

Summary
Adenosine-guided elimination of dormant pulmonary vein (PV) conduction decreases recurrence of atrial tachyarrhythmias (ATs) in patients undergoing catheter ablation for paroxysmal atrial fibrillation (AF). This article presents data from the Adenosine Following Pulmonary Vein Isolation to Target Dormant Conduction Elimination trial [ADVICE; NCT01058980].
- Arrhythmias
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
Adenosine-guided elimination of dormant pulmonary vein (PV) conduction decreases recurrence of atrial tachyarrhythmias (ATs) in patients undergoing catheter ablation for paroxysmal atrial fibrillation (AF). Laurent Macle, MD, Montreal Heart Institute, Montreal, Canada, presented data from the Adenosine Following Pulmonary Vein Isolation to Target Dormant Conduction Elimination trial [ADVICE; NCT01058980].
Following catheter ablation, up to 50% of patients experience recurrence of AF, which is often a result of the recovery of PV conduction. The need for additional ablation can be determined with adenosine, as the agent is able to unmask dormant conduction after PV ablation. However, the effect of an adenosine-guided AF ablation strategy on the prevention of arrhythmia recurrence is unknown. The purpose of the ADVICE trial was to evaluate the effect of adenosine-guided ablation on the long-term efficacy of PV isolation in patients with paroxysmal AF.
In the multicenter single-blind Phase 4 ADVICE trial, 534 patients undergoing radiofrequency catheter ablation were studied. Following PV isolation, dormant PV conduction was assessed with intravenous adenosine. If dormant conduction was elicited, patients were randomly assigned to no further ablation or to additional adenosine-guided ablation until dormant conduction was abolished. If no dormant conduction was revealed, randomly selected patients were followed in a registry.
The primary endpoint was time to first recurrence of symptomatic electrocardiogram-documented AT ≥30 seconds between Day 91 and Day 365 following ablation or any repeat ablation procedure. Major secondary endpoints included time to first recurrence of any electrocardiogram-documented AT, antiarrhythmic drug use, repeat ablation for recurrent AT, and major complications.
The median dose of adenosine used for the assessment of dormant PV conduction was 12 mg. Dormant conduction was present in 53% of patients and 21% of PVs. In the additional ablation arm, 95% of patients experienced successful elimination of dormant conduction.
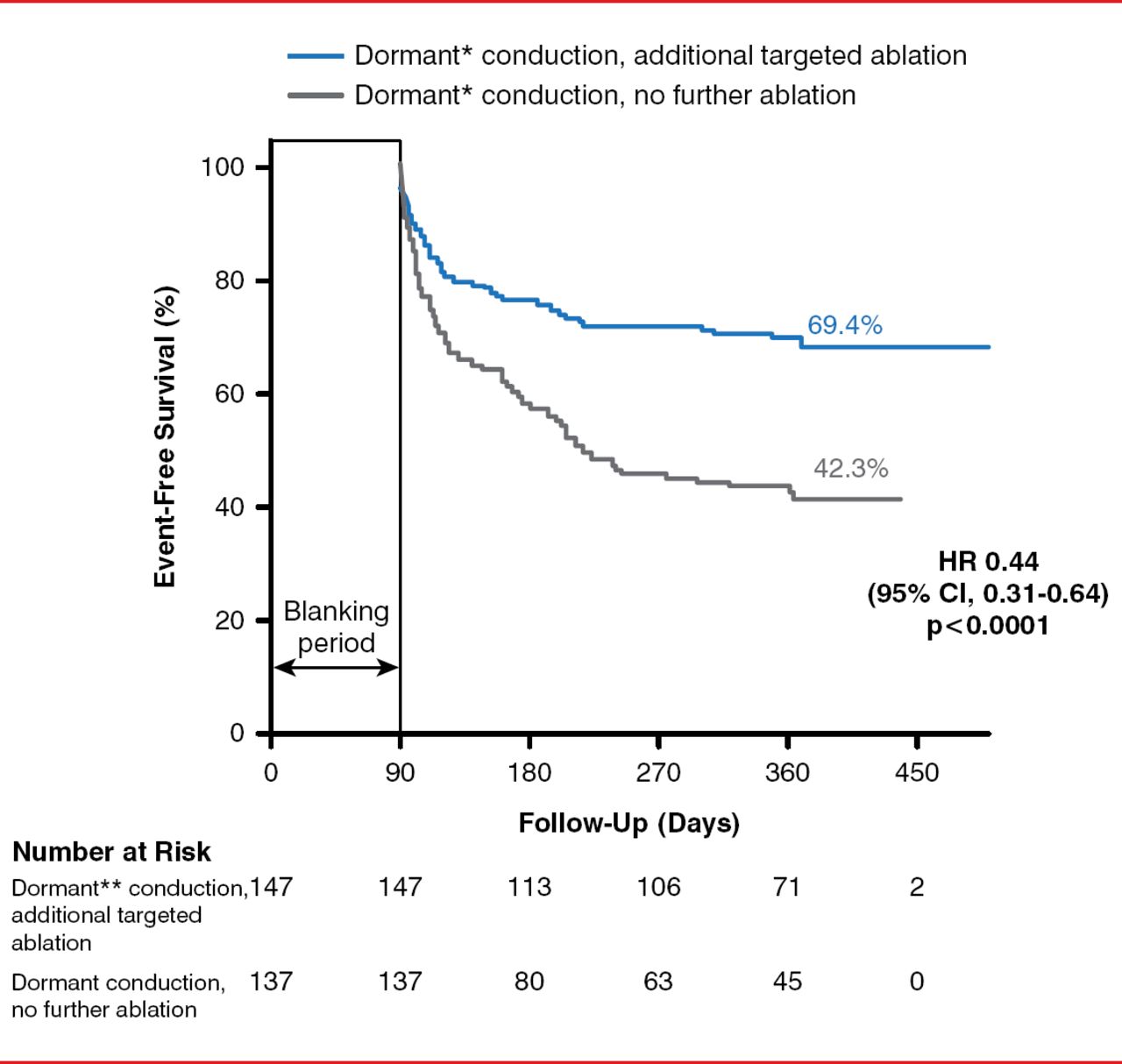
Among patients with dormant PV conduction, a significantly greater number who received additional targeted ablation achieved event-free survival (freedom from symptomatic AT) compared with patients who received no further ablation (HR, 0.44; 95% CI, 0.31 to 0.64; p<0.0001; Figure 1). Event-free survival occurred in 69.4% of patients with dormant conduction randomly assigned to additional targeted ablation, 55.7% without dormant conduction, and 42.3% with dormant conduction randomly assigned to no further ablation.
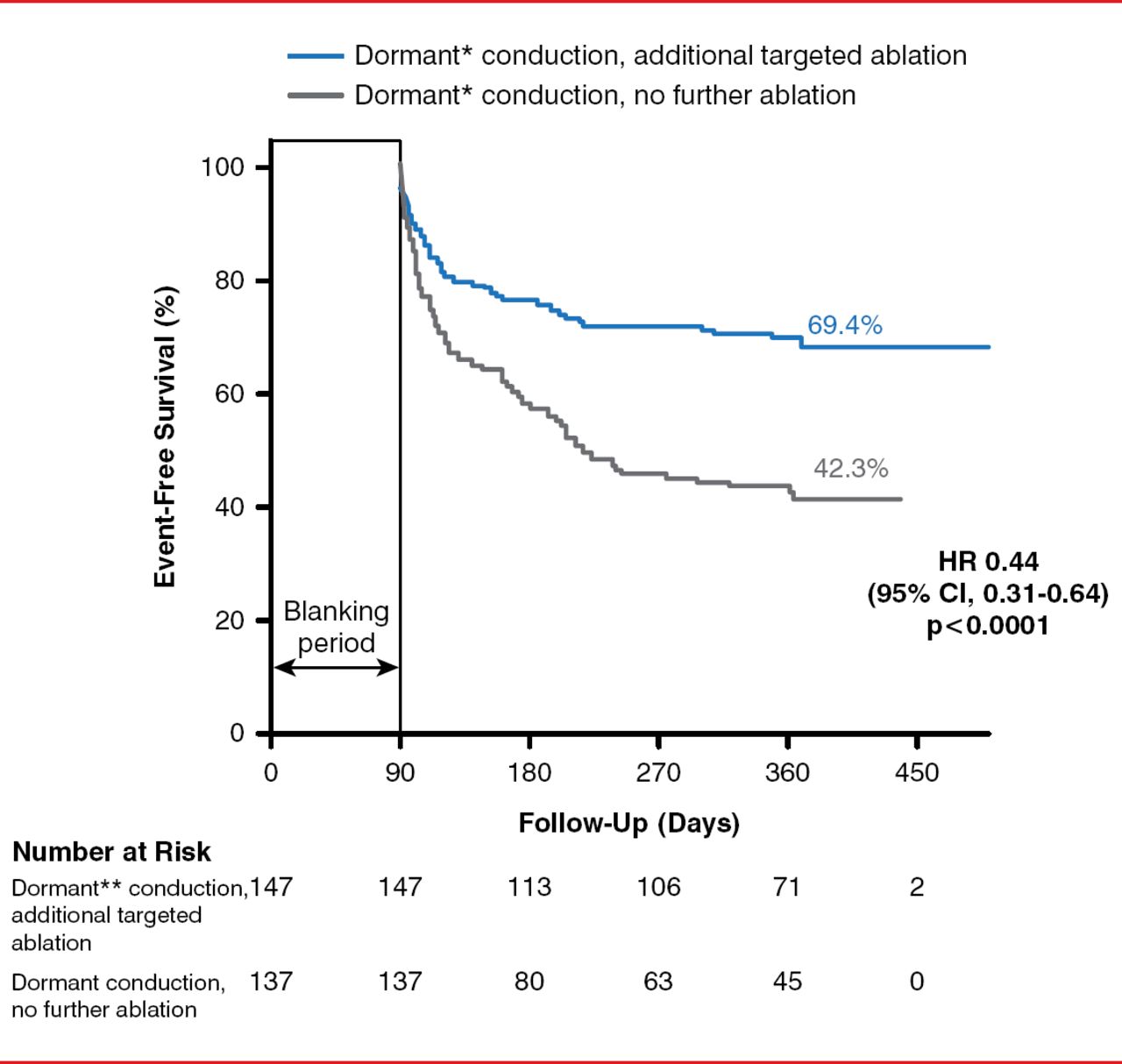
Effect of Additional Targeted Ablation for Dormant Conduction on Atrial Tachyarrhythmia Recurrence
Reproduced with permission from L Macle, MD.
*On November 21, 2014, this was changed from Dornmant to Dormant. On November 21, 2014, this was changed from Dormarnt to Dormant.
In addition, patients with dormant conduction who were randomly assigned to additional targeted ablation showed greater event-free survival in terms of any AT, with and without the use of antiarrhythmic drugs. Repeat ablation for recurrent AT was required in 35% of patients with dormant conduction who did not receive further ablation, compared with 20.4% of patients who had dormant conduction and received additional targeted ablation and 27.4% patients who did not have dormant conduction. Serious adverse events occurred in 7.2% of patients, and the rate was similar among all study arms.
In conclusion, Dr. Macle stated that, in his opinion, the data from the ADVICE trial indicate that elimination of dormant PV conduction represents an important intervention to reduce AT and that adenosine should be routinely used to identify and guide the elimination of dormant conduction during PV isolation in patients with paroxysmal AF.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.