

Summary
The prevalence of diabetes has grown at a rapid pace across the world, particularly in the United States. The World Health Organization estimates that the number of people with diabetes will grow globally from 171 million in 2000 to approximately 366 million in 2030 [Wild et al. Diabetes Care 2004], paralleling the global rise in obesity. This article discusses what these trends mean for stroke prevention and vascular health.
- cerebrovascular disease
- prevention & screening
- diabetes mellitus
The prevalence of diabetes has grown at a rapid pace across the world, particularly in the United States. The World Health Organization estimates that the number of people with diabetes will grow globally from 171 million in 2000 to approximately 366 million in 2030 (Wild et al. Diabetes Care 2004), paralleling the global rise in obesity. A panel of experts shared their thoughts on what these trends mean for stroke prevention and vascular health. David Tanne, MD, University of Tel Aviv, Tel Aviv, Israel, gave an overview of diabetes and the risk of stroke. In the Israeli Ischemic Heart Disease study of approximately 10,000 Israeli civil servants and municipal employees, the presence of diabetes at baseline led to a doubling of stroke risk after 20 years (hazard ratio=1.9; 95% CI 1.2–2.9; Tanne et al. Circulation 1998). Similar rates were reported in the Bezafibrate Infarction Prevention registry of 15,000 coronary heart disease patients who were followed for 6–8 years (HR=1.9; 95% CI 1.6.2.4; Tanne et al. Circulation 2001). The risks in blacks are even more pronounced, with even younger people (35–44 years) having a relative risk of 9.9 for stroke if they have diabetes (Kissela et al. Diabetes Care 2005). Across multiple longitudinal studies in various populations, the relative risk of stroke is 2–4 times higher than in patients without diabetes.
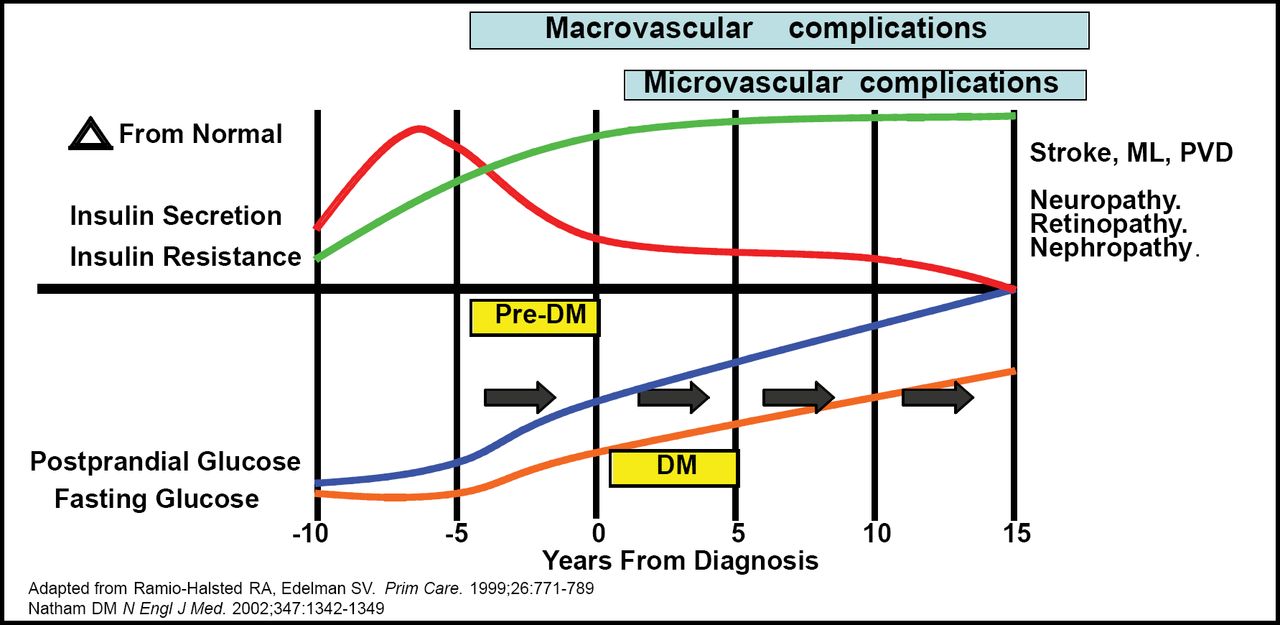
Insulin resistance is responsible for 95% of all types of diabetes. A complicated, interrelated series of mechanisms are implicated in the progression from hyperglycemia to atherosclerosis. Pierre Fayad, MD, University of Nebraska, Omaha, NE, reviewed the pathophysiology of impaired glucose metabolism and its relationship to vascular disease. The evolution of hyperglycemia and the resulting implications over time are presented in Figure 1. “The macrovascular complications span the whole spectrum from pre-diabetes to the full diabetic state, in association with resistance to insulin,” noted Dr. Fayad, “while microvascular complications appear restricted to the full diabetic phase primarily.” Factors responsible for the development of the pathologic vascular changes include inflammation, endothelial dysfunction, dyslipidemia, glycation, hypertension, oxidative stress, hypercoagulability, visceral obesity, and increases in protein kinase C and aldose reductase. “All of these factors and pathways additionally interact amongst each other, producing a very complex picture at the heart of the vascular pathology of diabetes and insulin resistance,” commented Dr. Fayad.

Evolution of Type 2 Diabetes.
Askiel Bruno, MD, Indiana University, Indianapolis, IN, discussed the management of hyperglycemia in patients with acute stroke. Preclinical acute stroke models have demonstrated that hyperglycemia results in larger infarctions and worse outcomes. The therapeutic window, optimal glucose target, and the primary mechanisms of harmful effects of glucose elevation are not well characterized. Potential harmful effects include tissue acidosis, free radical damage, excitotoxicity, accumulation of intracellular calcium, blood brain barrier permeability, brain edema, hemorrhagic infarct conversion, impaired reperfusion, and hypercoagulability. Dr. Bruno was careful to point out that not all stroke subtypes respond to hyperglycemia in the same way. In the Trial of ORG 10172 in Acute Stroke Treatment (TOAST), patients with lacunar strokes (n=304) had better outcomes with higher levels of blood glucose (Bruno et al. Neurology 1999). This is supported by data from a more recent study by Uyttenboogaart et al (Brain 2007), in which those with lacunar strokes had significantly better outcomes if blood glucose was >144 mg/dL (p=0.048). Clinical response to reperfusion is also affected by hyperglycemia. When reperfusion occurred early in patients with hyperglycemia, the potential for harm was higher than when reperfusion was delayed or did not occur (Alvarez et al. Stroke 2004).
The results of the Glucose Insulin in Stroke (GIST-UK) trial were published in 2007. In this study, patients were randomized to receive either IV insulin or saline. The majority of the patients (83%) was non-diabetic with a median glucose admission of 139 mg/dL. The study was stopped early due to slow enrollment, and the primary result (mortality) did not reach statistical significance (Gray et al. Lancet Neurology 2007). The difference in glucose between the 2 treatment groups was only 10 mg/dL, and mean treatment initiation time was 13 hours, which may have been too late. “These factors may have led to the trial being neutral,” said Dr. Bruno. A pilot trial of the Treatment of Hyperglycemia in Ischemic Stroke (THIS) was also published very recently (Bruno et al. Stroke 2008). The study was conducted at 5 centers, and patients were randomized 2:1 to either an aggressive protocol of continuous IV insulin (n=31) or subcutaneous insulin as needed (usual care; n=15). “With meals, the glucose shoots up, and in our experience that's very hard to control, especially in stroke patients who may or may not eat their meal entirely,” commented Dr. Bruno. Four patients in the trial were not diabetic, and their profiles were more similar to the IV group even though they were assigned to usual care. “My impression from this is that it's very hard to improve on the glycemic control in the patients without diabetes,” concluded Dr. Bruno.
The role of glucose control in the prevention of stroke and cardiovascular disease was reviewed by Walter Kernan, MD, Yale University, New Haven, CT. In the Epidemiology of Diabetes Interventions and Complications (EDIC) study, 1375 patients with type 1 diabetes were followed from 1993–2005. These patients had participated in the earlier Diabetes Control and Complications Trial (DCCT, 1983–1993), in which they underwent either intensive management of their hemoglobin A1c (HbA1c) levels or conventional therapy. Those who had intensive therapy had a risk reduction of 57% in cumulative incidence of myocardial infarction (MI), stroke, or death after follow-up (p=0.02; Nathan et al. NEJM 2005). “By 17 years out, there's really quite a distinct difference between these two curves…experts have coined the term “metabolic memory” to account for this durable effect of glucose control,” noted Dr. Kernan.
The Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial was undertaken to further study the effect of tight glucose control on cardiovascular disease. A total of 10,251 patients with type 2 diabetes were randomized to either a target HbA1c<6% or HbA1c between 7.0% and 7.9%. Patients were followed for 2–7 years, and the primary endpoint was the incidence of non-fatal stroke, non-fatal MI, and cardiovascular death. The study was stopped prematurely in January 2008. According to press releases, the mortality was higher (1.4%) in the intensive treatment arm than in the conventional arm (1.1%). “This was very discouraging data for those who believed that tight control in patients with type 2 diabetes might prevent macrovascular disease,” summarized Dr. Kernan. A similar ongoing trial that is being conducted in Australia (ADVANCE) indicated in a press release issued on February 13, 2008, that an interim analysis revealed no evidence of increased mortality risk in patients undergoing intensive glucose-lowering therapy. The publications from these 2 trials will shed additional light on what is occurring in this population. Ongoing research is examining the effectiveness of interventions to improve insulin resistance for prevention of vascular disease among persons with pre-diabetes and diabetes. For now, multifactorial strategies should focus on managing traditional risk factors such as lifestyle, blood pressure, dyslipidemia, and hyperglycemia (to conventional American Diabetes Association goals) to minimize the risk of cardiovascular disease and stroke in patients with diabetes.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.