

Summary
The retrospective PROMETHEUS study demonstrated that patients with an acute coronary syndrome who underwent percutaneous coronary intervention were more likely to be treated by their physicians with prasugrel as opposed to clopidogrel if they were younger and had a lower risk factor burden. The adjusted rate of ischemic events and bleeding risk is similar with prasugrel and clopidogrel.
- prasugrel
- clopidogrel
- acute coronary syndrome
- PROMETHEUS
- ischemic events
- bleeding
- percutaneous coronary intervention
- cardiology & cardiovascular medicine clinical trials
A retrospective study has shown that patients with an acute coronary syndrome (ACS) treated with prasugrel after a percutaneous coronary intervention (PCI) with stenting were younger and had a lower incidence of ischemic and hemorrhagic events, compared with patients treated with clopidogrel. Prasugrel was associated with a lower rate of ischemic events, but after adjustment for baseline characteristics, the magnitude of benefit was smaller and no longer statistically significant compared with clopidogrel.
The PROMETHEUS study was conducted to characterize patients with ACS who underwent PCI with stent implantation at 8 academic medical centers in the United States between January 2010 and June 2013. Each center maintained an institutional database with baseline clinical, procedural, and outcome data, stated Usman Baber, MD, MS, Icahn School of Medicine at Mount Sinai, New York, New York, USA.
PROMETHEUS included 19 914 patients, of whom 4058 (20%) received prasugrel and 15 856 (80%) received clopidogrel at the time of their index PCI. The majority of patients (n = 11 216; 56%) had unstable angina, followed by NSTEMI (n = 5412; 27%) and STEMI (n = 3285; 17%). The patients treated with clopidogrel compared with prasugrel more commonly presented with unstable angina (57.3% vs 52.3%), while patients presenting with NSTEMI or STEMI were more frequently treated with prasugrel compared with clopidogrel (28.6% vs 26.8% and 19.1% vs 15.8%, respectively).
The patients treated with prasugrel were significantly younger than those treated with clopidogrel, and they had a significantly lower frequency of major risk factors (P < .0001; Table 1).
Baseline Characteristics
Multivessel disease was identified in 41.2% of prasugrel-treated patients and 42.4% of clopidogrel-treated patients. In the prasugrel-treated group vs the clopidogrel-treated group, the stents were longer (31.4 vs 30.5 mm), larger in diameter (3.01 vs 2.96 mm), and more commonly a second-generation drug-eluting stent (81.2% vs 66.4%; P < .05 for all). The clopidogrel-treated vs the prasugrel-treated patients were more likely to receive periprocedural bivalirudin (74.0% vs 67.6%) and less likely to receive a glycoprotein 2b/3A inhibitor (21.4% vs 29.0%; P < .05 for all).
The primary efficacy end point of PROMETHEUS was the rate of major adverse cardiac events (MACEs; composite of all-cause death, myocardial infarction, stroke, and unplanned revascularization) at 90 days after the index PCI. The primary safety end point was bleeding that required hospitalization.
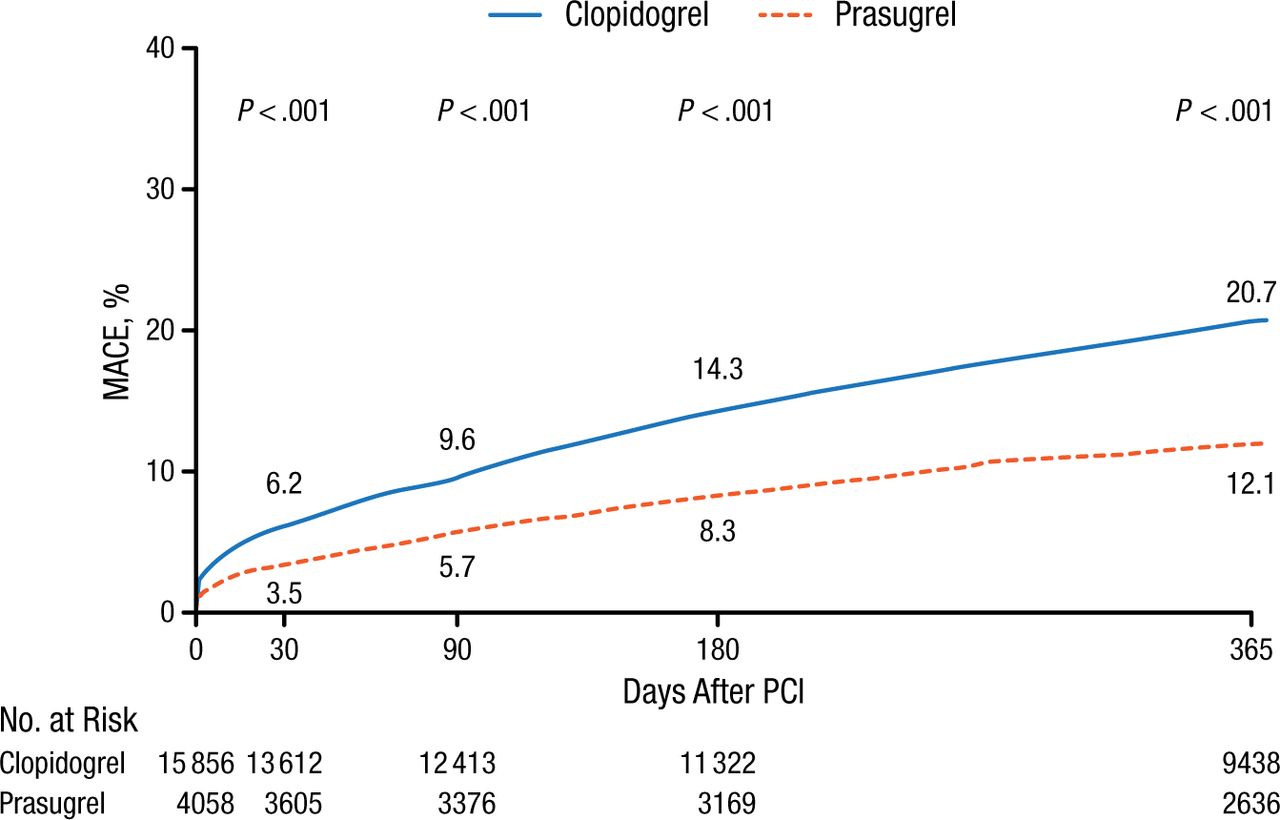
The unadjusted MACE rates showed a significant reduction with prasugrel vs clopidogrel (Figure 1), including for the primary efficacy end point at 90 days (P < .001).

Unadjusted MACE Rates Over 1 Year in PROMETHEUS
MACE, major adverse cardiac event; PCI, percutaneous coronary intervention.
Reproduced with permission from U Baber, MD.
Although the unadjusted hazard ratios (HRs) for MACE favored prasugrel at each assessment, the adjusted HRs were less significant. At 90 days, the unadjusted HR for MACE was 0.58 (P < .001), and the adjusted HR was 0.89 (P = .17). For myocardial infarction, the unadjusted HR was 0.51 (P < .001), but the adjusted HR was 0.84 (P = .18). For all-cause death at 90 days, the unadjusted HR was 0.21 (P < .001) and remained significant when adjusted (0.62; P = .04).
The unadjusted HRs for bleeding were significantly lower with prasugrel vs clopidogrel at each assessment, but the adjusted HRs showed no difference between the 2 treatments. At 90 days, the unadjusted HR was 0.65 (P < .001), and the adjusted HR was 1.03 (P = .79).
Dr Baber concluded that the lack of a difference in the bleeding rates with the 2 drugs after adjustment may reflect the selection of patients for PCI who are at very low risk for hemorrhagic complications. A possible interpretation of these data, he stated, is that the use of prasugrel should be based on the patient’s risk for an ischemic event to achieve more benefit with the drug, and its broader use in eligible patients may yield results similar to those in clinical trials.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.