

Summary
Reductions in cardiovascular mortality have been achieved via improved prevention, diagnosis, and treatment. However, costs have risen accordingly. A future emphasis on health promotion and disease prevention through research, education, and mitigation of disease-causing environmental factors holds the promise of improving outcomes and reducing the cost of treating CV disease.
- arrhythmias
- cardiovascular disease
- coronary artery disease
- education
- environment
- future
- imaging
- prevention
- therapeutics
- valvular disease
Leading experts in cardiology shared their visions for the future of cardiovascular (CV) disease management. Sophisticated imaging techniques, interventional technologies, and medical therapies are transforming the identification and treatment of arrhythmias, valvular diseases, and coronary artery disease (CAD). At the same time, a shift from a focus on treating disease to health promotion and disease prevention promises to reduce avoidable deaths from heart disease.
Sophisticated Imaging and Robotic Technology to Transform Arrhythmia Therapy
According to Josep Brugada, MD, PhD, University of Barcelona, Barcelona, Spain, the medical field is moving from reactive, disease-based medicine to P4 medicine (personalized, predictive, preventive, participatory). In the next 10 to 15 years, the focus will be on highly sophisticated imaging technology, minimally invasive therapeutics, and personalized genomic medicine.
Although progress has been made in the detection and treatment of arrhythmias, therapy is not standardized to produce the same results across centers and regions. In the next years, it may be possible to automatically identify reentrant circuits with magnetic resonance imaging (MRI) and systematically ablate them using robotic technology.
Currently, a variety of imaging systems and ablation methods are used for atrial fibrillation ablation, but only up to 70% of arrhythmias are successfully ablated. Prof Brugada predicted that a systematic approach using MRI anatomic map-guided ablation to identify and automatically ablate electrical channels will be used in the next decade.
There are 300 000 sudden cardiac deaths (SCDs) among the general population each year, according to Prof Brugada. Several risk factors are known but many persons at risk are not identified. MRI could be used to identify abnormalities such as arrhythmogenic scars.
New technologies that may reduce the incidence of SCD include wide distribution of public access defibrillators and sophisticated pacemakers. Small leadless, heart movement–powered pacemakers with wireless communication that can be implanted in the heart are also in development. Biological pacemakers using gene technology to convert normal heart cells into pacemaker cells and stem cells to repair injured areas of the heart are on the horizon. Novel therapeutic approaches using gene transfer, gene silencing, and gene editing techniques to cure genetic arrhythmogenic diseases are also under development.
Improved Imaging and New Therapies for Future Management of Coronary Artery Disease
Looking into the future of CAD treatment, Christian JM Vrints, MD, Antwerp University Hospital, Antwerp, Belgium, envisions the advent of improved imaging, revascularization, and lipid-lowering technologies.
Improved imaging of coronary arteries using coronary computed tomography angiography (CTA) can be expected in the future. CTA can detect, characterize, and quantify vulnerable plaques before they cause cardiac events [Maurovich-Hovat et al. Nat Rev Cardiol. 2014]. CT-derived fractional flow reserve (FFRCT) provides high diagnostic accuracy of hemodynamically significant CAD compared with invasive FFR and greater specificity compared with CTA [Norgaard BL et al. J Am Coll Cardiol. 2014]. Dynamic CT myocardial perfusion imaging is being studied for identification of ischemic myocardium.
The focus in CAD is shifting from identifying vulnerable atherosclerotic plaques to evaluating the total plaque burden for coronary event risk estimation. The use of bioabsorbable stents shows promise for promoting long-term vascular healing [Karanasos A et al. J Am Coll Cardiol. 2014].
New lipid-lowering agents with the potential to prevent CV events are emerging. The monoclonal antibody evolocumab has reduced low-density lipoprotein (LDL) levels and CV events when combined with standard therapy vs standard therapy alone [Sabatine MS et al. N Engl J Med. 2015].
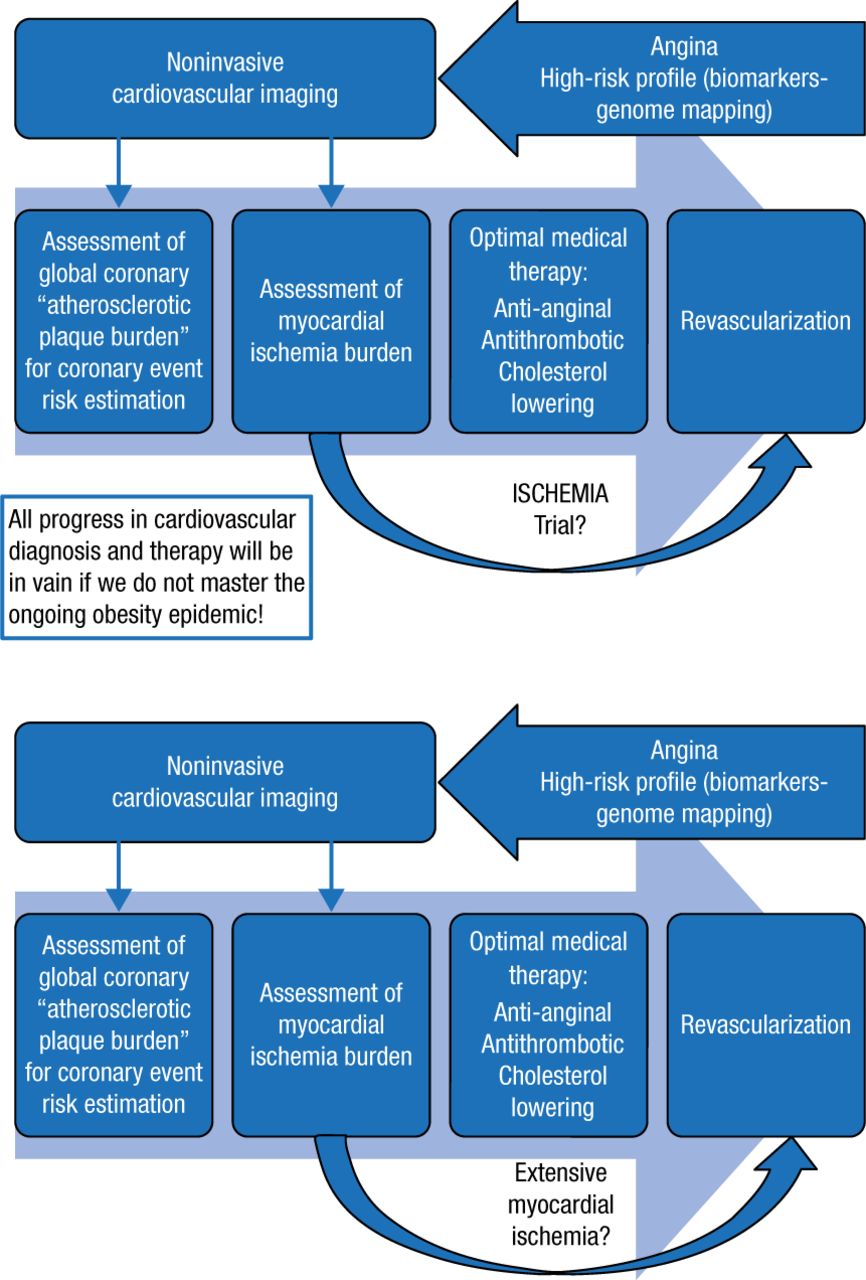
Prof Vrints presented an algorithm for the future management of CAD but cautioned that ischemic heart disease deaths may increase again if the ongoing obesity epidemic is not curbed (Figure 1). Optimal medical therapy aiming at preventing ischemia, thrombosis, and plaque burden progression will be the cornerstone of the management of CAD. Whether early revascularization in case of severe ischemia is helpful in chronic stable CAD will be clarified by the ongoing ISCHEMIA trial.
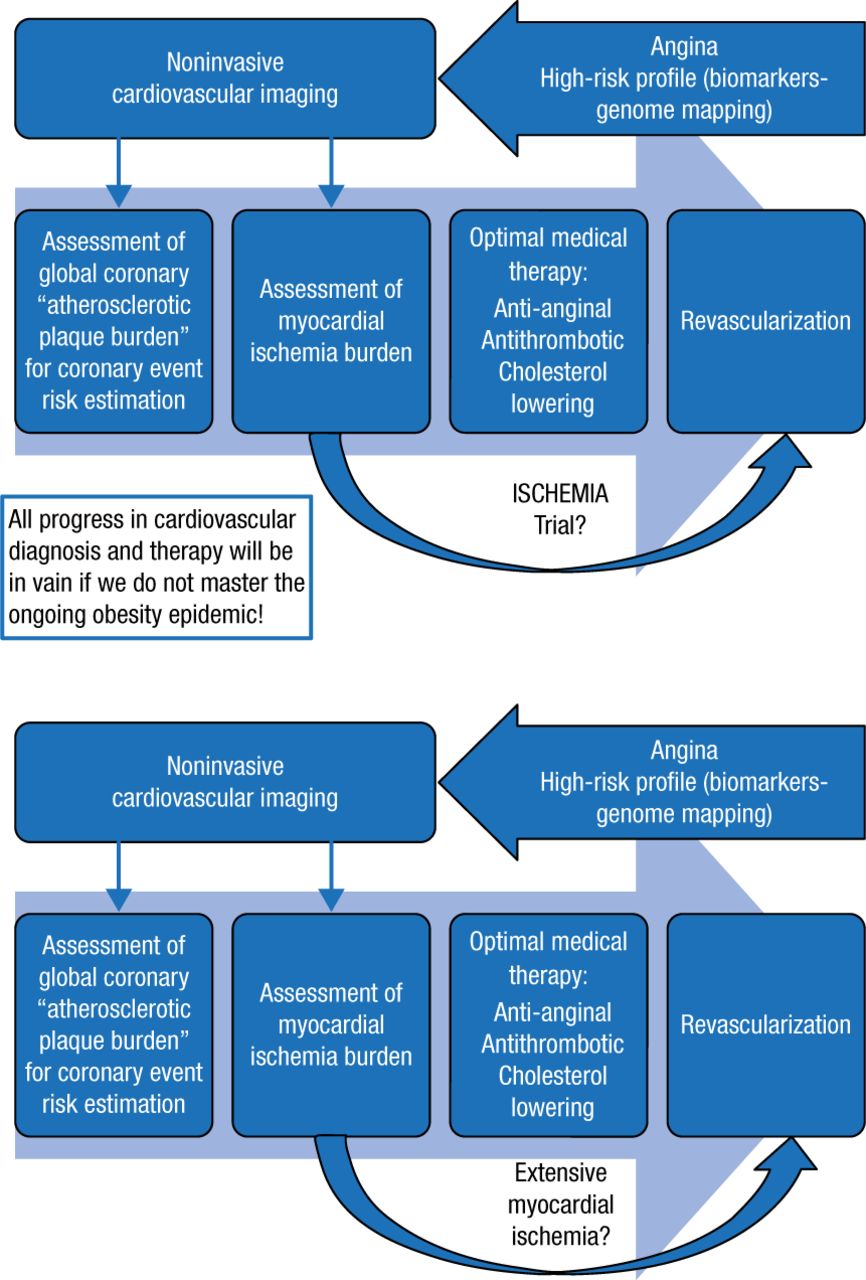
Future Management of Coronary Artery Disease
Reproduced with permission from CJM Vrints, MD.
Growth of Transcatheter Interventions for Valvular Heart Disease
Alain Cribier, MD, University of Rouen, France, presented his views about the future treatment of valvular heart disease (VHD). The role of interventional procedures for aortic stenosis (AS) and mitral regurgitation (MR) has been increasing since the early 1980s and is expected to grow by 30% over the next decade.
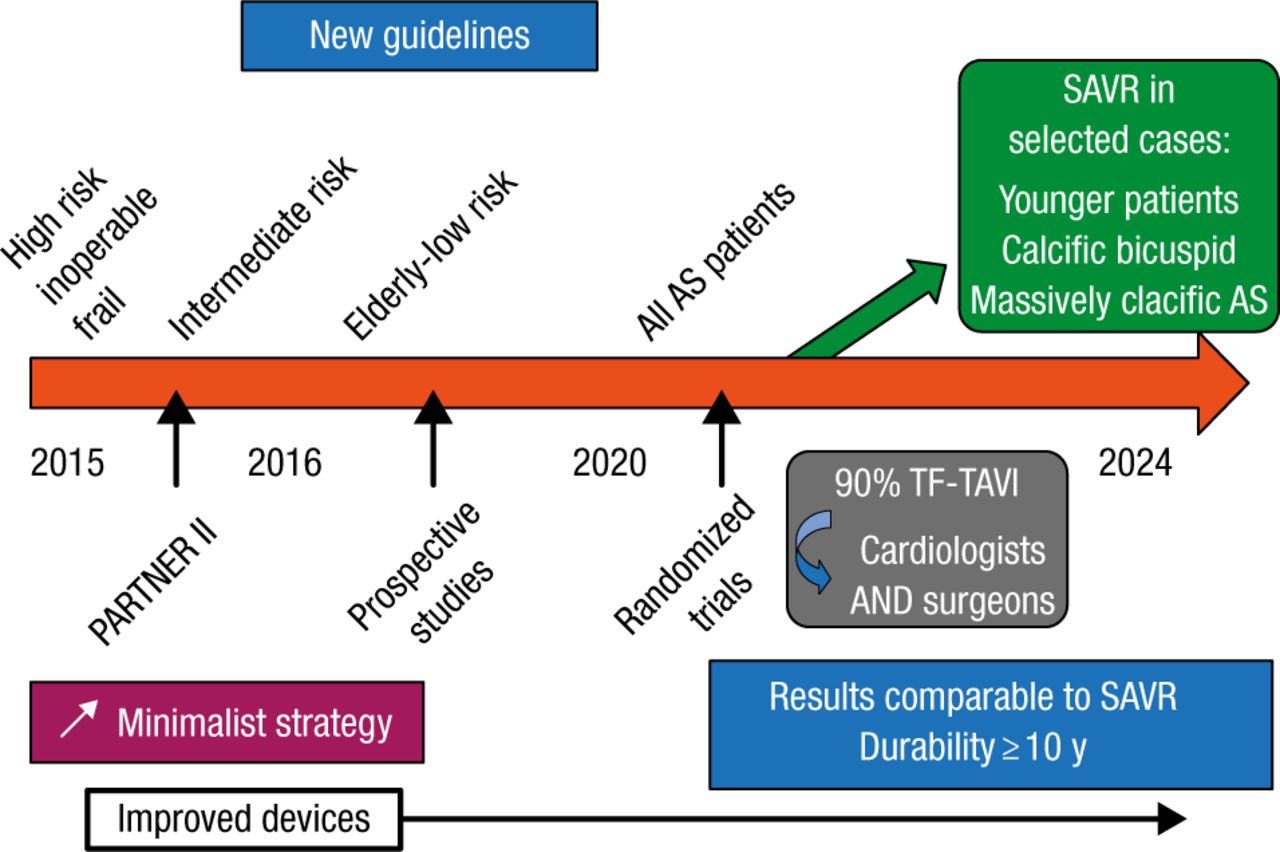
The advent of transcatheter atrial valve replacement (TAVR) for AS in 2002 has changed the landscape of interventional cardiology with more than 200 000 procedures performed worldwide, and a 4-fold increase in the number of patients treated predicted in the next decade. TAVR is now the standard of care for inoperable patients with AS and an important alternative to surgical AVR for high-risk patients [Kapadia SR et al. Lancet. 2015; Mack MJ et al. Lancet. 2015]. Advanced valves and delivery systems are improving TAVR results, and a minimalist approach that reduces time in the hospital is becoming more common. Prof Cribier predicted that TAVR indications will expand and results will improve in the next decade (Figure 2).
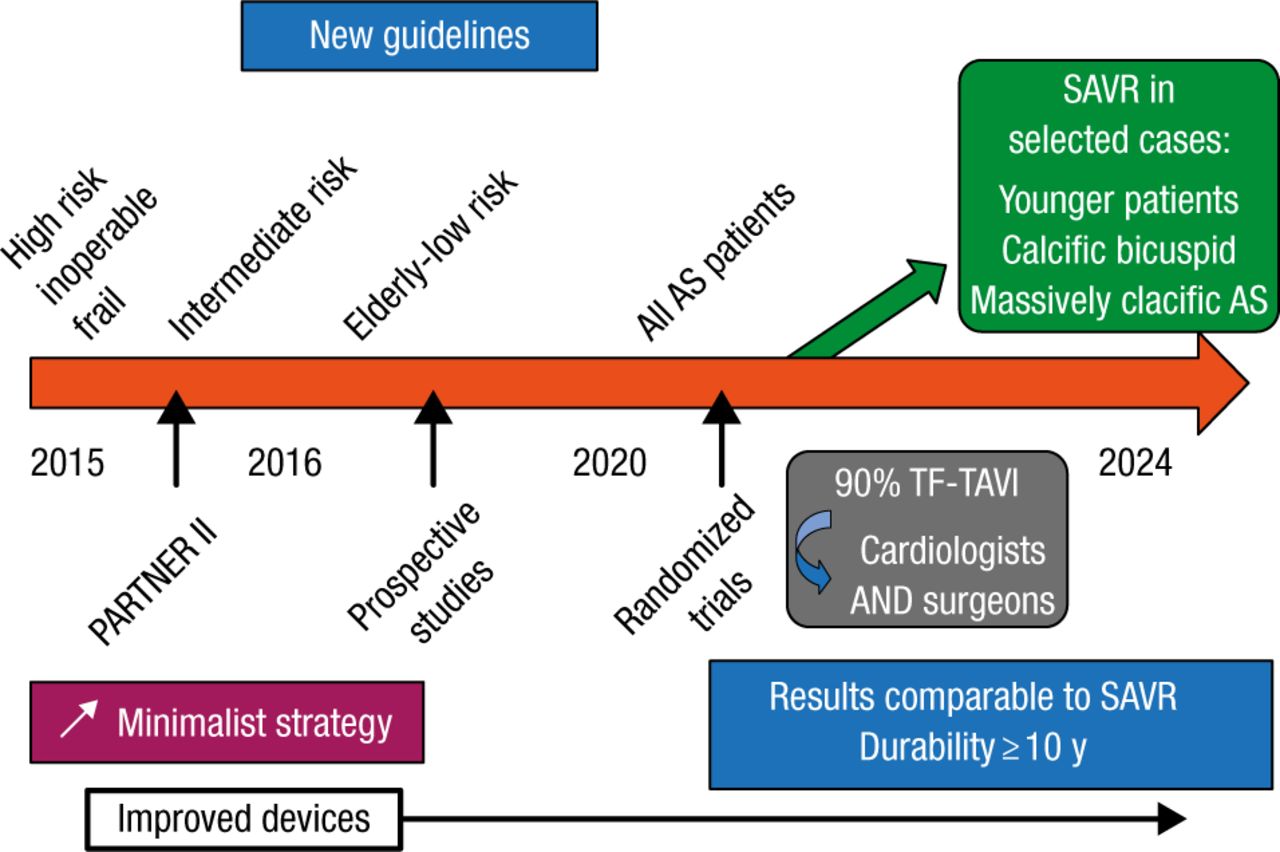
Vision for the Future of Transcatheter Aortic Valve Replacement
AS, aortic stenosis; SAVR, surgical aortic valve replacement; TF-TAVI, transfemoral transcatheter aortic valve implantation.
Reproduced with permission from A Cribier, MD.
Effective treatment for MR is an unmet clinical need, but innovative techniques for transcatheter mitral valve repair (TMVR) are dramatically increasing.
The greatest change in the management of VHD will be a considerable growth of transcatheter interventions. In patients with AS, advanced TAVR systems, improved operator technique, and a minimalist strategy will allow a fast expansion of indications to lower risk patients. For patients with degenerative and functional MR, interventional techniques, valve repair, and TMVR will continue to grow.
Shifting Focus to Prevention of Environmental Causes of Cardiovascular Disease
Valentin Fuster, MD, Mount Sinai Hospital, New York, New York, USA, discussed the relationship between the environment and CV disease. As people age, environmental conditions contribute to CV and other diseases and high health care costs. In the United States and Europe, CV mortality rates have decreased since the 1980s; 50% of this decrease can be attributed to prevention and 50% to health care technology. The cost of treatment for CV disease is expected to increase from $273 billion in 2010 to $818 billion in 2030 [Heidenreich PA et al. Circulation. 2011]. Prevention measures can go a long way toward decreasing these costs.
Among the top 25 diseases worldwide, of which one-third are related to the environment, ischemic heart disease is the most common [Kunzli N. Eur Heart J. 2015]. In addition to established risk factors, increasing evidence shows that air and noise pollution induce inflammation and oxidative stress in blood vessels, leading to obesity, diabetes, and CV disease [Munzel T et al. Eur Heart J. 2015].
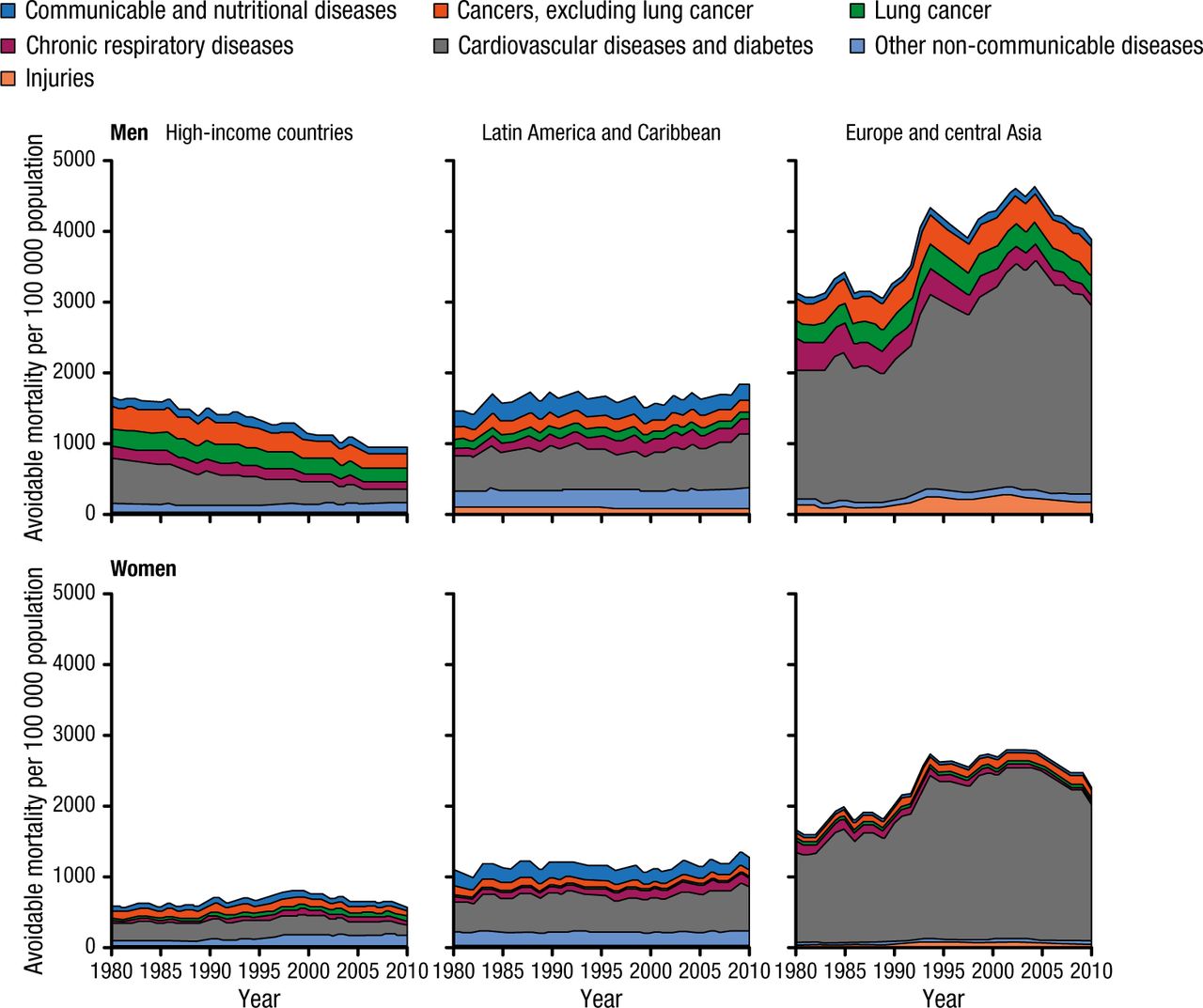
Programs throughout the world are using science and education to improve CV health. Programs such as these have the potential to reduce the number of CV deaths from avoidable causes (Figure 3).

Avoidable Mortality Rates (Aged > 60 Years) in 51 Selected Countries (1980–2011)
Reprinted from The Lancet, Vol 385, Mathers CD et al, Causes of international increases in older age life expectancy, Pages 540-548, Copyright (2015), with permission from World Health Organization.
One such program, developed by Dr Fuster and colleagues, employs a stratified approach to sustaining health throughout a lifetime. This approach promotes CV health and prevention of disease progression at 3 different age ranges using educational and behavioral tools appropriate to the age range and physiologic background. The optimal time to motivate healthy behavior is between the ages of 3 and 5 years. Educational interventions on how the body and heart work, healthy food habits, physical activity, and emotional habits to avoid addiction are used at this time. This program has had beneficial effects on adiposity, with the greatest impact when started at the earliest age and maintained over 3 years. At the age range of 25 to ~ 50 years, subclinical disease is evaluated with advanced noninvasive imaging modalities [Fernandez-Friera L et al. Circulation 2015; Baber U et al. J Am Coll Cardiol. 2015]. Findings of subclinical disease can be used as motivation for lifestyle changes. After age 50 years, the entire individual is examined for systemic CV disease, including the neurovascular region for microvascular changes that might cause dementia.
New technologies are leading to a better understanding of CV disease and its causes. Individualized treatment is becoming possible with emerging imaging techniques and genetic therapies. The recognition of lifestyle and environmental causes of CV disease has led to a focus on health promotion and disease prevention with goals for reducing CV mortality worldwide.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
- Article
- Summary
- Sophisticated Imaging and Robotic Technology to Transform Arrhythmia Therapy
- Improved Imaging and New Therapies for Future Management of Coronary Artery Disease
- Growth of Transcatheter Interventions for Valvular Heart Disease
- Shifting Focus to Prevention of Environmental Causes of Cardiovascular Disease
- Figures & Data
- Info & Metrics
- eLetters
Cited By...
- No citing articles found.