

Summary
The ObesityWeek 2014 keynote address focused on the foundation's strategies to reverse the childhood obesity epidemic.
- Pediatric Nutrition
- Obesity
- Pediatric Nutrition
- Obesity
- Endocrinology
- Diabetes & Metabolic Syndrome
James S. Marks, MD, MPH, Robert Wood Johnson Foundation (RWJF), Princeton, New Jersey, USA, delivered the ObesityWeek keynote address, which focused on the foundation's strategies to reverse the childhood obesity epidemic.
As a former director of the US Centers for Disease Control and Prevention's National Center for Chronic Disease Prevention and Health Promotion, Dr Marks spoke about how the RWJF came to focus on childhood obesity as a national health problem and how it strives to strategically work toward culture change specifically for the benefit of children.
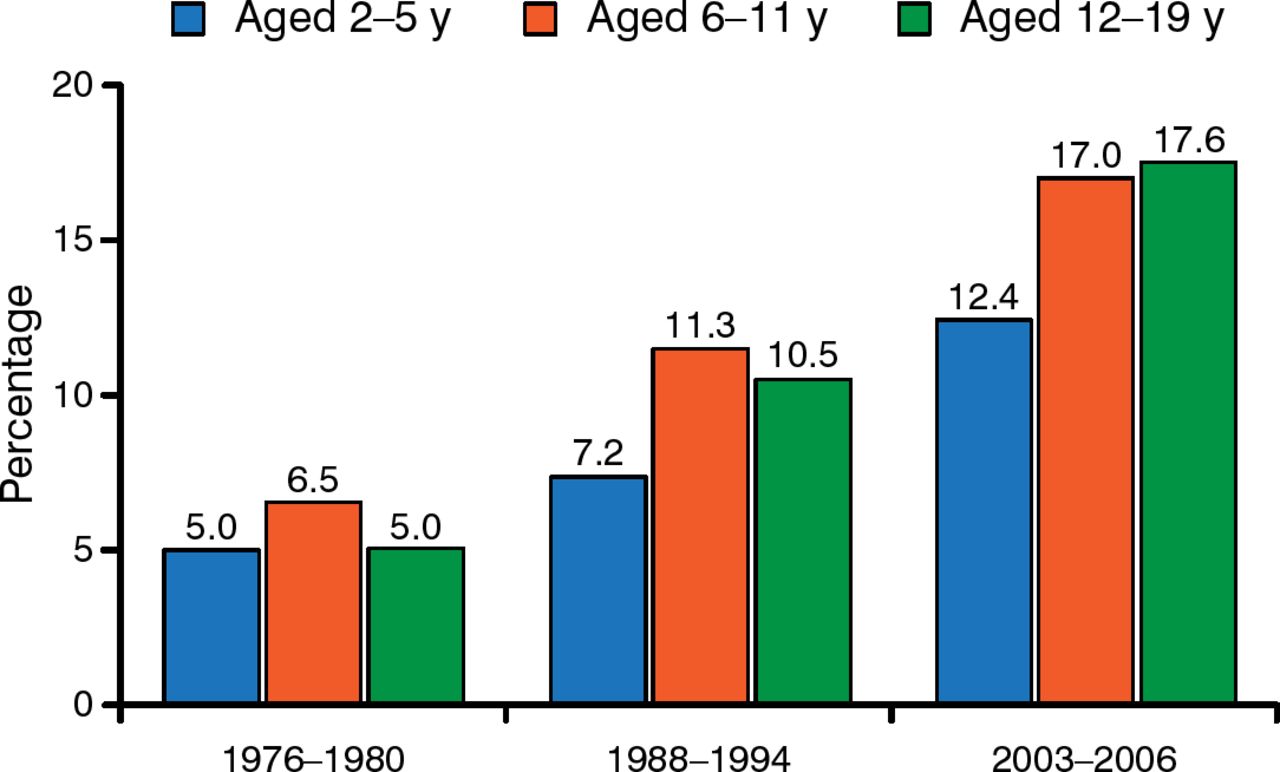
To highlight the impetus for the foundation's commitment to the problem, Dr Marks reviewed the prevalence of childhood obesity, which has increased dramatically over the past 3 decades (Figure 1). By the early 21st century, it became apparent that unless measures were undertaken to curb this trend, today's generation of children might be the first to “live sicker and die sooner” than their parents.

Prevalence of Obesity Among Children and Adolescents in the United States (1976–2006)
Obesity is defined according to sex- and age-specific body mass index ≥ 95th percentile, per the Centers for Disease Control and Prevention's growth charts.
Source: Overweight and Obesity, Centers for Disease Control and Prevention.
Adapted from Physiol & Behavior, 100, Hu FB et al. Sugar-sweetened beverages and risk of obesity and type 2 diabetes: Epidemiologic evidence, 47–54, Copyright 2010, with permission from Elsevier.
According to Dr Marks, the overall growth of obesity in the United States has been fueled by a series of gradual societal changes over time. These include a shift to less physical activity, the ready availability of more processed and calorie-laden foods, and a reduced consumption of fresh fruits and vegetables. He emphasized that progress in reversing all 3 of these trends will rely more on societal change than on clinical care and that children should be a key focus of these changes.
In 2004, the RWJF, along with ABC News and Time magazine, sought to focus public attention on the problem of childhood obesity by sponsoring a major obesity summit that brought the issue to the public and to policy influencers. In 2007, the foundation announced a goal of reversing the childhood obesity epidemic by 2015. It would prospectively invest $500 million to fund programs focused on:
-
improving the nutritional quality of snack foods and beverages offered in schools;
-
increasing access to healthy foods in communities;
-
providing local access to parks, playgrounds, and walking paths and other opportunities to be physically active;
-
reducing the consumption of sugary beverages;
-
publishing national reports on various elements of obesity; and
-
limiting the influence of food manufacturers and their products on children.
To augment its financial investment, the RWJF also made a commitment to investigate the creation of public and private partnerships likely to implement creative solutions to any or all of the announced initiatives.
While childhood obesity continues to be unacceptably high in the United States, Dr Marks presented data from the National Health and Examination Survey suggesting that, as of 2012, the prevalence of obesity in children between the ages of 2 and 11 years has leveled off and is now on the decline. He also highlighted data from Philadelphia and New York City (NYC) that have focused efforts on reversing childhood obesity, and he outlined the progress that these cities have made toward solving the problem.
NYC has reported substantial progress in decreasing obesity rates among children enrolled in kindergarten through eighth grade. Between 2006 and 2011, obesity rates dropped across all age ranges, poverty levels, neighborhoods, and racial and ethnic groups, with the largest decreases occurring among the youngest white and Asian students.
This encouraging trend was supported by a layering of community initiatives that included financial incentives to purchase fresh fruits and vegetables in farmers' markets among families receiving federal food benefit; in addition, 1000 mobile vending carts selling fresh produce increased access to healthy foods in city neighborhoods. In 2008, the city instituted nutritional standards for every city agency that purchases or serves meals. In 2009, the city's chain restaurants were required to prominently post calorie contents of items sold. The city has implemented “Active Design Guidelines,” which encourage architects and urban planners to design buildings that promote and support physical activity. The school board has charged school districts with serving healthier meals that include more fruits and vegetables and offer lower-fat milk options. NYC schools now offer a “Move to Improve” guideline, which promotes physical activity in the classrooms at times other than recess. NYC has also passed regulations that help younger children in day care centers receive more nutritious foods and more time for physical activity.
Dr Marks then highlighted the efforts in Philadelphia to curb childhood obesity. Between 2006 and 2010, obesity rates fell on average about 5%, with the overall decrease being slightly more prominent among black boys (7.6%) and Hispanic girls (7.4%). The city directly involved a wide range of partners that included schools, restaurants, as well as city and community agencies. In 2006, nutritional standards were set for snacks sold in school vending machines and à la carte lines. That same year, the Philadelphia School Reform Commission approved a school wellness policy that included healthier foods, nutrition education, and increased physical activity. Outside of school, more than 600 corner stores now offer fresh fruits and vegetables—facilitated in part by the city's interventions to help finance the refrigeration required to store the produce. The Pennsylvania Fresh Food Financing Initiative supported the development costs and startup for private sector supermarkets within the city, a model that has been replicated by the federal government.
According to Dr Marks, the promising results from these 2 cities demonstrate that if a city is able to implement these types of changes, their children will get healthier. Emphasizing that there is much more to be done and that the journey to “cure” obesity is in no way over, he described key future initiatives at the RWJF that will continue to address the problem. These include closing disparity gaps among minority children, bringing increased attention to pregnant women and young children, building public interest in demanding healthy changes, and fostering greater collaboration among public health, the health care sector, and social services.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.