

Summary
For patients with comorbid medical conditions, knowledge of drug metabolism is important and may in fact be critical in the oncology setting. A case in point is the widespread use of the anti-estrogen compound tamoxifen, which acts via estrogen receptor modulation. Unfortunately, one of the more common adverse events that occur with this drug is hot flashes, a condition that is uncomfortable to the point of discouraging long-term treatment adherence. An attempt to resolve this discomfort may result in additional unforeseen risk.
- mood disorders
- breast cancer
For patients with comorbid medical conditions, knowledge of drug metabolism is important and may in fact be critical in the oncology setting. “As physicians, we need to know everything about our patients that we can,” said David Flockhart, MD, PhD, Indiana University School of Medicine, Indianapolis, IN. At the very least, it is important to know what medications they are currently taking.
A case in point is the widespread use of the anti-estrogen compound tamoxifen, which acts via estrogen receptor (ER) modulation. Tamoxifen is highly effective in the prevention of breast cancer in ER-positive women and is used both as adjuvant therapy against cancer recurrence and as a prevention measure for those who are considered to be at high risk for disease. Unfortunately, one of the more common adverse events that occur with this drug is hot flashes, a condition that is uncomfortable to the point of discouraging long-term treatment adherence. An attempt to resolve this discomfort may result in additional unforeseen risk.
To illustrate this point, Dr. Flockhart presented a case report of a 45-year-old woman with tamoxifen-related hot flashes and comorbid depression who was prescribed paroxetine. Within a week, the hot flashes resolved; the hot flashes resumed when she was taken off paroxetine. “Now, paroxetine's effect on depression takes much longer than a week, so there's something else going on here.” The working hypothesis was that paroxetine had somehow interfered with the anti-estrogen activity of tamoxifen, either by preventing absorption, which seemed unlikely, or by altering the transformation of tamoxifen into its active metabolite, endoxifen. “We were lucky to have chromatograms of this woman before and after peroxetine administration,” said Dr. Flockhart, and analysis of these data showed an obvious decrease in endoxifen concentrations. “We were very interested in this. There is some sort of decreased activity in this woman when she's taking paroxetine.”
Cytochrome P450 enzyme activity was the most likely suspect—specifically, subtype CYP2D6, a site of metabolism for multiple commonly prescribed drugs. Prior investigations confirm that paroxetine inhibits this enzyme, but the extent and therapeutic impact of inhibition are unclear. In a small study of 12 women with tamoxifen-induced hot flashes, Dr. Flockhart, using a combination of serum concentration and genetic analysis, was able to determine that the effect of paroxetine/CYP2D6 downregulation was so pronounced, it nearly matched the lack of activity seen in women who had a mutant, non-functioning form of the enzyme [J Natl Cancer Inst 2003].
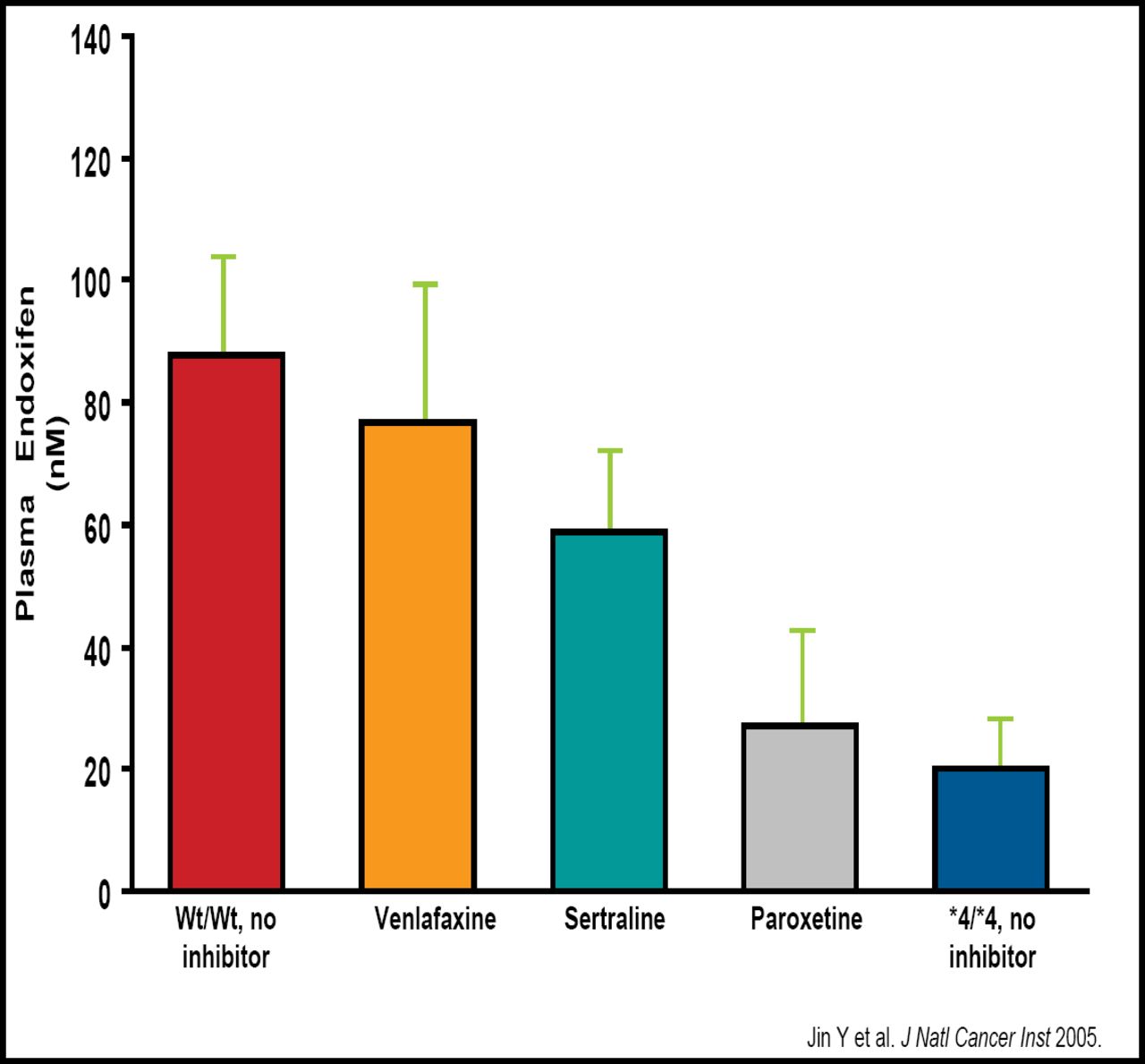
This observation was cause for great concern. An estimated 30% of tamoxifen-treated patients are prescribed antidepressants for depression or hot flashes. Were other SSRIs placing them at risk? One answer came from Jin et al, who investigated the plasma concentrations of endoxifen in patients who were concomitantly using one of 3 different SSRIs. Inhibition of the CYP2D6 enzyme was determined and ranked as follows: paroxetine > sertraline > venlafaxine [J Natl Cancer Inst 2005].
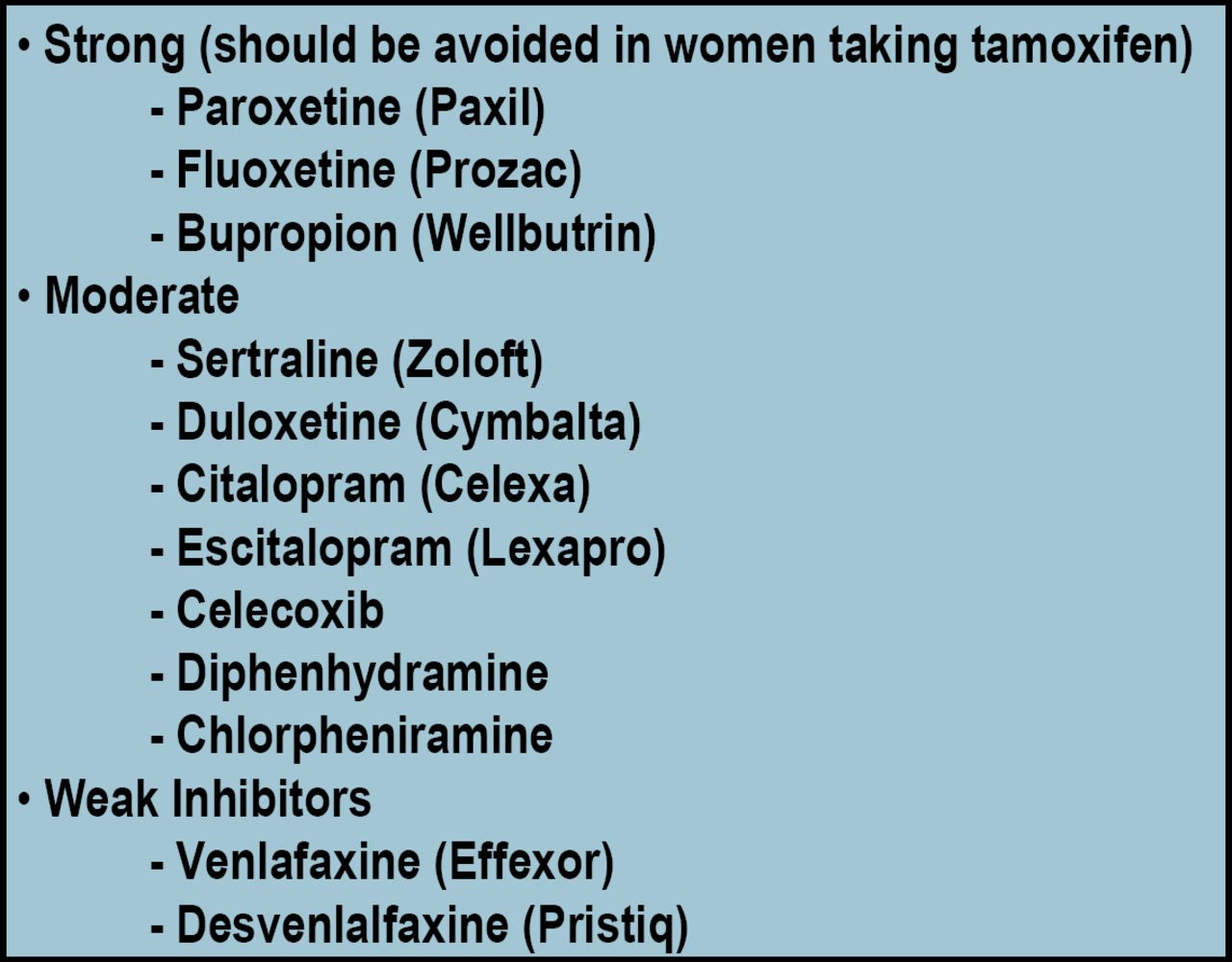
Commenting on these results, Dr. Flockhart noted that venlafaxine can be effectively used to treat tamoxifen-related hot flashes while retaining tamoxifen protection. “This can improve compliance with this very effective medication” and thereby have a direct impact on long-term survival. Other investigators have carried these observations forward, and there is now consensus that the following agents are potent inhibitors of CYP2D6 and should not be prescribed with tamoxifen: bupropion, fluoxetine, and paroxetine (Figures 1 and 2).
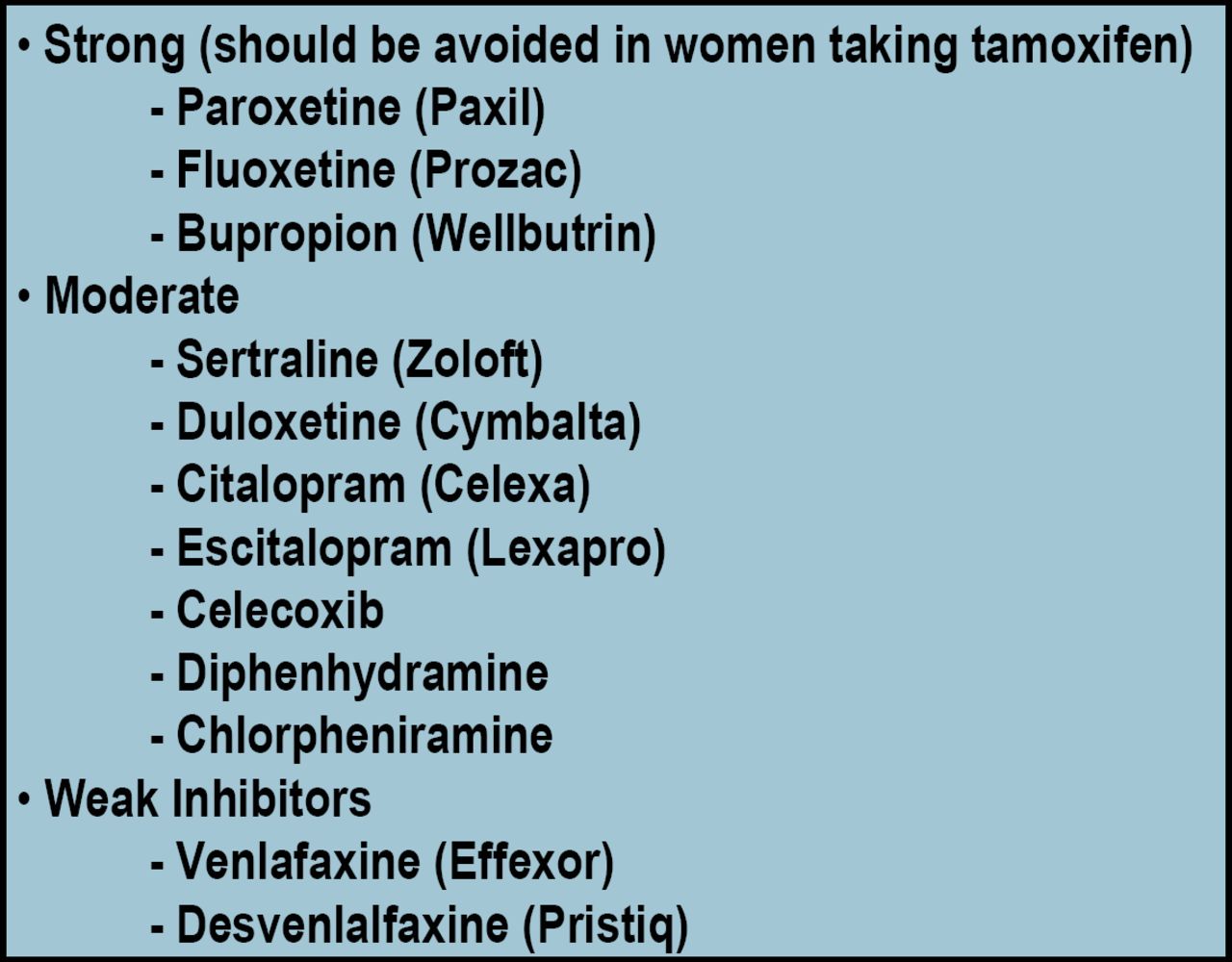
Partial List of Common CYP2D6 Inhibitors.
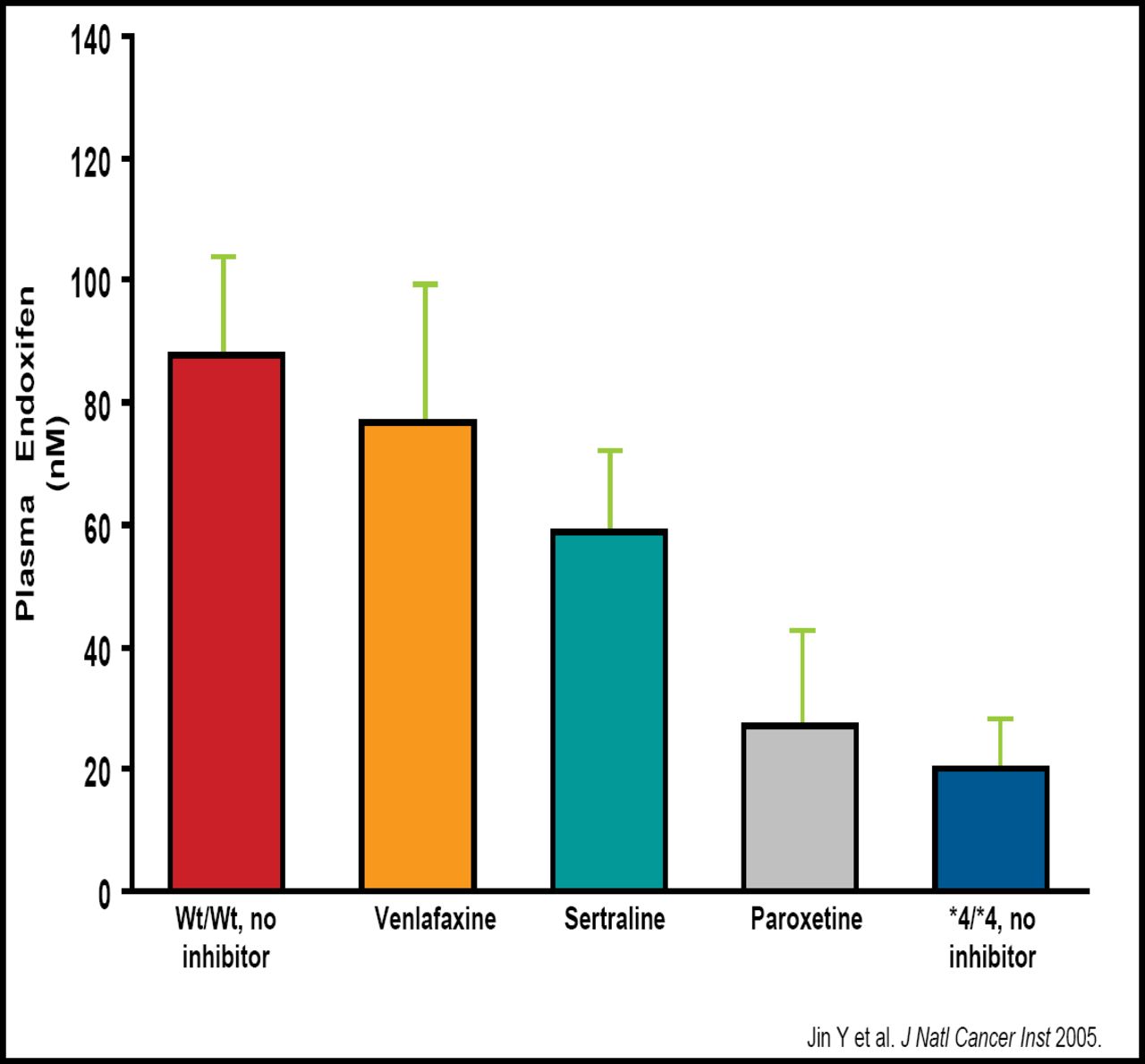
Inhibition of CYP2D6 Affects Endoxifen Concentrations.
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.