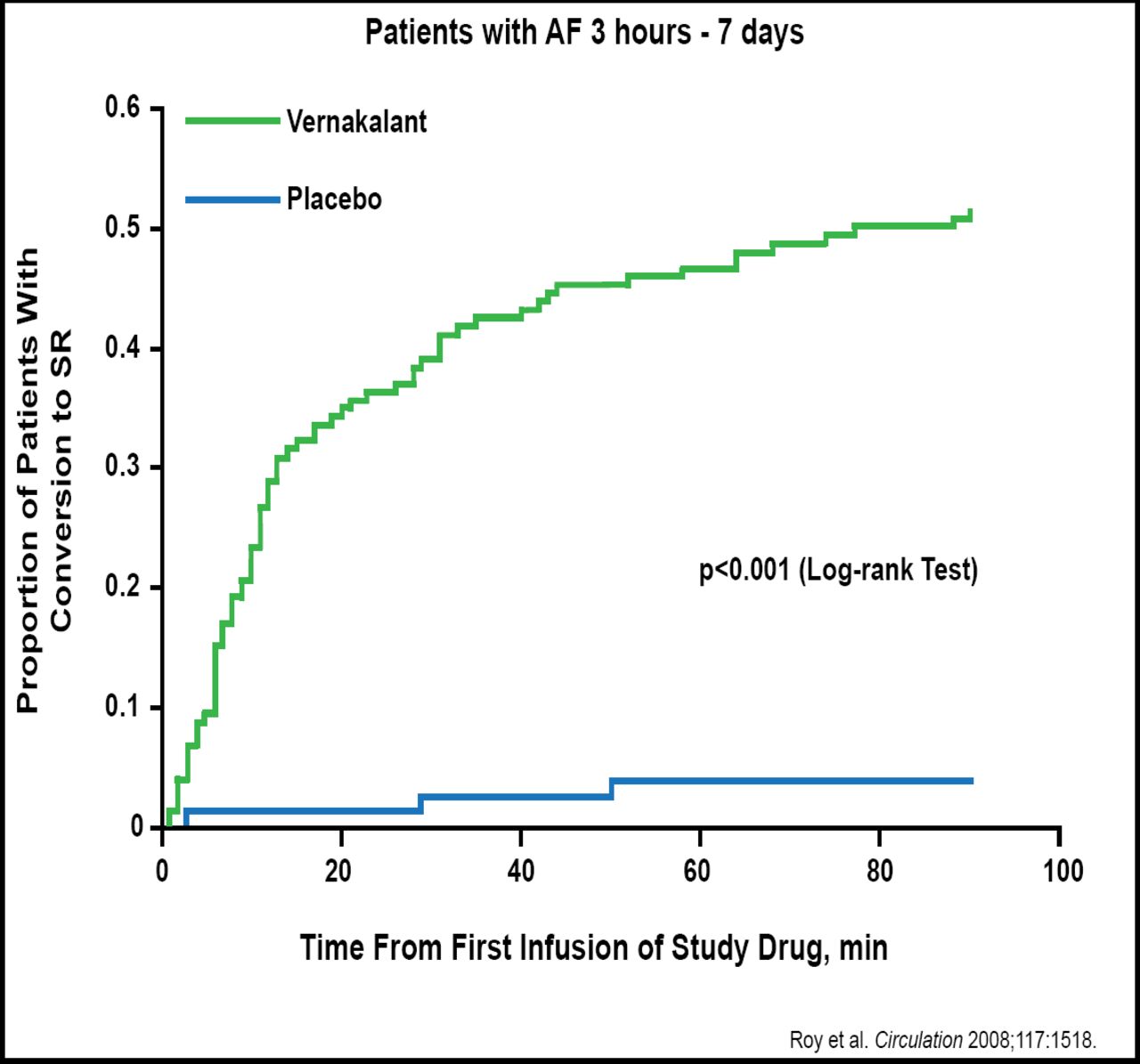
Time Course to Conversion of AF.
Copyright © 2008 Wolters Kluwer. All rights reserved.
Proving that the debate between rhythm versus rate control of AF continues, Dr. Page reviewed results from a study that directly compared rhythm control (primarily amiodarone) versus rate control (primarily beta-blockers or digoxin) in subjects with AF and congestive heart failure, which found both treatments to be equally effective [Roy D et al. N Engl J Med 2008].
According to Dr. Page, new hope for improved outcomes in patients with paroxysmal/persistent AF may come from a trial of rhythm control using dronedarone (400 mg/day), which showed that after 21 months, there was a clinically significant reduction in primary study outcome of time to first cardiovascular hospitalization or death (HR, 0.76; p<0.001) [AHA Scientific Sessions 2008; Abstract 1327].
“Even in light of promising new medical therapies, total prevention of AF with antiarrhythmics is unlikely,” said Gerald V. Naccarelli, MD, Penn State University College of Medicine, Hershey, PA. “Thus, there is still a need for catheter ablation.”
Several approaches can be taken with AF catheter ablation: isolation of the triggers and perpetuating re-entrant circuits that are located in the pulmonary veins (PVs); disruption of the substrate for perpetuating rotors in the antra of the PVs; disruption of the putative dominant rotors in the left and right atria; and targeted ablation of ganglionated autonomic plexi in the epicardial fat pads.
Patients with symptomatic paroxysmal AF, with no structural heart disease, who are aged under 70 years, and have a left atrial diameter <5.0 cm who have failed treatment with antiarrhythmic drugs appear to be the best candidates for AF ablation. Dr. Naccarelli concluded by pointing out that AF ablation techniques need to be standardized and that FDA approval is required for catheters and procedures. More comparison efficacy studies, as well as long-term follow-up studies to measure adverse events and recurrence rates, also are needed.
Eric N. Prystowsky, MD, St. Vincent's Hospital, Indianapolis, IN, stressed that although the data seem to indicate no survival differences between a rate or rhythm approach, there are conditions that favor rhythm over rate control. These include the continuation of substantial symptoms during rate control, younger patients who face decades of AF, and patients who are predisposed to left ventricular diastolic dysfunction.
While not in favor of using catheter ablation routinely as first-line therapy, he suggested that in the case of younger patients for whom the only remaining medical therapy is amiodarone, catheter ablation probably is preferred over 10 to 15 years of amiodarone therapy.
Dr. Prystowsky stressed that the prime directive for the management of AF is to preserve the brain. He agreed with Dr. Hylek on the importance of the CHADS2 scores, and he also stressed that ACC/AHA/ESC guidelines be followed when therapies that aim to maintain sinus rhythm are considered.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.