

Summary
Atrial fibrillation (AF) is the most common arrhythmia encountered in clinical practice and is associated with significant morbidity, mortality, and health care expenditures. Prevention of AF is of major public health importance; however, up to 58% of the risk factors for AF are currently unknown. Therefore, the prevention of AF is critical. This article discusses the role of exercise in AF, the effect of supplements on AF, role of the treatment of sleep apnea in the prevention of AF, as well as cultures lifestyle and psychosocial interventions.
- Sleep Disorders
- Arrhythmias
- Prevention & Screening
- Sleep Disorders
- Cardiology & Cardiovascular Medicine
- Arrhythmias
- Prevention & Screening
- Exclusive Article - For home page
Atrial fibrillation (AF) is the most common arrhythmia encountered in clinical practice and is associated with significant morbidity, mortality, and health care expenditures. Prevention of AF is of major public health importance; however, up to 58% of the risk factors for AF are currently unknown. Therefore, the prevention of AF is critical. Christine M. Albert, MD, MPH, Brigham and Women's Hospital, Boston, Massachusetts, USA, discussed the role of exercise in AF.
Although moderate physical exercise is associated with broad health benefits, more vigorous exercise may predispose individuals to AF. A meta-analysis demonstrated that patients who regularly perform vigorous exercise, including marathon runners and cyclists, had an increased risk for AF, with odds ratios ranging from 2.86 to 14.38 [Abdulla J, Nielsen JR. Europace 2009]. A longitudinal study of a large cohort of cross-country skiers showed that not only do these athletes have an increased risk of developing AF, but their risk also increased in a “dose-response” manner—for example, with the number of races in which they participated per year and their performance [Andersen K et al. Eur Heart J 2013].
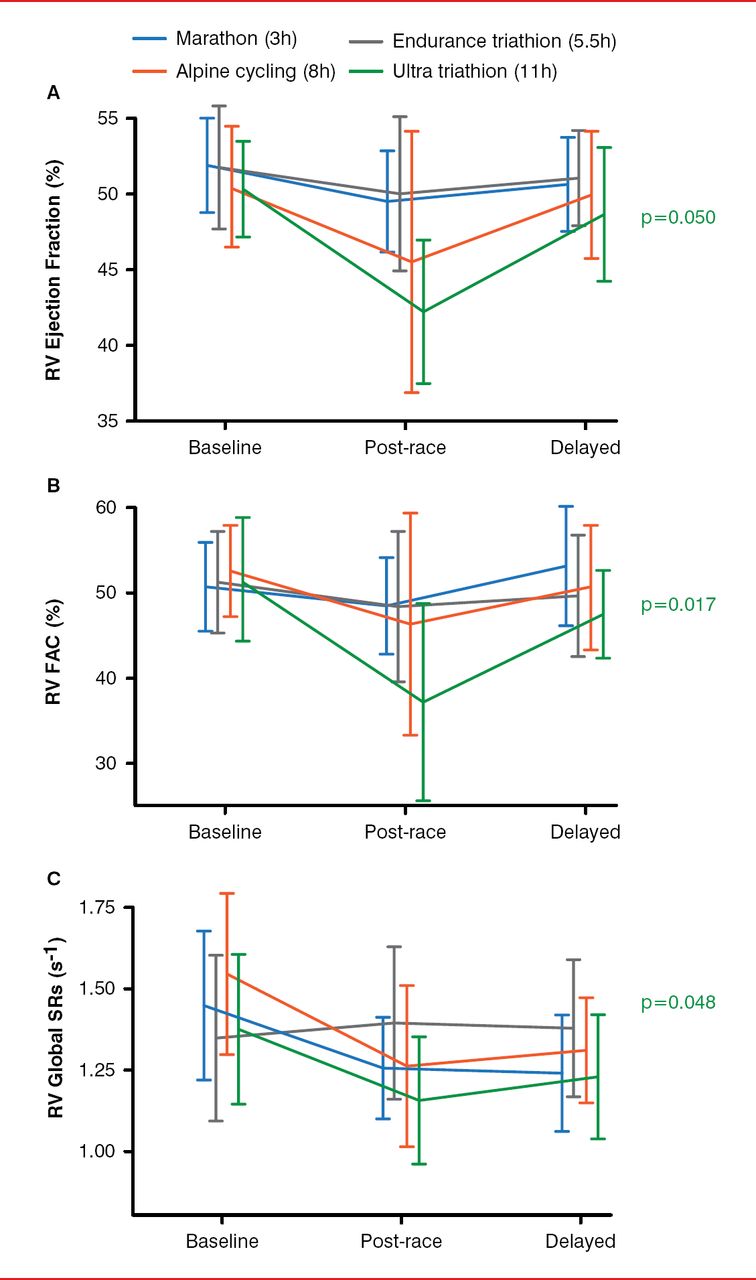
The mechanism for the increased risk of AF in athletes has been speculated to be increased atrial pressure and atrial dilatation as well as shorter refractory periods. In a study based on echocardiograms performed before, immediately following, and 2 weeks after a race, researchers found that the right ventricle (RV) dilates more than the left ventricle (LV), resulting in a higher RV volume with a lower systolic volume [La Gerche A et al. Eur Heart J 2012]. These changes were associated with gadolinium enhancement in the interventricular septum on cardiac magnetic resonance imaging in 12.8% of patients. By 2 weeks after the race, these changes returned to near baseline (Figure 1). In addition, troponin and N-terminal pro-brain natriuretic peptide levels were elevated in the athletes, which corresponded with RV dysfunction. Interestingly, the change from baseline was greatest in patients whose sport required more endurance.
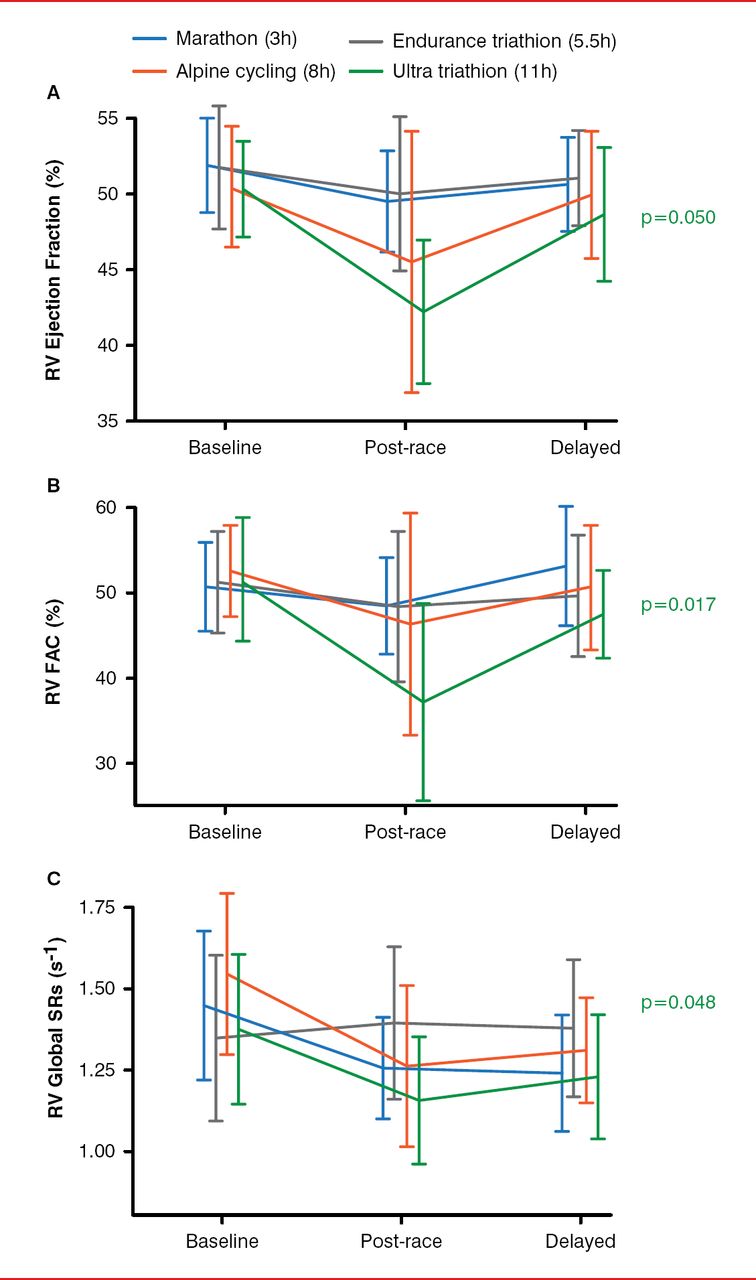
Changes in RV in Endurance Athletes During a Competitive Event
FAC=fractional area change; RV=right ventricle/ventricular; SR=strain rate.
Reproduced from Gerche A et al. Exercise-induced right ventricular dysfunction and structural remodelling in endurance athletes. Eur Heart J 2012;33:998–1006. With permission from Oxford University Press.
In the nonathlete, data from the Physicians' Health Study did not show a significant increase in AF risk in men who habitually performed vigorous exercise when body mass index (BMI) and blood pressure were not taken into account [Aizer A et al. Am J Cardiol 2009]. However, men who went jogging showed an increased risk of developing AF that was associated with frequency of jogging per week (trend p<0.01). Dr. Albert concluded by stating that risk of AF appears to be associated with long-term vigorous exercise—particularly, endurance sports. However, moderate exercise reduces the risk of AF, likely as a result of lowering BMI.
T. Jared Bunch, MD, Intermountain Medical Center, Salt Lake City, Utah, USA, discussed the effect of supplements on AF. Many patients with AF take supplements. Importantly, 9 of the 10 most commonly used supplements decrease international normalized ratio (coenzyme Q10, multiherbs, soy) or increase it (glucosamine, chondroitin, essential fatty acids, melatonin, cranberry, antioxidants). In addition, patients who take supplements are more likely to be noncompliant with warfarin and typically are not aware of warfarin-supplement interactions [Smith MB et al. Circulation 2009 (abstr 1116)]. Furthermore, ∼60% of patients taking warfarin for AF used vitamins—with multivitamin products, vitamin C, vitamin D, and vitamin E the most common [Smith MB et al. Cardiology 2010]. Dr. Bunch pointed out that these data indicate that physicians need to educate their patients about supplement and vitamin use.
Data from the Framingham Heart Study showed that caffeine intake was not associated with AF, even when patients regularly consumed up to 1000 mg/d [Frost L, Vestergaard P. Am J Clin Nutr 2005]. Other dietary factors not associated with increased risk of AF were fiber, fish intake, and alcohol consumption, as well as energy drinks; however, energy drinks did result in a prolonged QT interval [Shah SA et al. Circulation 2013 (abstr P324)]. In addition, serum vitamin D levels above 100 were associated with increased risk of AF (HR, 2.51; p=0.003) [Smith MB et al. Circulation 2011 (abstr 14699)].
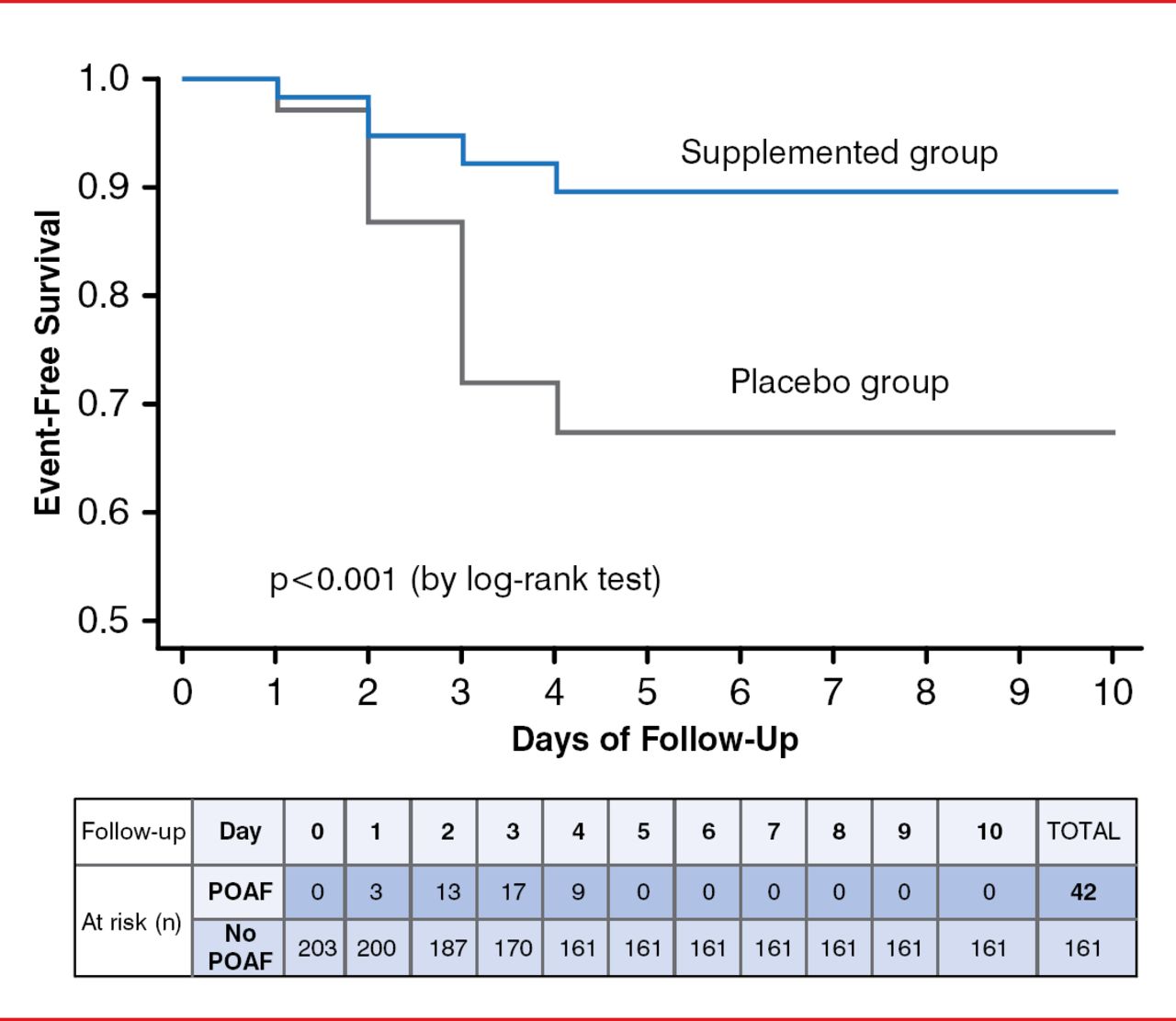
In a randomized placebo-controlled study of patients who supplemented with eicosapentaenoic and docosahexaenoic acids (omega-3 fatty acid fish oil antioxidants; 1:2 ratio), vitamin C (1 g/day), and vitamin E (400 IU/day) before on-pump cardiac surgery, patients who supplemented had a significantly higher rate of event-free survival compared with the placebo group (log-rank p<0.001; Figure 2) [Rodrigo R et al. J Am Coll Cardiol 2013]. However, a randomized placebo-controlled study of omega-3 fatty acid supplementation demonstrated no effect on survival-free recurrence of AF [Macchia A et al. J Am Coll Cardiol 2013].
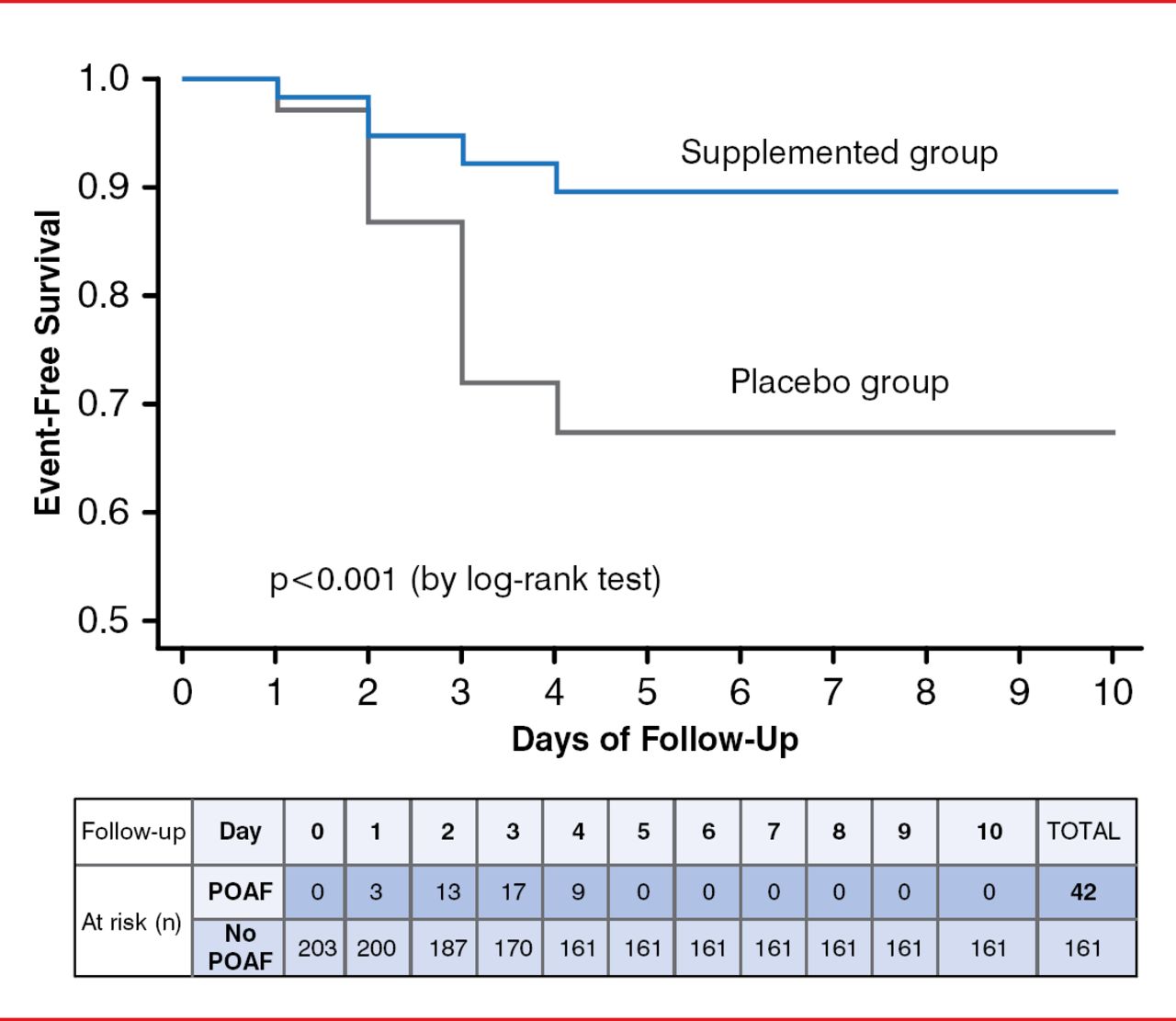
Effect of Antioxidant Supplementation on Atrial Fibrillation Occurrence
POAF=postoperative atrial fibrillation.
Reproduced from Roidrigo R et al. A randomized controlled trial to prevent post-operative atrial fibrillation by antioxidant reinforcement. J Am Coll Cardiol 2013;62:1457–1465. With permission from Elsevier.
Sumeet S. Chugh, MD, Cedars-Sinai Medical Center, Los Angeles, California, USA, presented the role of the treatment of sleep apnea in the prevention of AF. Observational studies have suggested that there is an association between obstructive sleep apnea (OSA) and AF. In one study, 49% of cardiology patients with AF had OSA, compared with 32% of patients without AF (p=0.0004); the OR was 2.19 (95% CI, 1.40–3.42; p=0.0006) after adjustment for BMI, neck circumference, hypertension, and diabetes mellitus [Gami AS et al. Circulation 2004]. In addition, researchers of a retrospective cohort study of more than 3500 patients found that over a median 4.7 years of follow-up, the frequency of AF was greatest in patients with OSA compared with patients without OSA [Gami AS et al. J Am Coll Cardiol 2007]. Another study revealed that as hypoxemia increased in patients with OSA, so did risk of AF [Tanigawa T et al. Heart 2006]. However, some studies have found no association between OSA and AF and between age-, sex-, and cardiovascular morbidity-matched AF cases and controls [Porthan KM. Chest 2004].
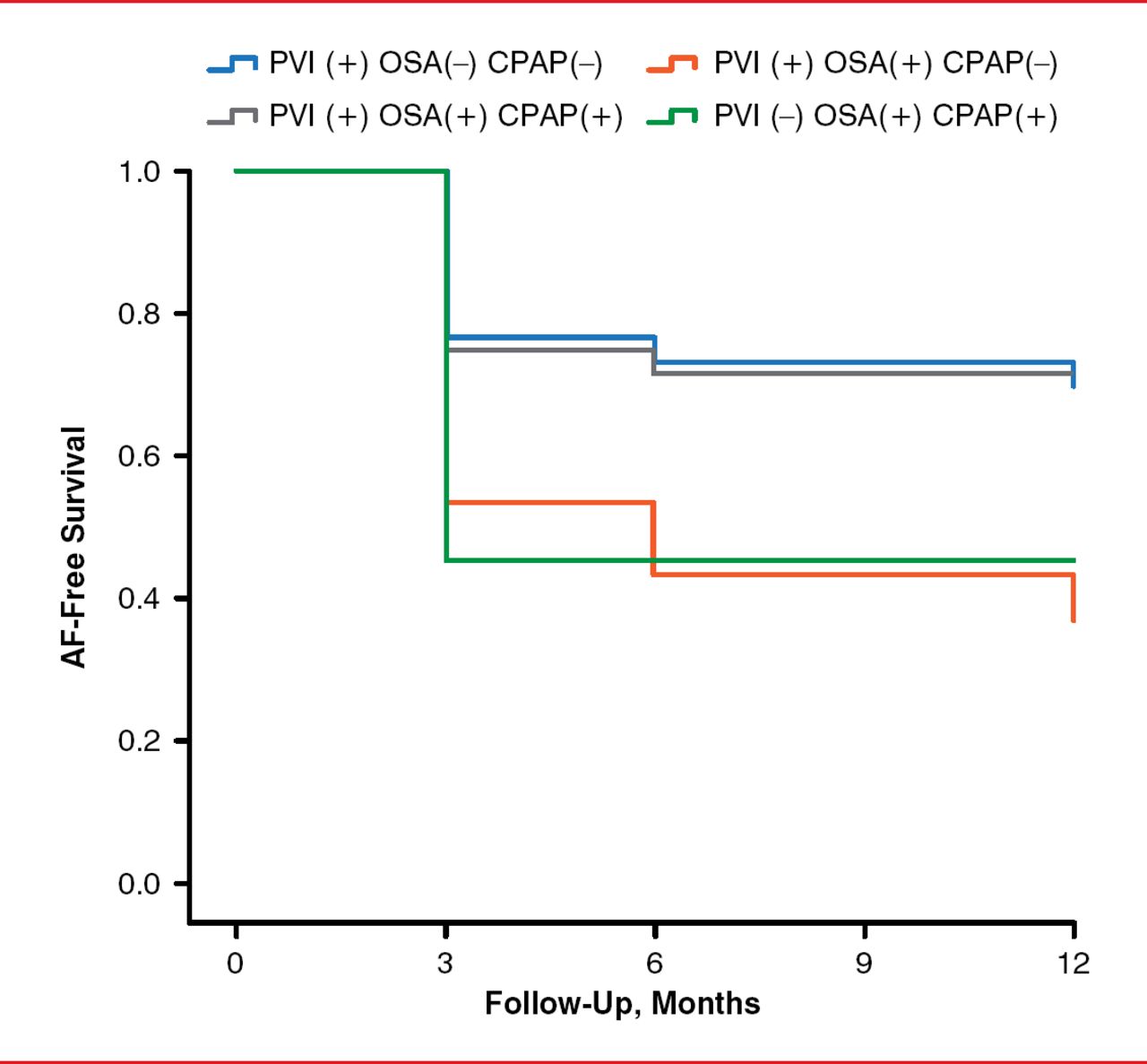
Yet, in a study of patients who experienced an acute episode of AF, treatment of diagnosed OSA with continuous positive airway pressure (CPAP) resulted in no significant difference in reductions in AF recurrence compared with control patients and patients with untreated OSA [Kanagala R et al. Circulation 2003]. A recent study showed that treatment of OSA with CPAP reduced the risk of AF recurrence in patients who underwent catheter ablation, similar to that of patients without OSA (Figure 3). For patients who underwent pulmonary vein isolation (PVI) and had OSA, their risk of recurrence was lower if they used CPAP than if they did not use it. In fact, if they underwent PVI and used CPAP, their risk was similar to that of patients without OSA. Patients with OSA who underwent catheter ablation and did not receive CPAP treatment had similar rates of AF recurrence as patients with OSA who did not undergo catheter ablation [Fein AS et al. J Am Coll Cardiol 2013].
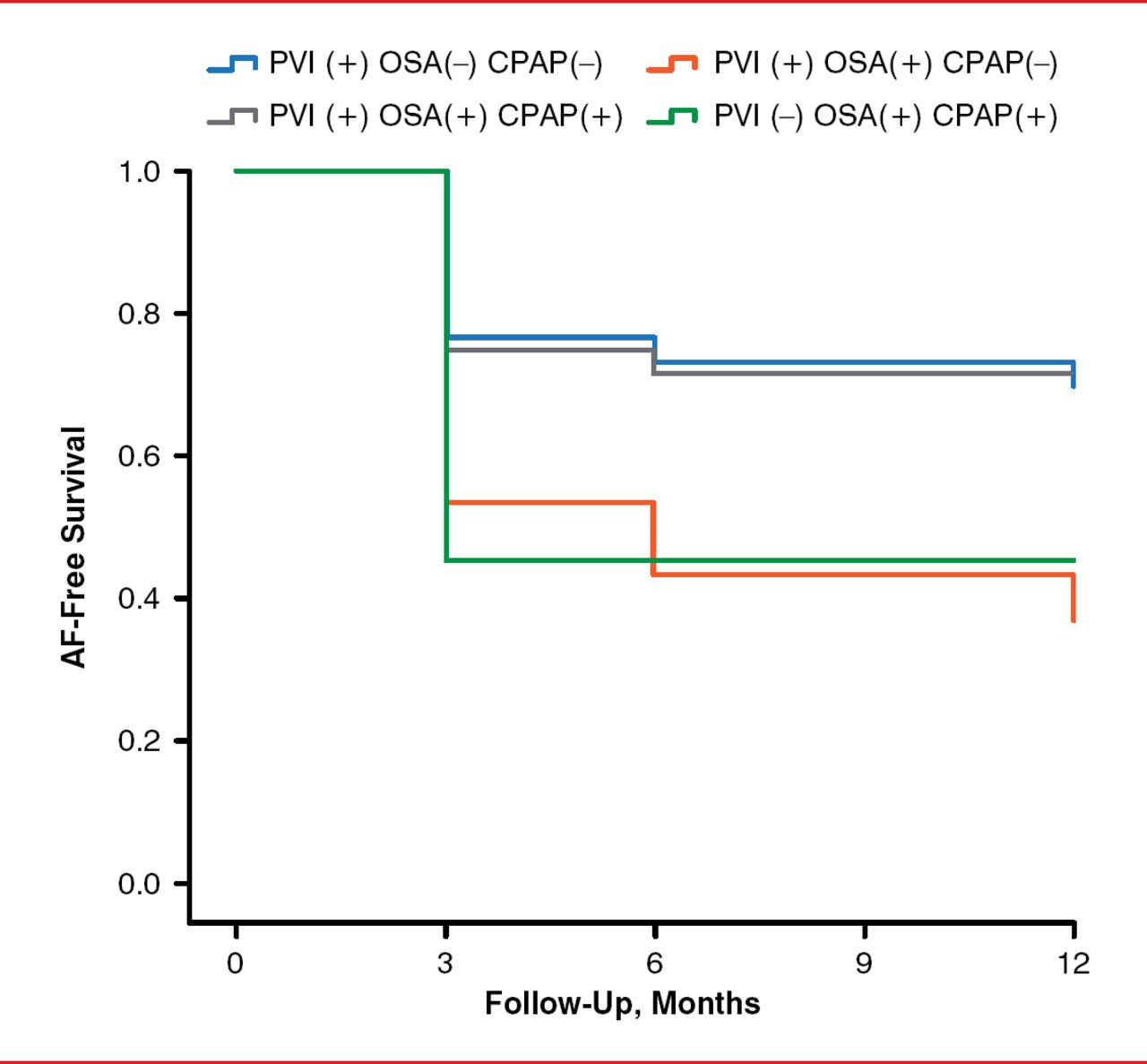
Effect of CPAP Treatment of OSA on AF-Free Survival
AF=atrial fibrillation; CPAP=continuous positive airway pressure; OSA=obstructive sleep apnea; PVI=pulmonary vein isolation.
Reproduced from Fein AS et al. Treatment of obstructive sleep apnea reduces the risk of atrial fibrillation recurrence after catheter ablation. J Am Coll Cardiol 2013;62:300–305. With permission from Elsevier.
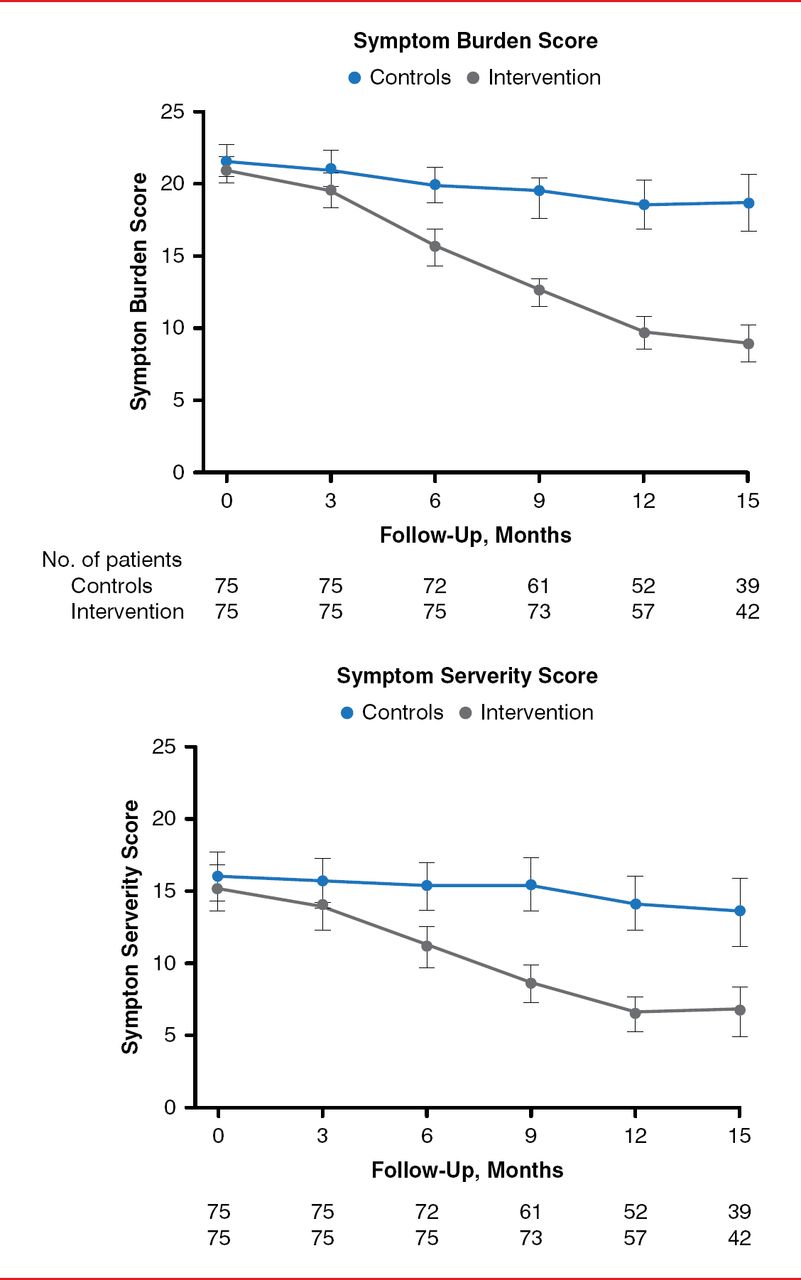
John D. Day, MD, Intermountain Medical Center, Salt Lake City, Utah, USA, discussed cultures lifestyle and psychosocial interventions. A recent study of 438 patients with a BMI ≥43 showed that after 7.2 years, AF occurrence was significantly lower in patients who underwent bariatric surgery (6.4%) compared with those who did not undergo surgery (16.1%; p<0.01) [Cha YM et al. HRS 2014 (abstr PO01–187)]. This was about a 4-fold increase in prevalence of AF in patients who did not undergo bariatric surgery. Dr. Day highlighted that this study suggests that AF is not a “life sentence” but is reversible. A trial of 150 patients with a BMI >27 who had symptomatic AF were randomly assigned to receive weight loss advice or participate in a weight loss program and were followed for 15 months. Patients who participated in the program lost an average of 32 pounds, whereas patients who received advice lost an average of 8 pounds [Abed HS et al. JAMA 2013]. Similarly, patients who participated in the program had a greater reduction in AF symptoms, C-reactive protein levels, blood pressure, lipids, insulin and glucose levels, and left atrial size (Figure 4). Dr. Day pointed out that even the group that received advice had a decrease in AF symptoms.
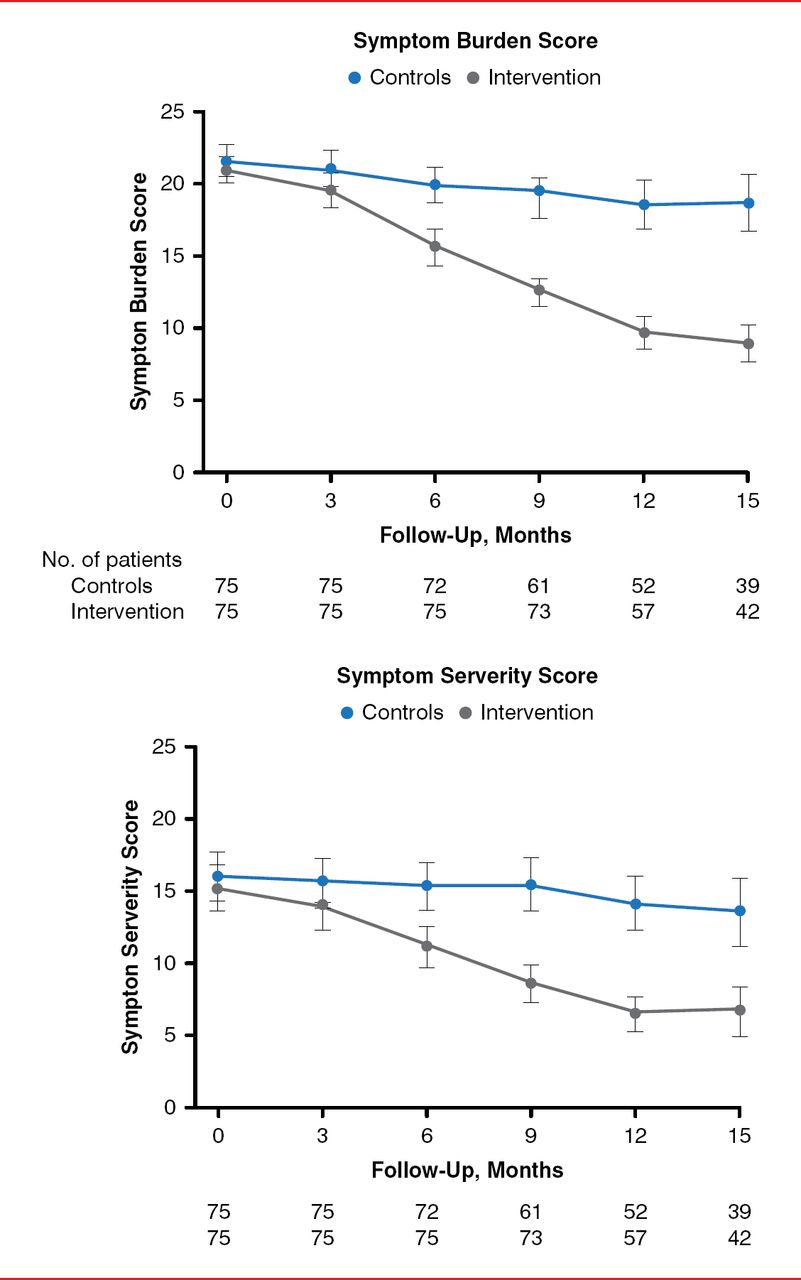
Atrial Fibrillation Symptoms Following Weight Loss
Reproduced from Abed HS et al. Effect of weight reduction and cardiometabolic risk factor management on symptom burden and severity in patients with atrial fibrillation: a randomized clinical trial. JAMA 2013;310:2050–2060. © 2013 American Medical Association. All rights reserved.
Although the prevalence of AF is rising, moderate exercise and improved diet resulting in weight loss may have a beneficial effect on the development and recurrence of AF and may decrease AF symptoms. Studies are ongoing of the mechanisms underpinning the benefit of these lifestyle changes and the potential adverse effects of intensive exercise and OSA that lead to AF. Historically taught triggers of AF, such as excessive caffeine intake, may not be as impactful as once thought.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.