

Summary
Evidence to date suggests that surgical treatment can improve pain and disability in adults with symptomatic spinal deformity. However, most previous studies were small, retrospective series without direct comparisons with nonoperative treatment approaches. The aim of this study, Outcomes of Operative and Nonoperative Treatment for Adult Spinal Deformity (ASD): A Prospective, Multicenter Matched and Unmatched Cohort Assessment with Minimum Two-Year Follow-up was to compare minimum 2-year outcomes for operative and nonoperative treatment for ASD in a prospective population, using both matched and unmatched cohorts.
- Orthopaedics Clinical Trials
- Spine Conditions
- Orthopaedic Procedures
- Orthopaedics Clinical Trials
- Spine Conditions
- Orthopaedics
- Orthopaedic Procedures
Evidence to date suggests that surgical treatment can improve pain and disability in adults with symptomatic spinal deformity. However, most previous studies were small, retrospective series without direct comparisons with nonoperative treatment approaches. The aim of this study, Outcomes of Operative and Nonoperative Treatment for Adult Spinal Deformity (ASD): A Prospective, Multicenter Matched and Unmatched Cohort Assessment with Minimum Two-Year Follow-up [Smith JS et al. Spine. 2014], presented by Justin S. Smith, MD, PhD, University of Virginia Health System, Charlottesville, Virginia, USA, was to compare minimum 2-year outcomes for operative and nonoperative treatment for ASD in a prospective population, using both matched and unmatched cohorts.
The patients (n = 689) were recruited from a multicenter database for ASD through the International Spine Study Group. They were classified as operative (n = 286) or nonoperative (n = 403) based on the initial management approach. At baseline and follow-up, the patients completed health-related quality of life (HRQOL) measures, including the Scoliosis Research Society Questionnaire-22 (SRS-22), Oswestry Disability Index (ODI), Short Form-36 Health Survey (SF-36) physical component score (PCS), and measures of back and leg pain.
Included patients (aged > 18 years) had a diagnosis of ASD and at least one of the following: coronal Cobb angle ≥ 20°, sagittal vertical access > 5 cm, pelvic tilt ≥ 25°, and thoracic kyphosis ≥ 60°. Outcomes were compared within and between surgical and nonsurgical groups using unmatched and propensity-matched cohorts. The propensity-matched cohort was matched according to baseline ODI, SRS-22, leg pain score, pelvic incidence-lumbar lordosis (PI-LL) mismatch, and maximum thoracolumbar/lumbar Cobb angle.
At baseline, patients in the operative group (n = 246) had significantly worse HRQOL measures (P < .001) and mean body mass index (P = .003) compared with those in the nonoperative group (n = 223). The operative group also had significantly worse mean coronal balance (P < .001), sagittal balance (P < .001), pelvic tilt (P = .002), and PI-LL (P < .001) at baseline.
At a minimum 2-year follow-up, for unmatched outcomes, patients in the operative group (n = 246) had significant improvements from baseline in ODI (P < .001), SF-36 score (P < .001), SRS-22 score (P < .001), numeric rating scale (NRS) back pain score (P < .001), and NRS leg pain score (P < .001), whereas the nonoperative group (n = 223) had no significant improvements from baseline in these measures (Table 1). The operative group had significantly improved mean back pain score compared with the nonoperative group (P = .001).
Impact of Nonoperative vs Operative Treatment on Outcomes
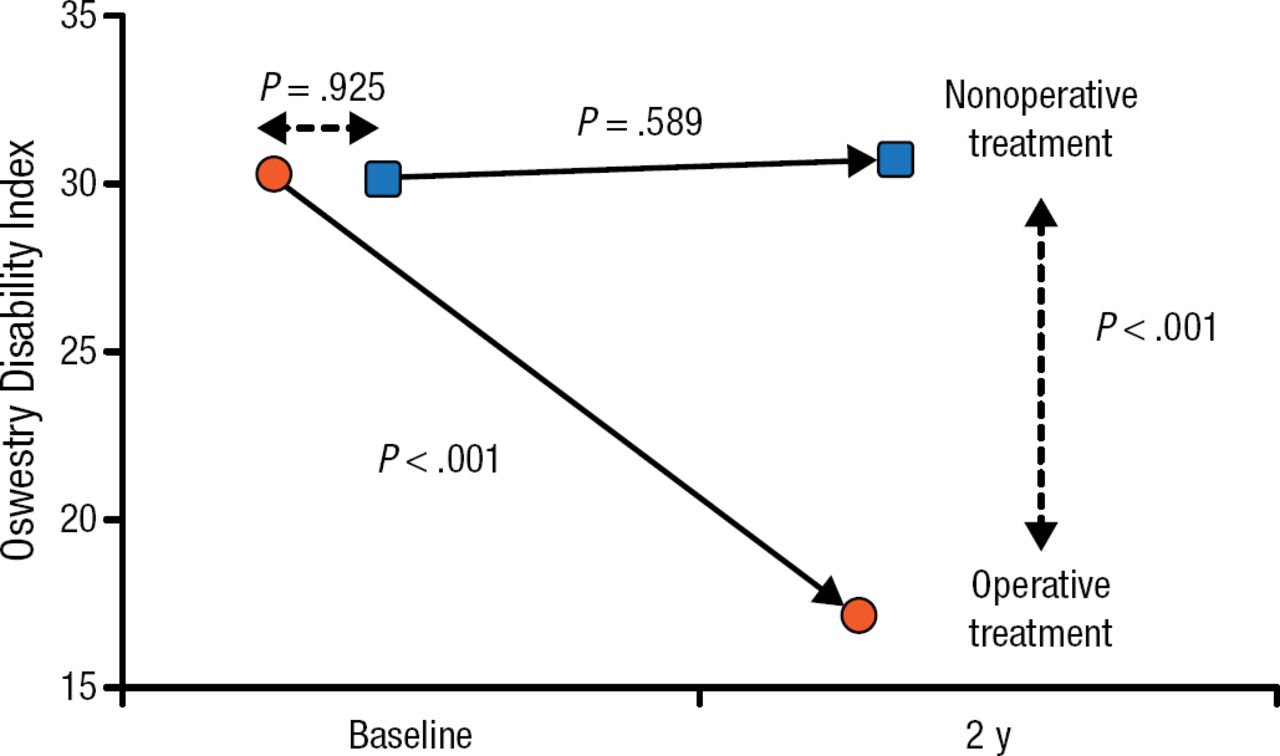
A total of 97 matched operative-nonoperative pairs were identified based on propensity scores. The only parameter that was significantly different between the operative and nonoperative pairs was mean age (51.4 vs 58.0; P = .003). Among the matched pairs, the operative group had significant improvements from baseline and vs the nonoperative group in ODI score (P < .001 both comparisons; Figure 1), SRS-22 total score (P < .001 both comparisons), SF-36 PCS (P < .001 both comparisons), back pain score (P < .001 both comparisons), and leg pain score (P < .001 both comparisons). The nonoperative group lacked significant improvements from baseline in any of the measures, except for the SRS-22 (P = .021).
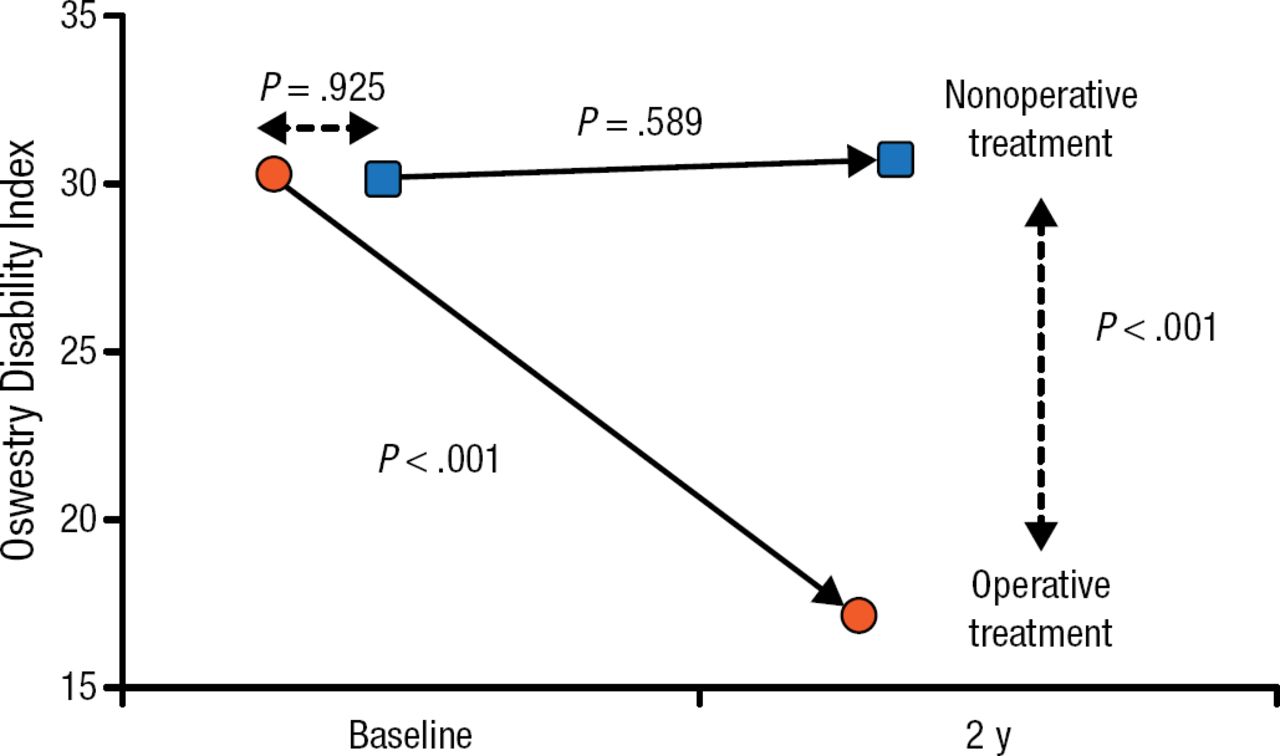
Operative vs Nonoperative Treatment: Impact on Disability
Data are presented for 97 propensity-matched operative-nonoperative pairs. P values were calculated with the paired t test.
Reproduced with permission from JS Smith, MD, PhD.
Patients electing nonoperative treatment tend to have less deformity and less pain and disability than patients choosing to undergo surgery. Surgical treatment for ASD can provide significant improvements in HRQOL at a minimum 2-year follow-up. Nonoperative treatment appears to maintain presenting levels of pain and disability.
- © 2015 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.