

Summary
This article discusses the increasing global burden of cardiovascular disease and highlights key risk factors in Asia in particular. It also discusses some important interventions that have been initiated in order to reach the World Heart Federation’s goal of a 25% reduction in premature deaths from cardiovascular disease by 2025.
- Asia
- cardiovascular disease
- coronary artery disease
- diabetes
- Emerging Leaders Programme
- hypertension
- obesity
- smoking
- stroke
- World Heart Federation
- World Health Organization
- WHO
- cardiology & cardiovascular medicine guidelines
- cardiology & cardiovascular medicine screening & prevention
- hypertensive disease
- smoking cessation
The World Health Organization (WHO) has endorsed a target to reduce deaths from noncommunicable diseases (NCDs) by 25% by the year 2025 (25 by 25), and in conjunction with this, the World Heart Federation (WHF) aims to achieve a 25% reduction in premature deaths from cardiovascular disease (CVD) by this date. A panel of speakers discussed the significant burden of CVD worldwide and highlighted important goals and interventions that aim to achieve this target.
Cardiovascular Disease in Asia
According to Cheuk-Man Yu, MD, The Chinese University of Hong Kong, Hong Kong, China, CVD-associated morbidity and mortality are a substantial problem in Asia, and their rates continue to rise, along with the cost of managing CVD. In particular, CVD burden and mortality are especially high in Central and South Asia compared with developed countries, he said [Moran AE et al. Circulation. 2014].
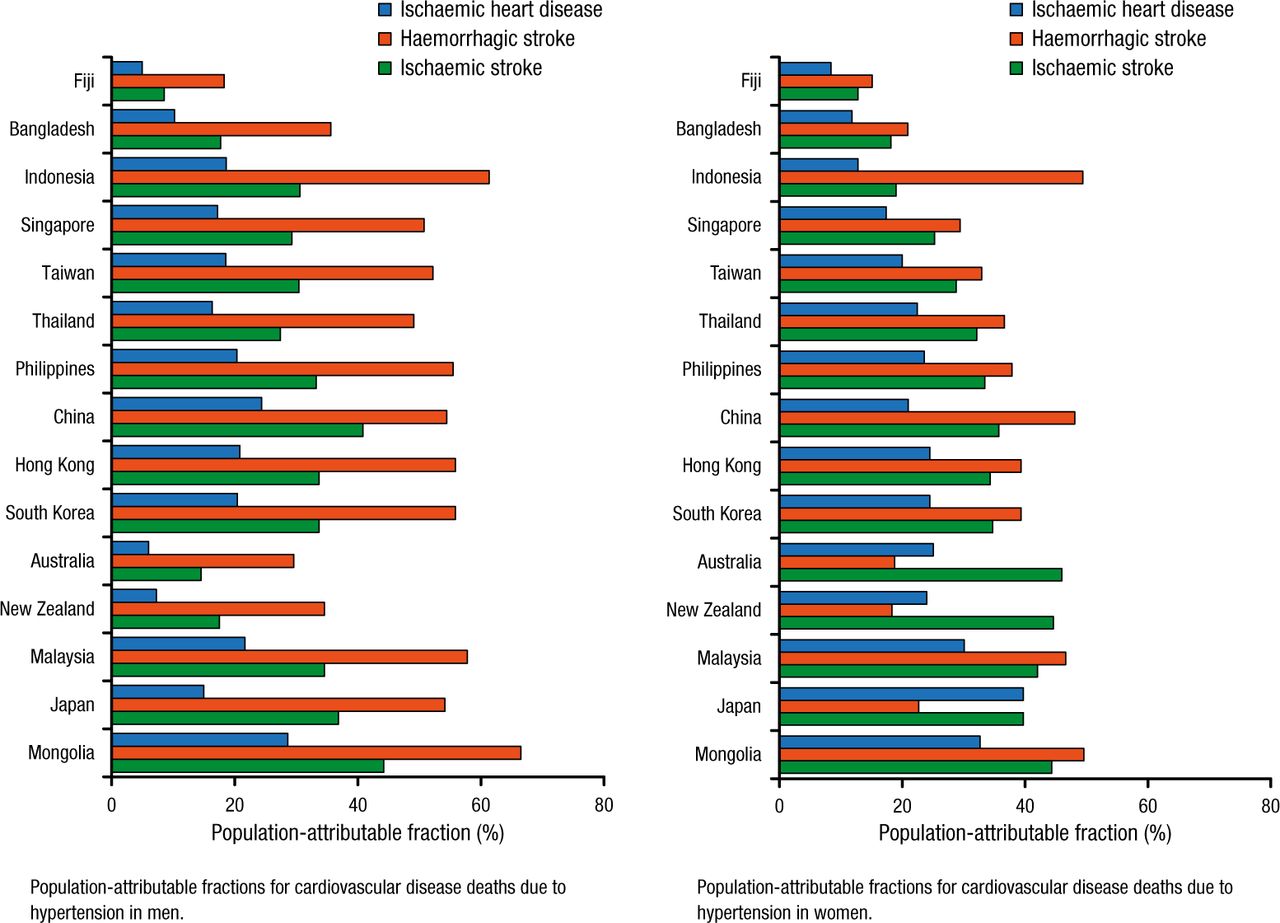
The relationship between risk factors and CVD is slightly different in Asia than in Western countries, Prof Yu added. Indeed, hypertension (HTN) is increasing in prevalence in Asia, and plays a more significant role in the development of CVD and its associated deaths in this region (Figure 1) [Martiniuk AL et al. J Hypertens. 2007]. Coronary artery disease and stroke (typically ischemic stroke involving large arteries) are 2 other major risk factors [Mehndiratta MM et al. J Neurol Neurosurg Psychiatry. 2014; Moran AE et al. Circulation. 2014]. In addition, the marked increase in the prevalence of obesity and diabetes mostly reflects changes in lifestyle as a result of economic development [Ramachandran A et al. Lancet. 2010; Yoon KH et al. Lancet. 2006]. Smoking is also a common health care problem and CVD risk factor in Asia [Martiniuk ALC et al. Tob Control. 2006]. CVD risk factor–free adults comprise the minority of the Asian population, he added.

Cardiovascular Disease Deaths Associated With Hypertension in Men and Women in Asia
Reprinted from Martiniuk AL et al. Hypertension: its prevalence and population-attributable fraction for mortality from cardiovascular disease in the Asia-Pacific region, J Hypertens., Vol 25, issue 1, Pages 73-79, Copyright © (2007), with permission from Lippincott Williams.
The prevalence of these risk factors is also projected to double by 2030, said Prof Yu, adding that the cost burden of treatment for CVD in Asia will also increase accordingly, for both drugs and devices. Consequently, because management of patients with CVD in Asia is largely based on European and American data [Kwong JS, Yu CM. Nat Rev Cardiol. 2013], more clinical trials are needed in Asia to help determine the efficacy of specific treatments and define treatment guidelines targeted to Asian patients, he concluded.
Cardiovascular Disease in Europe
Dan Gaita, MD, PhD, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania, highlighted the substantial burden of CVD in Europe, where recent data have shown that CVD accounts for about 40% of all deaths in men and even more (49%) in women [Townsend N et al. Eur Heart J. 2015].
According to Prof Gaita, although risk factors such as inactivity, HTN, and elevated cholesterol levels are common, obesity and diabetes are the most significant in Europe. He discussed the different aims and prevention activities underway in various European countries in order to help reach the 25 by 25 goal. For example, Ireland has a high prevalence of overweight or obesity (61% to 64%) and smoking (22%). Its future aims, however, are to increase the proportion of people who are healthy at all stages of life, and to have a smoking rate of < 5% by 2025. To meet these goals, it has initiated a National Cardiovascular Health Policy (2010-2019), a Childhood Obesity Campaign, and the Tobacco Free Ireland campaign.
He also shared some data from Romania, noting that it ranks fourth among European countries with respect to obesity prevalence, and ninth for smoking. Nevertheless, its future aim, in conjunction with the Romanian Heart Foundation, is to reduce CVD mortality by 10% by 2025, to extend cardiovascular health, and to increase quality of life.
Prof Gaita emphasized the value of WHF roadmaps in guiding European countries toward their 2025 targets. This is particularly important because, although the estimated efficacy of CVD treatments is about 75%, this is further reduced by several factors, including patient adherence and lifestyle, he concluded [Perel P et al. Global Heart. 2015].
The Role of the WHF in Reducing Premature Deaths From CVD
According to Johanna Ralston, World Heart Federation, Geneva, Switzerland, the Global Burden of Disease 2010 Study data showed that although CVD accounts for about one-third of deaths due to NCDs, < 1% of official development assistance funding is assigned to manage CVD. One major reason for this gap is advocacy. She noted that in the global health space, NCDs, including CVD, were omitted from the Millennium Development Goals that were initiated in 2000 to focus donor priorities and funding around key global issues.
Consequently, she added that among other things, the WHF aims to significantly reduce this gap between CVD burden and resources. It is instrumental both as an advocate in the campaign for global action on CVD and in guiding implementation of effective interventions.
Ralston said that the WHF has identified 5 key focus areas as part of its strategy to achieve the WHO’s global target of a 25% reduction in premature mortality due to CVD by 2025:
Increased global advocacy
Development of national plans in priority countries
Development of the Emerging Leaders Programme, CVD roadmaps, and a CVD prevention course in primary care
Increased focus on rheumatic heart disease
Expansion of the World Congress of Cardiology to become the World Congress of Cardiology and Cardiovascular Health; and the World Heart Day initiative
Highlighting the Emerging Leaders Programme, Ralston noted that it aligns with the WHO’s 25 by 25 goal. This initiative comprises a long-term collaboration of CVD experts that aims to achieve the biggest possible improvement in global heart health. The expert group changes each year, and each group focuses on a key priority area. The 2016 program will focus on tobacco prevention and control, said Ralston.
She also emphasized that in order to reach the 2025 goal, the WHF’s highest priority targets include HTN (aiming for a 25% relative reduction in the prevalence of HTN), secondary CVD prevention (to enable 50% of eligible people to receive drug therapy or counseling), and tobacco control (to achieve a 30% reduction in tobacco use). Success in reaching these 3 targets will save many lives and achieve the WHO’s 25 by 25 target, concluded Ralston.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.