

Summary
A panel of 4 experts explored clinical guidelines regarding pacing, implantable cardioverter-defibrillators, and cardiac resynchronization therapy. Two speakers also debated clinical, financial, and ethical questions related to continued use of cardiac resynchronization therapy in the setting of clinical improvement, such as an improved left ventricular ejection fraction.
- atrioventricular block
- cardiac resynchronization therapy
- generator replacement
- implantable cardioverter defibrillators
- left ventricular ejection fraction
- pacemaker
The basic goal of cardiac resynchronization therapy (CRT) is to restore left ventricular (LV) synchrony in patients with congestive heart failure and a widened QRS complex. A panel of 4 experts explored published clinical guidelines regarding pacing, the use of implantable cardioverter-defibrillators (ICDs), CRT, and the clinical manifestations of specific bradyarrhythmias.
Jean-Jacques Blanc, MD, Université de Bretagne Occidentale, Brest, France, began with a discussion of whether biventricular or right ventricular (RV) pacing is the more appropriate treatment for patients with high-degree atrioventricular (AV) block. He reviewed data suggesting that in many patients, RV apical (RVA) pacing induces LV dysfunction with severe clinical implications [Manolis AS. Pacing Clin Electrophysiol. 2006]. While options have been proposed to mitigate the detrimental effects of RVA pacing, they are usually not applicable to patients with permanent AV block. Data suggest that biventricular pacing may be a plausible approach for some patients [Curtis AB et al. N Engl J Med. 2013] but not for all [Blanc JJ. ESC. 2014].
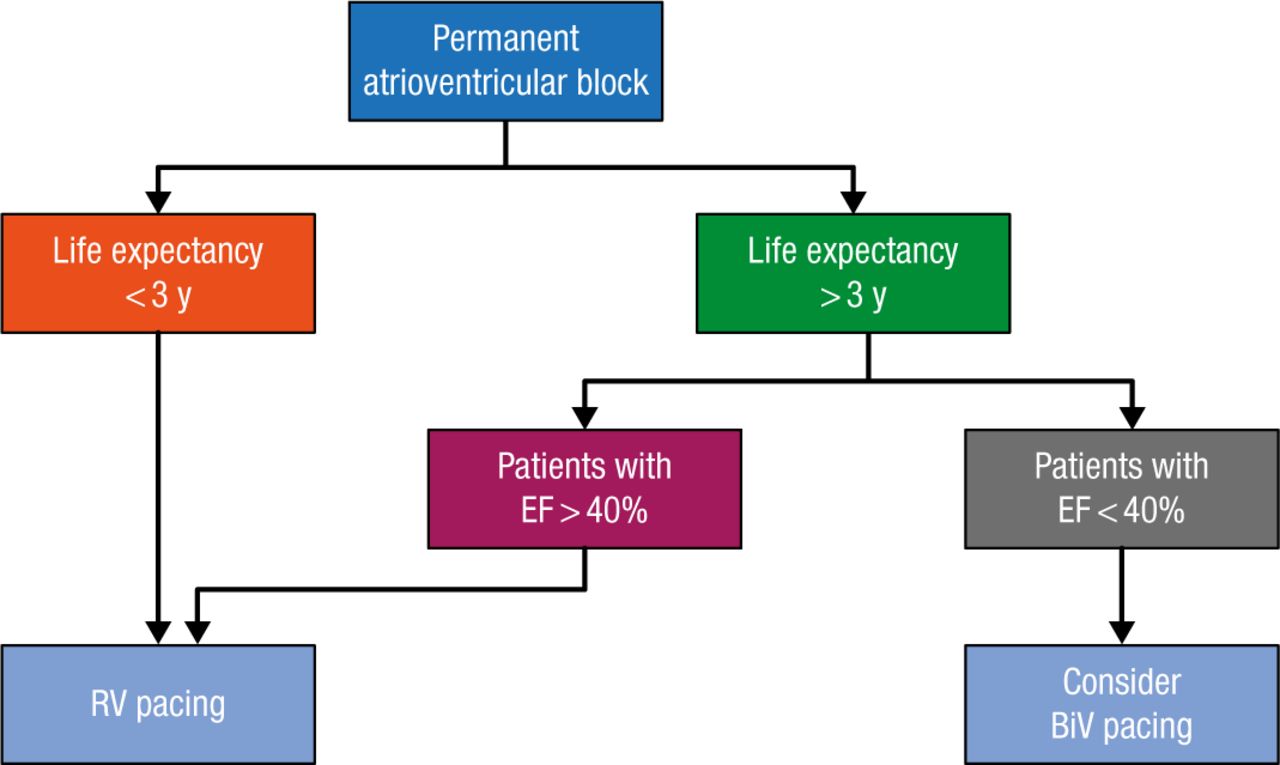
According to Prof Blanc, current research does not support a comprehensive recommendation of one pacing strategy over the other. Instead, he urged practitioners to consider the algorithm shown in Figure 1.
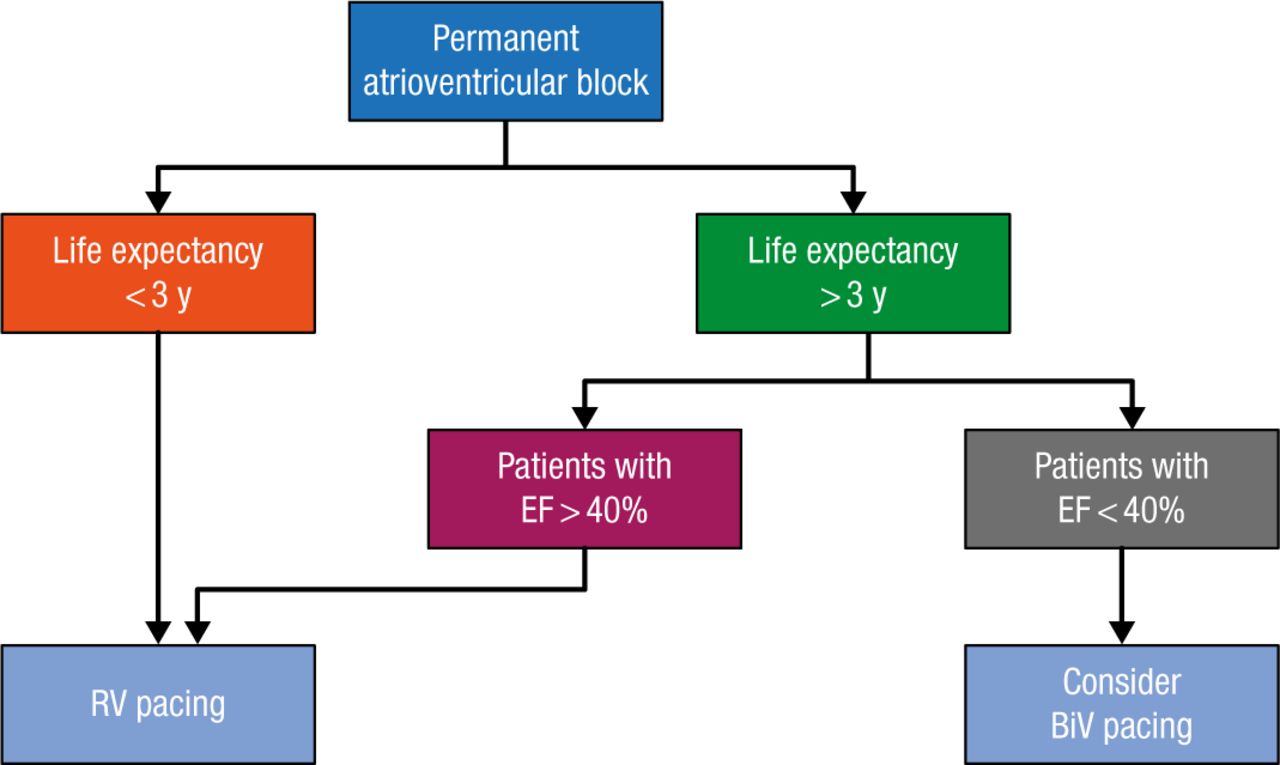
Algorithm to Choose RV vs BiV Pacing
BiV, biventricular; EF, ejection fraction; RV, right ventricular.
Reproduced with permission from JJ Blanc, MD.
He also recommended that patients with RVA pacing and an ejection fraction (EF) > 40% be evaluated regularly relative to LV function and heart failure status. If the parameters begin to deteriorate considerably, the clinician should propose an upgrade from RVA pacing to LV-based pacing, which has shown some success in several observational and randomized crossover studies [Tops LF et al. J Am Coll Cardiol. 2009].
He summarized his presentation with 2 key points:
In a select number of patients, LV-based pacing could be proposed as a first-line option to prevent the deleterious effects of RV pacing.
In patients with AV block and RV pacing, the clinician should monitor pacing parameters and LV function and consider upgrading to a biventricular system if the patient’s condition deteriorates.
Michael Glikson, MD, Sheba Medical Center, Tel Hashomer, Israel, presented 2 case studies to determine whether each patient would be better served by CRT or RV pacing. Case 1 was a man, and case 2 was a woman. Both were aged 70 years with symptomatic sinus bradycardia at 45 beats per minute. The man had a PR interval of 220 milliseconds, a right bundle branch block (RBBB) of 130 milliseconds, a normal EF, and NYHA class 1, whereas the woman had a PR interval of 320 milliseconds, an RBBB of 180 milliseconds, an EF of 36%, and NYHA class 2.
He then presented 4 possible options for pacing: (1) atrial pacing (AAI/R), (2) dual-chamber RV pacing (DDD/R), (3) DDD/R plus RV pacing minimization (MVP) algorithms, or (4) CRT pacing. According to Prof Glikson, AAI/R is not a good choice when compared with moderate AV delay management. AAI/R is associated with 2% to 3% AV block per year in certain populations and has no outcome benefit. AAI/R is also associated with twice the reoperative rate and does not appear to have an advantage outcome over DDD/R with moderately prolonged AV delay (AVD) [Nielsen JC et al. Europace. 2012; Nielsen JC et al. Eur Heart J. 2011]. He also confirmed the previous speaker’s comments regarding the deleterious effects of RV apical pacing.
Compared with DDD/R, DDD/R plus MVP appears to prevent ventricular desynchronization and moderately reduces the risk of persistent AF in patients with sinus node disease [Sweeney MO et al. N Engl J Med. 2007]. According to Prof Glikson, a patient with a very long PR interval and conduction system disease is not likely to see a clear advantage of DDD/R plus MVP compared with simple DDD/R pacing. A patient with conduction system disease is more prone to progress to complete AV block—at which point no MVP algorithm will be useful.
Compared with traditional pacing, there is little evidence that CRT provides a benefit for patients with preserved systolic function [Brignole M et al. Eur Heart J. 2013]. Furthermore, there is limited support for any effect of CRT in RBBB, and the effect of CRT may be limited to patients with QRS > 150 milliseconds and advanced congestive heart failure.
Prof Glikson closed his remarks by returning to his original 2 cases. On the basis of the evidence that he provided during his presentation, he concluded that the best treatment for case 1 would be DDD/R plus MVP and for case 2, CRT.
Maurizio Gasparini, MD, Humanitas Research Hospital, Rozzano-Milano, Italy, next spoke about how to determine whether an ICD should be replaced at the time of battery depletion. According to Prof Gasparini, if a conventional ICD was originally implanted for the correct indication, it would be unusual to deny the patient a replacement at the time that the battery needed to be changed, usually at 5 to 7 years. Some patients are too ill to undergo ICD replacement, while others might be deemed too well for ICD replacement. In some cases, the initial indication no longer meets guideline indications [Kini V et al. J Am Coll Cardiol. 2014]. In other cases, the EF may have been underestimated at the time of the initial implant [Kutyifa V et al. J Am Coll Cardiol. 2013]. Prof Gasparini argued that in most cases, denying ICD replacement might also raise ethical and legal implications. Even in this case, however, the clinician should hold a thorough discussion with individual patients and their families.
Jagmeet Singh, MD, Harvard Medical School, Boston, Massachusetts, USA, rounded out the session with a presentation focusing on whether patients who have an implanted CRT defibrillator should receive a pacemaker or a defibrillator at the time of generator replacement if they have an improved left ventricular ejection fraction (LVEF). Although current guidelines for ICDs are based on an LVEF < 35%, Dr Singh emphasized that a onetime baseline risk is not an everlasting risk, that survival can be normal once the LVEF has normalized, that ICDs can pose harm, and that it is the responsibility of a clinician to revisit the indications for ICD implant. Recovery of LVEF post-CRT is associated with significantly reduced appropriate ICD therapy.
According to Dr Singh, patients with improvement of LVEF ≥ 45% and those with primary prevention indication for ICD appear to be at lowest risk [Chatterjee NA et al. Eur Heart J. 2015]. In addition, inappropriate ICD shocks are fairly common and significantly associated with worse outcomes. He also urged providers to use a more deliberative process at the time of generator change. Clinical situations change over a 6- to 8-year period prior to the need for generator change. However, defining response is still an issue, and it is important to define what the cutoff in LVEF should be. Dr Singh proposed that the decision not to replace an ICD be based on a patient’s risk of sudden cardiac death as determined by 3 metrics:
LVEF > 45%
Initial indication for primary prevention
No documented arrhythmias and no ICD therapy over the length of the device
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.