

Summary
Early intensive glucose-lowering provides long-term protection against major diabetes outcomes as well as myocardial infarction and all-cause mortality, according to new 10-year follow-up data from the United Kingdom Prospective Diabetes Study (UKPDS). However, the benefits of tighter blood pressure control that were observed in 1997 were not maintained in the 2007 analysis of UKPDS.
- endocrinology
- diabetes & endocrinology clinical trials
- diabetes mellitus
- hypertensive disease
Early intensive glucose-lowering provides long-term protection against major diabetes outcomes as well as myocardial infarction (MI) and all-cause mortality, according to new 10-year follow-up data from the United Kingdom Prospective Diabetes Study (UKPDS). However, the benefits of tighter blood pressure control that were observed in 1997 were not maintained in the 2007 analysis of UKPDS.
The newest UKPDS (ISRCTN75451837) findings represent 30 years of data, including 20 years of active intervention and 10 years of post-trial follow-up data. UKPDS researchers Rury R. Holman, FRCP, and David R. Matthews, DPhil, Oxford Centre for Diabetes, Endocrinology, and Metabolism, Oxford, UK, presented the follow-up findings exactly 10 years to the day after the initial UKPDS findings were reported at the 1998 EASD meeting in Barcelona, Spain. Results also were published online in the New England Journal of Medicine (www.nejm.org; DOI: 10.1056/NEJMoa0806359; DOI: 10.1056/NEJMoa0806470).
Glucose Control
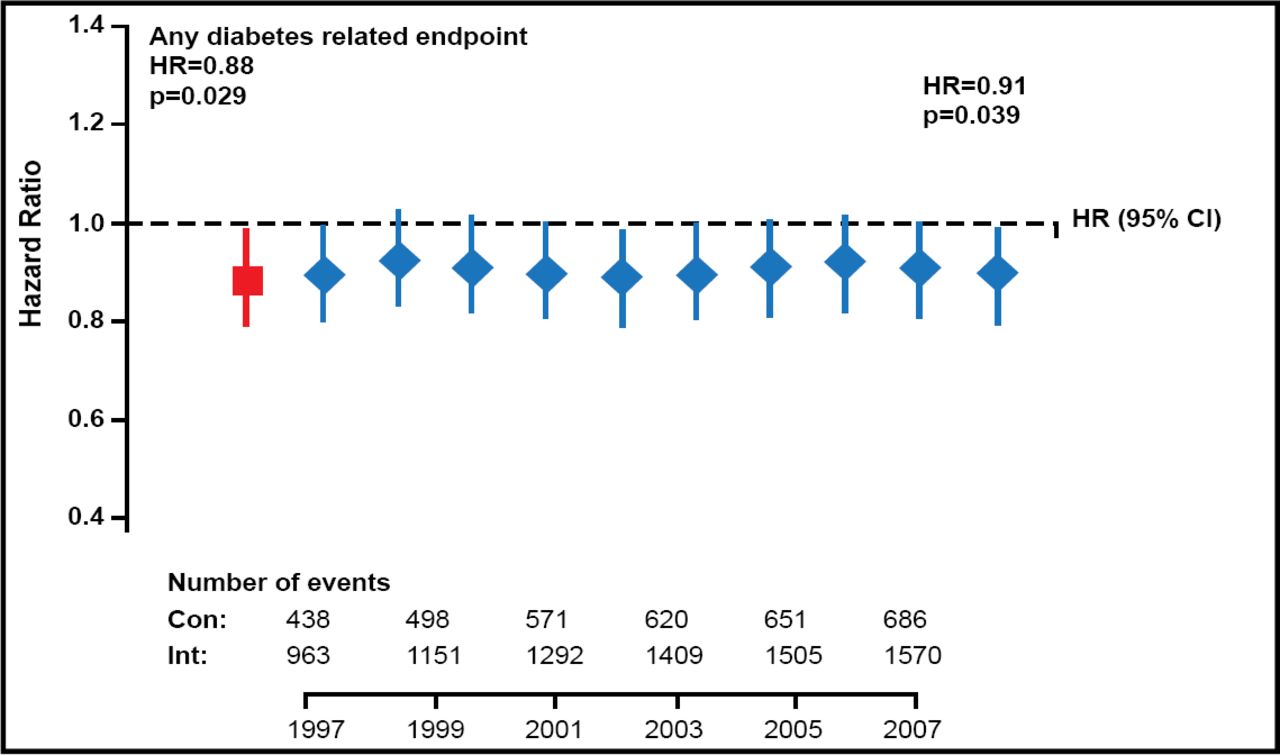
Between 1977 and 1991, UKPDS randomly assigned patients with newly diagnosed type 2 diabetes mellitus (T2DM) to intensive glucose-lowering with sulfonylurea or insulin treatment (n=2729) or conventional glucose control through diet (n=1138). Compared with conventional treatment, intensive glucose control reduced the risk of major diabetes outcomes by 12% in the 1997 analysis (p=0.029) and by 9% in 2007 (p=0.040; Figure 1). Intensive glucose control also reduced the risk of microvascular disease by 25% in 1997 (p=0.0099) and by 24% in 2007 (p=0.001).

Long-Term Effects of Early Intensive Glucose-Lowering.
Two additional benefits that are related to intensive glucose control have emerged with longer follow-up. Regarding MI, the relative risk reduction (RRR) that was observed in 1997 (RRR=16%; p=0.052) became statistically significant by 2007 (RRR=15%; p=0.01). In addition, although no effect on all-cause mortality was observed in 1997 (p=0.44), a statistically significant mortality benefit in favor of intensive therapy emerged by 2007 (RRR=13%; p=0.007).
Blood Pressure Control
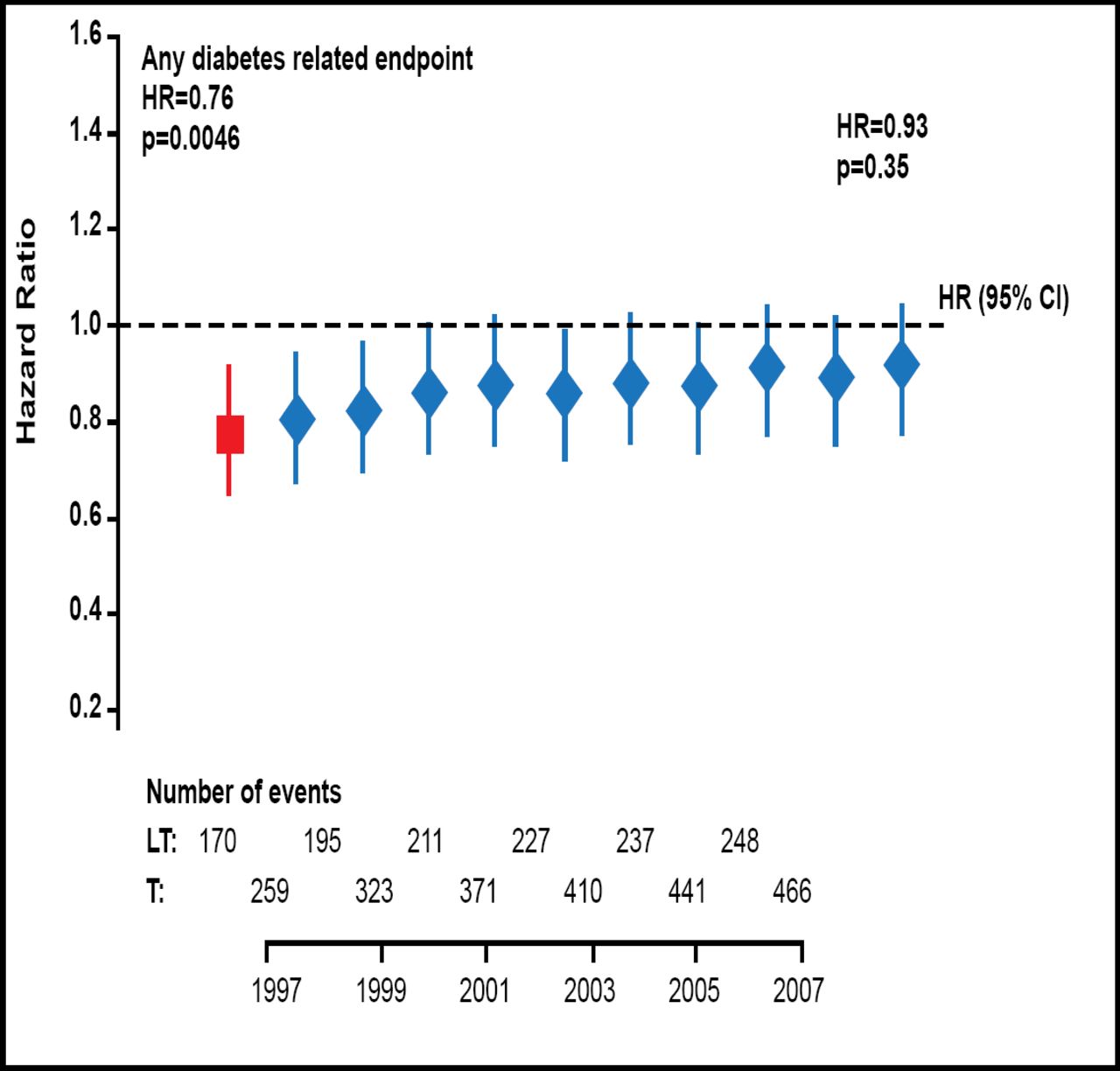
In the UKPDS blood pressure factorial study, 1448 patients with T2DM and hypertension were randomly assigned to tight blood pressure control with an angiotensin-converting enzyme (ACE) inhibitor and a beta-blocker, or to less aggressive blood pressure control with any pharmacologic intervention except ACE inhibitor or beta-blocker therapy. Of these patients, 884 continued with post-trial monitoring.
In the 1997 analysis of UKPDS data, tight blood pressure control reduced the risk of any diabetes-related endpoint by 24% versus less aggressive control (p=0.005); this benefit was lost by 2007 (Figure 2). Similarly, the protection against microvascular disease that was shown in 1997 (HR=0.63; p=0.0092) faded in the 2007 analysis (HR=0.84; p=0.020). Blood pressure control did not appear to affect the risk of MI or all-cause mortality at any time point.

Tight Blood Pressure Control and Diabetes-Related Outcomes.
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.