

Summary
Management of pain following spinal surgery is important not only for patient outcomes but also for improving costs, complication rates, and patient experiences. In this session, presenters reviewed current guidelines and recommendations, the use of perioperative epidurals, ways to reduce tissue injury, and characteristics of current medications used postoperatively for spinal surgery.
- Analgesic Drugs
- Pain Management
- Acute & Chronic
- Orthopaedic Procedures
- Orthopaedic Pain Management
- Spine Conditions
- Analgesic Drugs
- Pain Management
- Acute & Chronic
- Orthopaedic Procedures
- Orthopaedic Pain Management
- Spine Conditions
- Orthopaedics
Management of pain following spinal surgery is important not only for patient outcomes but also for improving costs, complication rates, and patient experiences. In this session, presenters reviewed current guidelines and recommendations, the use of perioperative epidurals, ways to reduce tissue injury, and characteristics of current medications used postoperatively for spinal surgery.
Daniel K. Resnick, MD, MS, University of Wisconsin, Madison, Wisconsin, USA, discussed current ideas and recommendations for pain management. He presented information on the ERAS Society guidelines, which were developed based on work with colorectal surgery and to use evidence-based approaches to improve patient outcomes—namely, enhanced recovery after surgery (ERAS). While there is evidence supporting the ERAS guidelines, Dr Resnick noted that the reviews vary substantially in certain variables (eg, protocols and outcome definitions) and that length of hospital stay varied considerably, making it more difficult to draw conclusions. He also discussed the limitations in the evidence underlying the ERAS guidelines and emphasized that conclusions from colorectal surgery may not always be applicable to other types of surgery.
After discussing some other general efforts to improve outcomes, Dr Resnick addressed options from literature, including using lower doses of multiple medications and using preemptive analgesia. He noted that multimodal approaches for pain control have produced promising outcomes, including reduced narcotic use. Epidural analgesia showed promise in 1 randomized clinical trial; however, the research is limited [Kjærgaard M et al. Acta Anaesthesiol Scand. 2012].
To conclude, Dr Resnick reiterated the importance of effective pain control and to realize that patients are heterogeneous. He also noted that hospitals most likely will require formal protocols and that pressure to reduce narcotic use will continue.
Michael P. Steinmetz, MD, Case Western Reserve University, Cleveland, Ohio, USA, presented an overview of the clinical practice guidelines for perioperative pain management from the American Society of Anesthesiologists Task Force on Acute Pain Management [Apfelbaum JL et al. Anesthesiology. 2012]. The aims of the guidelines include decreasing the risk of adverse outcomes and improving patient outcomes. Recommended institutional policies include the importance of educating personnel and using standardized instruments.
Dr Steinmetz also addressed recommended steps for preoperative evaluation, perioperative techniques, and populations of special concern (ie, pediatric patients, who are susceptible to over- and undertreatment, and geriatric patients, who tend to be stoic rather than request pain relief). Multimodal techniques should be used when possible. He concluded that these guidelines form a framework, that pain management should continue from the preoperative period until recovery, and that individualized/customized plans are most effective.
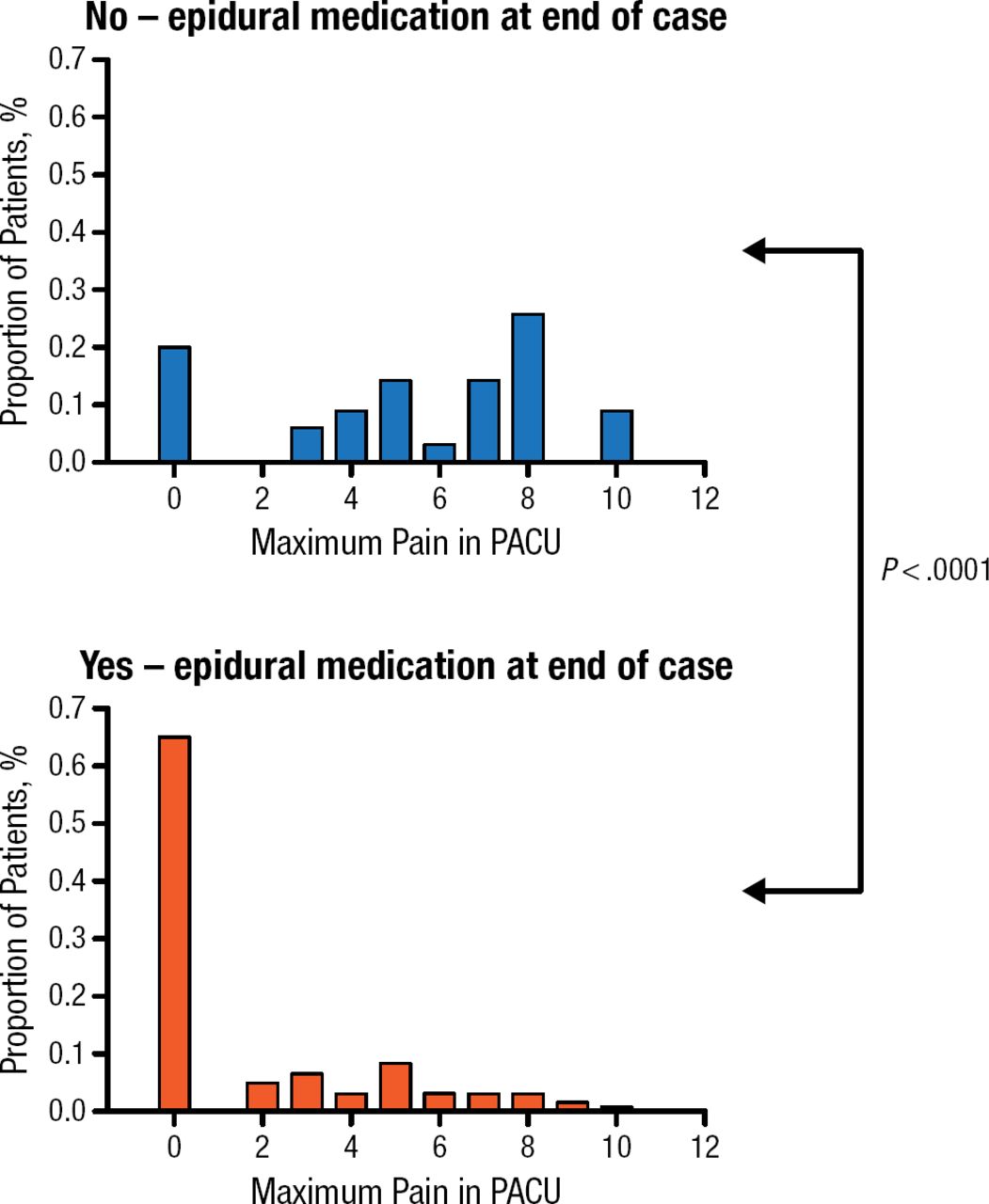
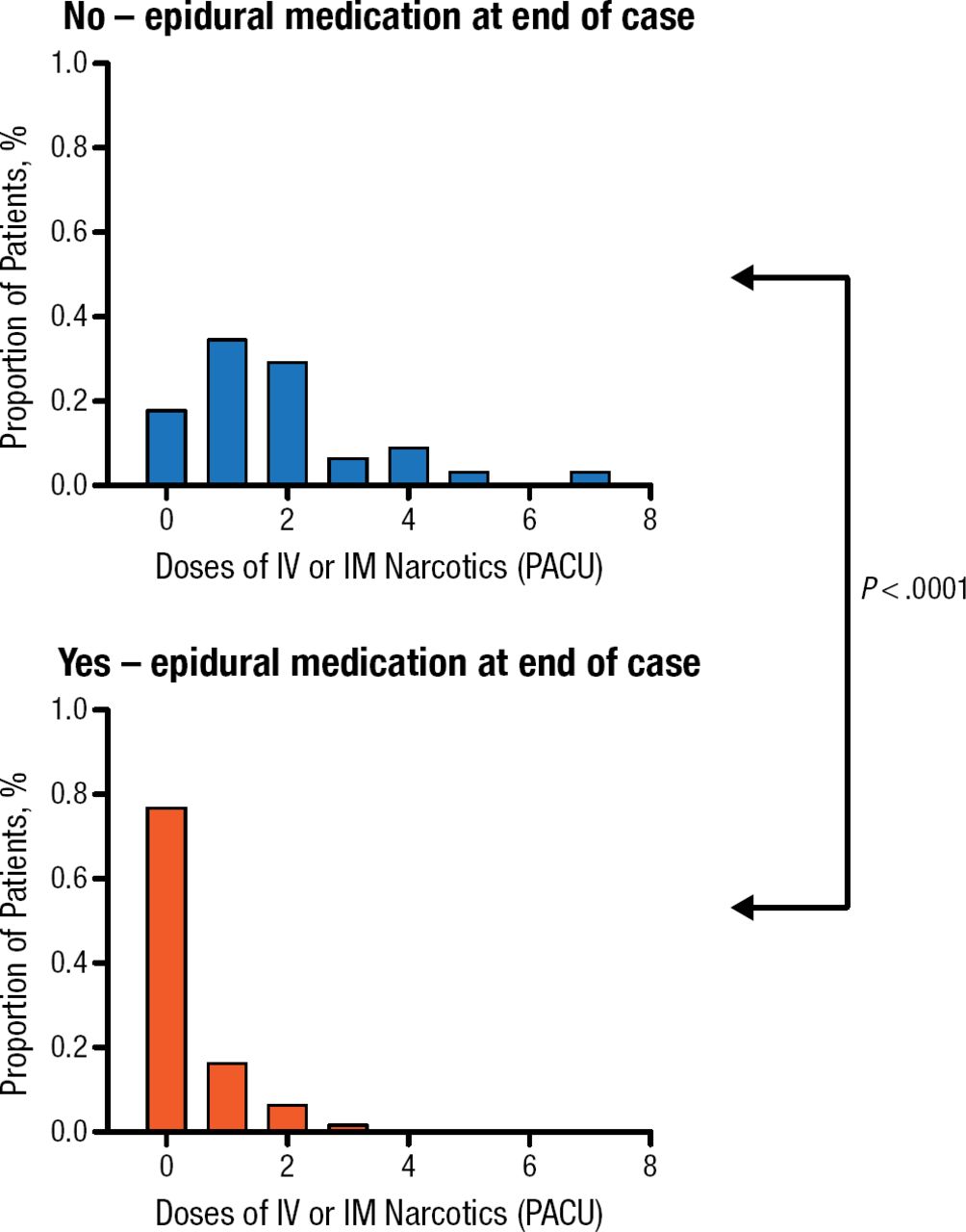
Fred H. Geisler, MD, PhD, Rhausler Inc, San Carlos, California, USA, presented data on the use of epidural local anesthetic and narcotic medications administered intraoperatively to aid in postoperative analgesia. After reviewing epidural medications in general and their use as operative anesthesia and postoperative analgesia, Dr Geisler presented the results of his cases [Geisler F. Spine J. 2009]. This consisted of 168 lumbar surgeries in which he compared maximum postoperative pain response and number of intravenous (IV) narcotic doses in the postanesthesia care unit (PACU) for patients who either did (n = 133) or did not (n = 35) receive an intraoperative epidural injection near the end of the procedure. All patients had postoperative pain managed in the PACU with intramuscular (IM) or IV narcotics as necessary. The differences between the 2 groups were striking and highly statistically significant, with 65% of patients who received an epidural having 0 out of 10 on the visual analog scale for pain in the PACU, which was significantly better than that of the IV or IM-narcotics-only group (P < .0001; Figure 1). Additionally, patients who had epidurals needed significantly fewer narcotic doses (P < .0001; Figure 2) in the PACU. Dr Geisler noted that it was important to make certain that patients had additional long-term pain relief medication added before the pain relief effects of the epidural medications diminished in a few hours. This analgesic drug-dosing plan represents the preemptive rather than reactive philosophy of pain management. He concluded by advising an increase in the use of intraoperative epidurals for pain relief following spinal surgery.

Maximum PACU Pain on the Visual Analog Scale (Out of 10)
PACU, postanesthesia care unit.
Adapted from The Spine Journal, Geisler F, 31. Intra-operative epidural anesthetic injection for control of immediate post operative pain in PACU after lumbar spinal surgery. 9:17S. Copyright (2009), with permission from Elsevier, Inc.

Number of PACU Narcotic Doses
IM, intramuscular; IV, intravenous; PACU, postanesthesia care unit.
Adapted from The Spine Journal, Geisler F, 31. Intra-operative epidural anesthetic injection for control of immediate post operative pain in PACU after lumbar spinal surgery. 9:17S. Copyright (2009), with permission from Elsevier, Inc.
Following the discussion of epidurals, Karthik Madhavan, MD, University of Miami, Miami, Florida, USA, presented an overview of nonopioid analgesic options, including perioperative anesthesia, nonsteroidal anti-inflammatory drugs (NSAIDs), IV acetaminophen, intraoperative analgesia, and local anesthesia. He provided detailed information on each (Table 1), including information from a pilot study of 16 patients who received bupivacaine liposome injectable suspension, resulting in less narcotic use and lower pain scores. While further studies are needed, the results of the pilot study suggest that bupivacaine liposome injectable suspension is effective but must be injected at more sites because it does not diffuse far from the injection site.
Nonopoid Analgesic Options
Choll W. Kim, MD, PhD, Spine Institute of San Diego, San Diego, California, USA, discussed surgical techniques and ways to reduce tissue damage and pain by using minimally invasive surgery (MIS). After explaining MIS and making clear that it is not defined by incision size, Dr Kim discussed ways to protect the multifidus muscle. He emphasized the importance of using table-mounted, non-self-retaining, tubular-type retractors because these exert less pressure than powerful, self-retaining retractors [Stevens KJ et al. J Spinal Disord Tech. 2006]. Additionally, open self-retaining retractors use continuous pressure, while table-mounted retractors do not. This means that the tissue is crushed for a shorter time with table-mounted retractors, reducing the risk of tissue injury [Kim KT et al. Spine (Phila PA 1976). 2006; Gejo R et al. Spine (Phila PA 1976). 2000].
In conclusion, Dr Kim stated that MIS decreases blood loss, infections, postoperative pain, and time in hospital. It is also likely that with MIS, there is faster recovery of function and lower overall costs.
The final presenter for this session was Christoph Hofstetter, MD, PhD, University of Washington, Seattle, Washington, USA. Dr Hofstetter described types of pain and highlighted that postsurgical pain is generally nociceptive, meaning that it is caused by noxious stimuli [Woolf CJ. Ann Intern Med. 2004]. Following discharge, about 80% of patients experienced acute pain after surgery [Apfelbaum JL et al. Anesth Analg. 2003].
Dr Hofstetter reviewed options for multimodal analgesia with analgesics, including acetaminophen, NSAIDs, opioids, muscle relaxants, gabapentin, and pregabalin. Both acetaminophen and NSAIDs have anti-inflammatory effects. However, while acetaminophen can cause hepatotoxicity, NSAIDs can cause renal injury, thrombotic events, gastrointestinal bleeding or perforation, and possible decrease in fusion rate (for ketorolac) [Li Q et al. Spine (Phila PA 1976). 2011]. While opioids may be the most effective option for the control of substantial pain (moderate to severe), they also can cause nausea, vomiting, respiratory depression, sedation, bowel effects, and pruritus. Knowledge of these risks and benefits is essential in determining the best option for each patient and in providing appropriate patient education.
- © 2015 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.