

Summary
The The Outcome of PCI for stent-ThrombosIs MultIcentre Study [OPTIMIST] trial was designed to assess the angiographic and clinical outcomes of percutaneous coronary intervention in patients with stent thrombosis.
- thrombotic disorders
- interventional techniques & devices clinical trials
The OPTIMIST (The Outcome of Pci for stent-ThrombosIs MultIcentre STudy) trial was designed to assess the angiographic and clinical outcomes of percutaneous coronary intervention (PCI) in patients with stent thrombosis.
Professor Francesco Burzotta, Catholic University of the Sacred Heart, Rome, Italy, who presented the findings of the study, noted that the OPTIMIST trial was also designed to evaluate the efficacy and feasibility of using thrombectomy devices during PCI for stent-related thrombosis and to compare the outcome associated with drug-eluting stent (DES) and bare metal stent (BMS) thrombosis.
This multicenter, independent retrospective study included data for 110 patients, representing the largest single series of patients with angiographically confirmed stent-related thrombosis, said Prof. Burzotta. He noted that stent-related thrombosis accounted for 3.6% of the emergency PCIs for STEMI. Stent thrombosis occurred in 62 patients with DES and 52 with BMS.
Prof. Burzotta reported that the overall clinical outcome at 6 months was poor, especially with regard to mortality and the rate of major adverse coronary or cerebrovascular events (MACCE) at 6 months (Table 1), despite the best pharmacological and technical resources. Angiographic outcome was also unsatisfactory, he said, with establishment of TIMI 3 blood flow in only 73% of patients.
PCI for Stent Thrombosis: Clinical Outcome.
Reperfusion was not significantly better after thrombectomy among the overall population. However, among patients without cardiogenic shock, restoration of both epicardial and myocardial reperfusion (TIMI epicardial flow grade 3 and MPG 2/3) was significantly improved after thrombectomy (89% vs 61%; p=0.027). “Mechanical thrombectomy is feasible but probably should be reserved for patients without hemodyanamic instability,” said Prof. Burzotta.
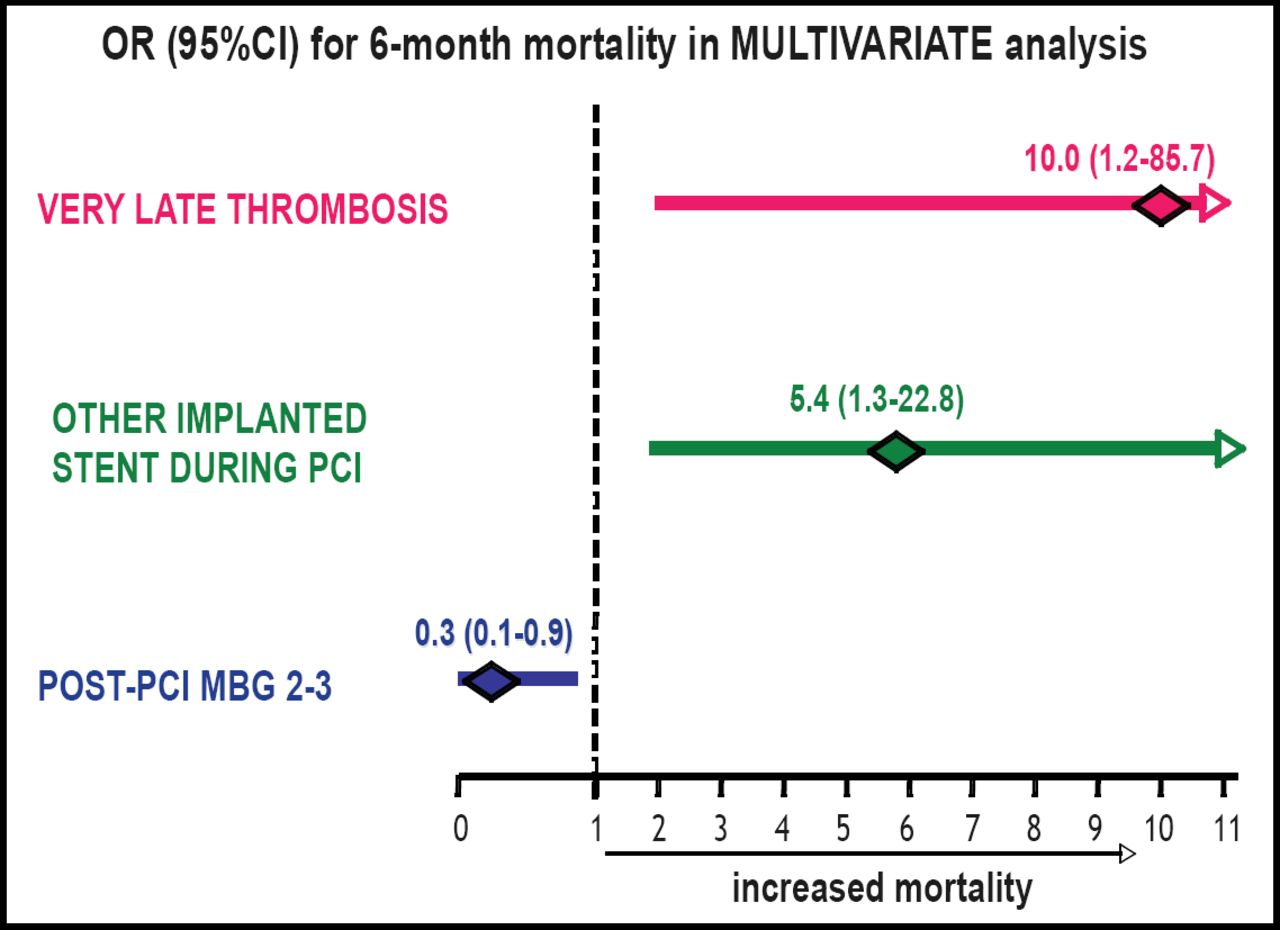
Multivariate analysis showed that very late thrombosis (at one year or more) and implantation of another stent at the time of treatment of the stent thrombosis were predictors of 6-month mortality, whereas achievement of good reperfusion was protective (Figure 1). Prof. Burzotta commented, “This means that two factors in the cath lab—a technical decision to implant another stent and the results obtained [for reperfusion]—influence late mortality.” He suggested that it might be more important to re-establish optimal myocardial flow than to fix stenosis.
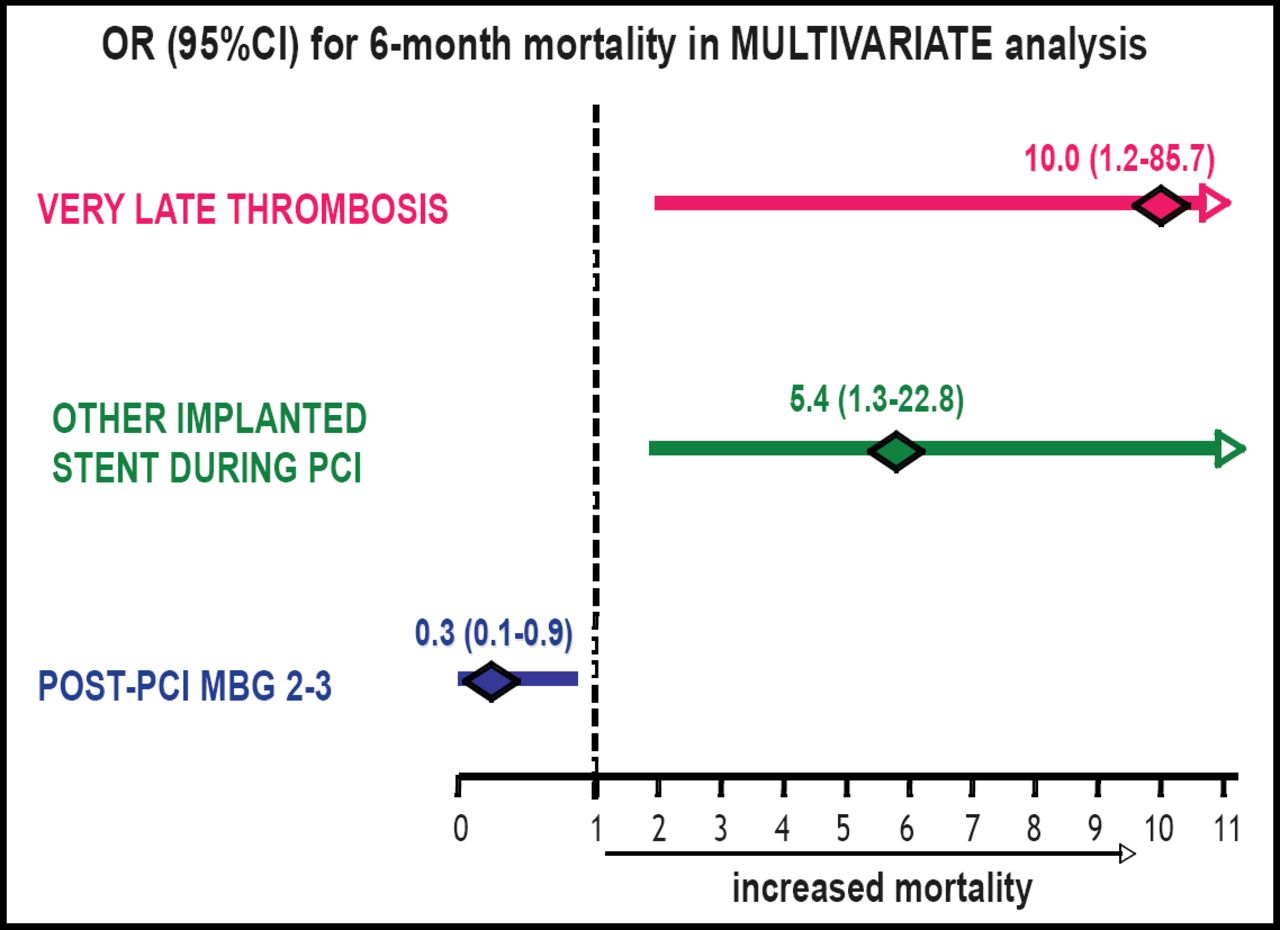
Predictors of Outcome in PCI for Stent Thrombosis.
The clinical and angiographic outcomes were similar for DES and BMS, but two clinical features differed. Prof. Burzotta explained that a significantly higher percentage of the thromboses that occurred after 30 days were related to DES (33% vs 14%; p=0.03). Also, there was a stronger association between DES-related thrombosis and the withdrawal of antiplatelet therapy within 15 days (15% vs 2%; p=0.04).
Professor William Wijns, Cardiovascular Center, Aalst, Belgium, who discussed the study, noted that the mechanisms of poor clinical outcome remain undetermined and could result from any or a combination of the following: persistent focal trigger of thombosis, systemic prothrombotic state, or poor left ventricular function due to the index infarction.
- © 2007 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.