

Summary
For people who experience an out-of-hospital cardiac arrest (OHCA), prehospital body cooling has been linked to improved survival rates. The benefits of therapeutic hypothermia after an OHCA were discussed by a panel of experts, including background information on the epidemiology and prognostic importance of pre-hospital factors on survival outcomes, whether all patients should be cooled after experiencing an OHCA, and issues involved in percutaneous coronary intervention during cardiopulmonary resuscitation.
- Interventional Techniques & Devices
- Myocardial Infarction
- Critical Care
- Interventional Techniques & Devices
- Myocardial Infarction
- Critical Care
- Cardiology
For people who experience an out-of-hospital cardiac arrest (OHCA), prehospital body cooling has been linked to improved survival rates. The benefits of therapeutic hypothermia after an OHCA were discussed by a panel of experts, including background information on the epidemiology and prognostic importance of prehospital factors on survival outcomes, whether all patients should be cooled after experiencing an OHCA, and issues involved in percutaneous coronary intervention (PCI) during cardiopulmonary resuscitation (CPR).
PROVIDING CONTEXT
Christian Hassager, MD, Rigshospitalet, Copenhagen, Denmark, set the context for the discussion by providing epidemiologic data and the prognostic importance of prehospital factors on outcomes in people who experience OHCA. Citing statistics from Denmark, he said that OHCAs occur in about 60 per 100 000 person-years. When looking at prehospital prognostic factors, he said significant factors related to survival included
-
male sex
-
age < 80 years
-
lack of comorbidities where the arrest is in a public place
-
presence of a bystander witness
-
bystander CPR performed
-
arrest of presumed cardiac etiology
-
a shockable primary rhythm
After multivariate adjustment, bystander witness and CPR, presumed cardiac etiology, and ventricular tachycardia (VT) and ventricular fibrillation (VF) as primary rhythm remained independent positive prognostic factors. Negative prognostic factors included increased age, longer time to emergency medical services care, and a cardiac arrest at night.
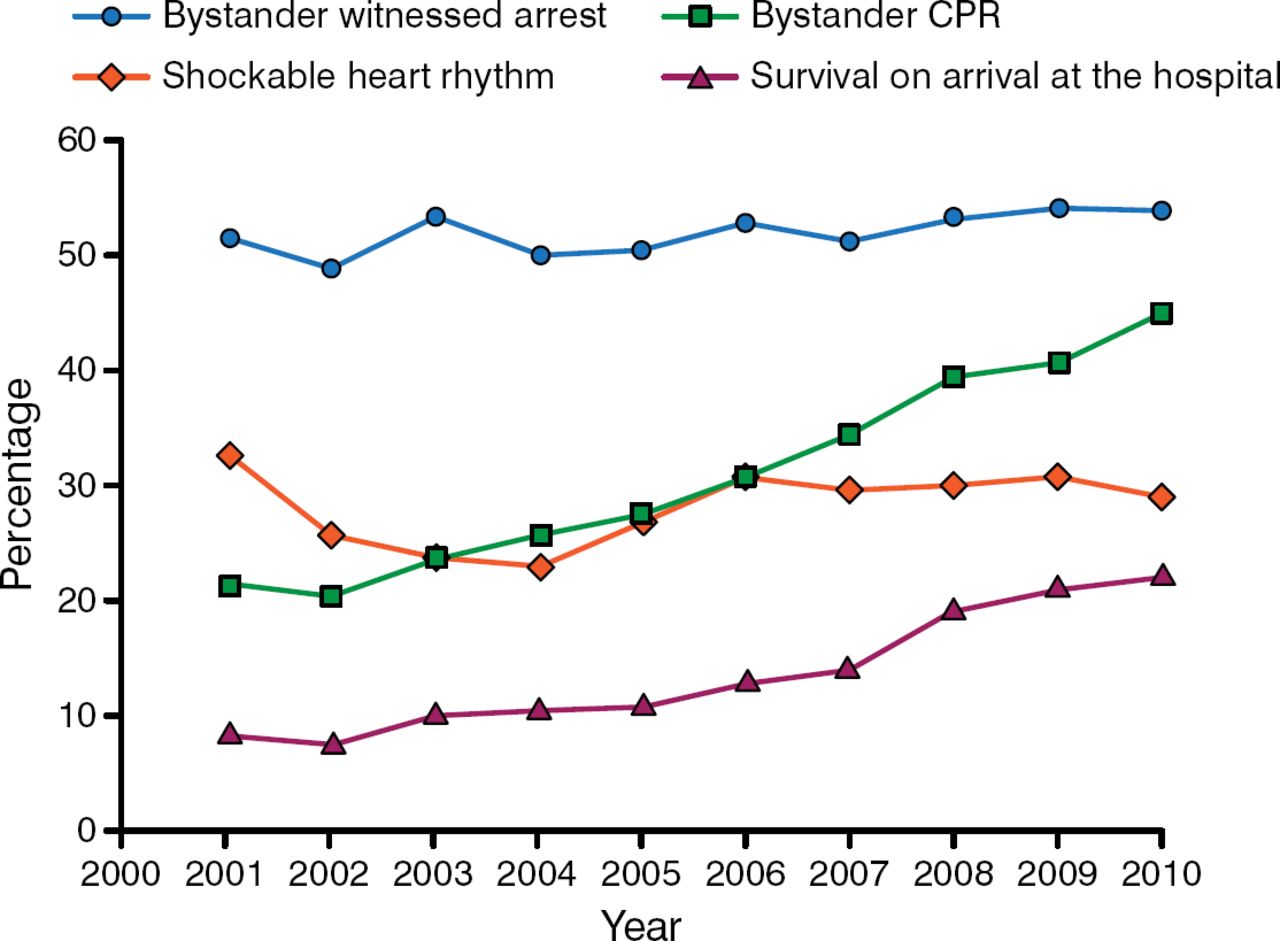
Data from a Danish cohort of nearly 20 000 patients who experienced OHCA between 2001 and 2010 showed that survival at arrival at the hospital has increased, as has the percentage of bystanders administering CPR (Figure 1) [Wissenberg M et al. JAMA. 2013].
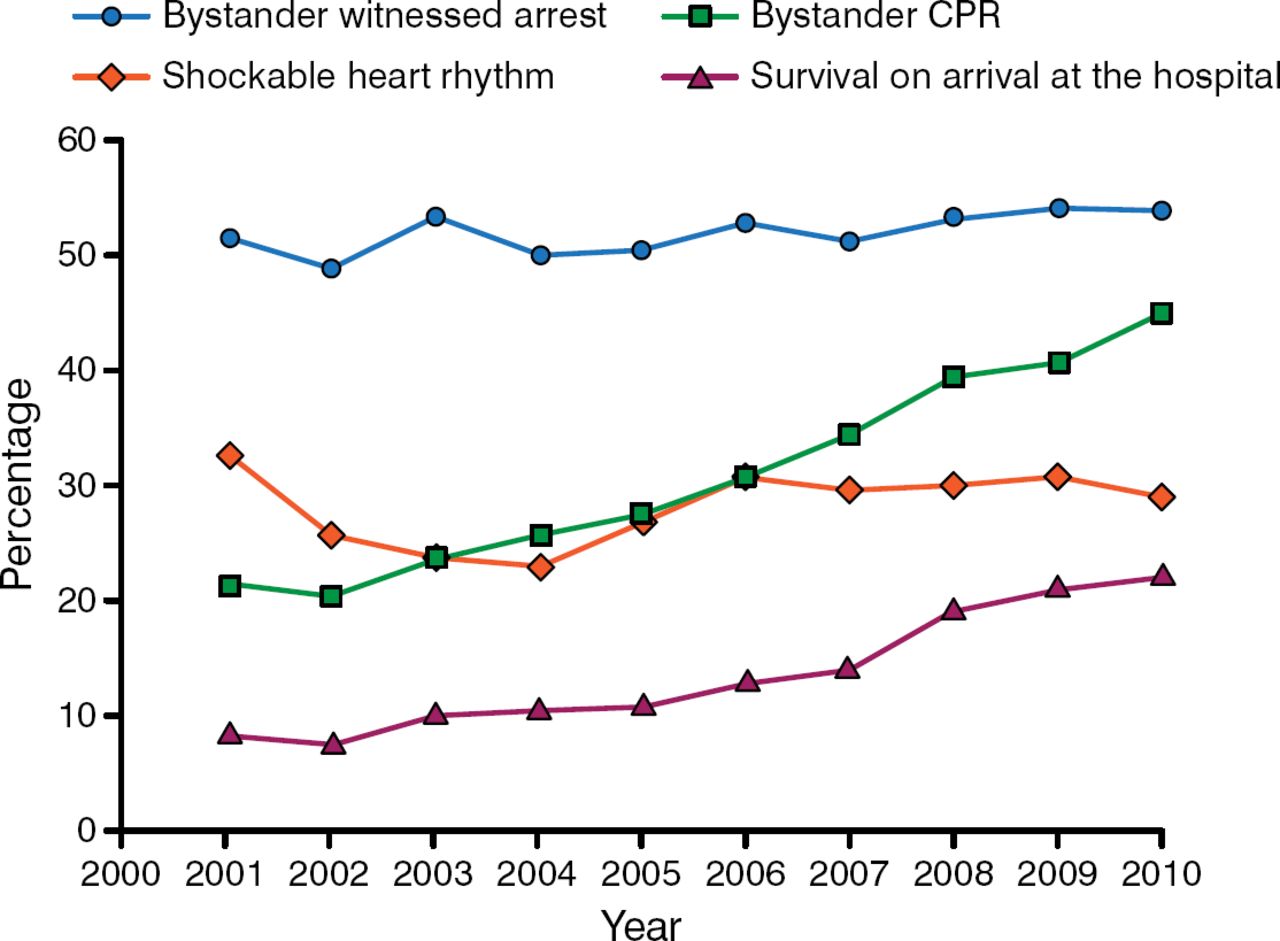
Trends Over Time in Patients With Out-of-Hospital Cardiac Arrest in Denmark
CPR, cardiopulmonary resuscitation.
Adapted from Wissenberg M et al. Association of national initiatives to improve cardiac arrest management with rates of bystander intervention and patient survival after out-of-hospital cardiac arrest. JAMA. 2013;310:1377–1384. Copyright © (2013) American Medical Association. All rights reserved.
In conclusion, Dr Hassager emphasized that bystander CPR is increasing and currently > 50% of OHCAs in Denmark have a bystander who administers CPR. Along with bystander CPR, the other most important prehospital prognostic factors include having someone witness the cardiac arrest, having VT/VF as the primary rhythm, time to EMS care, and time to return of spontaneous circulation (ROSC).
DO ALL PATIENTS BENEFIT?
Jacob E. Møller, MD, Odense University Hospital, Odense, Denmark, discussed 4 main questions regarding the benefit of therapeutic hypothermia in patients experiencing an OHCA. Namely, should all OHCAs be cooled? Which temperature should be the target temperature to cool patients in this setting to confer a survival benefit? When should cooling take place? How long should a patient be cooled?
In answering all of these questions, Prof Møller reviewed several key studies that overall showed no clear survival advantage of therapeutic hypothermia in unselected patients, which questions the current thinking on the temperature needed to benefit patients in this situation as well as when and for how long cooling should be done.
Based on the current evidence, which is largely observational, he said that there are no data to support cooling patients who, after OHCA, are in a nonshockable rhythm, those who revert to shockable rhythm, or those in cardiogenic shock [Mader TJ et al. Ther Hypothermia Temp Manag. 2014; Thomas AJ et al. Resuscitation. 2013]. Although he said that evidence does not currently support the benefit of therapeutic hypothermia for patients with a nonshockable rhythm, he also said that no data demonstrate any harm either.
In terms of goal temperature, he cited data from a recent well-designed study that showed little rationale for targeting the currently recommended 33°C to improve survival. The study evaluated all-cause mortality in 939 unconscious adults randomized to targeted temperature of either 33°C or 36°C after OHCA and found no difference between the 2 temperature cohorts (50% vs 48%; HR, 1.06; 95% CI, 0.89 to 1.28; P = .51) [Nielsen N et al. N Engl J Med. 2013]. Again, Prof Møller emphasized that although the data do not support a target temperature of 33°C, the data indicate no additional harm either.
For determining when to cool patients, there is also a lack of evidence supporting initiation of therapeutic hypothermia in the ambulance outside of the hospital [Kim F et al. JAMA. 2014; Bernard SA et al. Circulation. 2010] and recommended that cooling should not be done prior to hospitalization, though Prof Møller suggested the results may be confounded by an imbalance in baseline risk between the 2 intervention groups.
In terms of the duration of hypothermia, he noted that while 24 hours is the current recommendation, the evidence to support this duration is lacking. He emphasized that the answer to this question remains to be determined and is currently under investigation.
PCI DURING CPR
Marko Noc, MD, University Medical Center, Ljubljana, Slovenia, addressed what can be done in patients with refractory cardiac arrest needing ongoing chest compression during PCI for ROSC.
Emphasizing that PCI can be challenging or impossible if the lesion is complex and distal, Prof Noc said that a bigger issue in his experience in managing these patients is that even with an open artery, ROSC is often not established, patients often have recurrent cardiac arrest, or patients end up with profound cardiogenic shock despite successful PCI.
To better manage these patients, he proposed coupling hemodynamic support with PCI. He proposed first doing a venoarterial extracorporeal membrane oxygenation (ECMO) insertion during ongoing automated chest compression, stopping chest compression to perform a coronary angiography and PCI, and then keeping ECMO after PCI to reverse perfusion failure, inducing hypothermia and to buy time for the “stunned” myocardium.
He highlighted the importance of early induction of ECMO by citing a European study of 51 patients with refractory cardiac arrest in whom automated chest compression was started out of the hospital and followed by ECMO implantation upon hospital arrival at a median delay from collapse to ECMO of 120 minutes [Le Guen M et al. Critical Care. 2011]. Of the 51 patients, only 2 (4%) survived and were in good neurologic condition at 28 days, arguing for an aggressive central neurologic system protective strategy with therapeutic hypothermia.
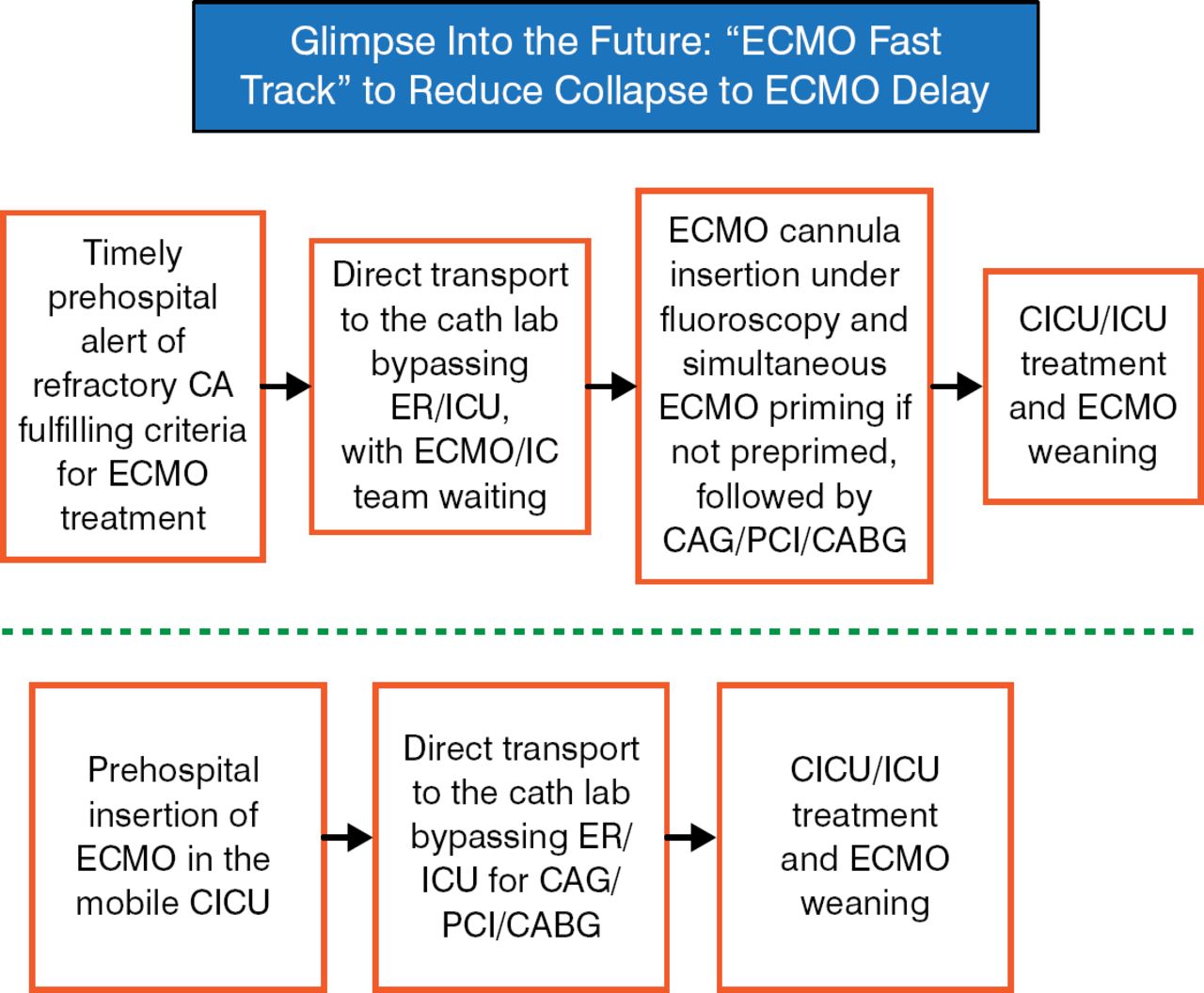
Prof Noc shared a schema that may provide a method of more effectively managing patients with refractory cardiac arrest based on early use of ECMO (Figure 2).
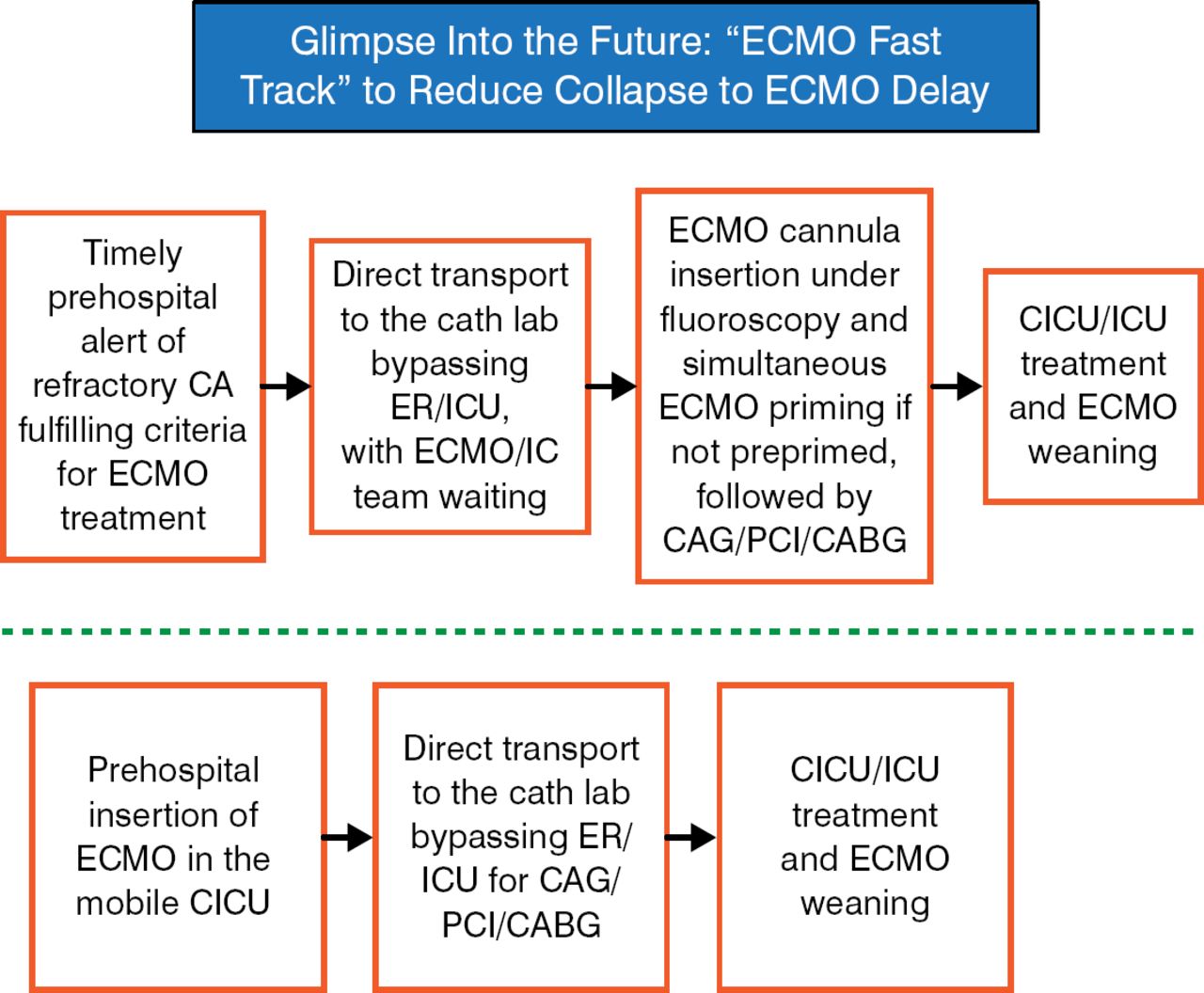
Future Schema on Treating Patients With Refractory Cardiac Arrest
CA, cardiac arrest; CABG, coronary artery bypass grafting; CAG, coronary angiography; cath lab, catheter laboratory; CICU, cardiac intensive care unit; ECMO, extracorporeal membrane oxygenation; ER, emergency room; IC, intensive care; ICU, intensive care unit; PCI, percutaneous coronary intervention.
Reproduced with permission from M Noc, MD.
Finally, Prof Noc emphasized the need for developing adequate multidisciplinary prehospital and in hospital systems to better support the critical need to not delay the time between cardiac arrest and performing ECMO and PCI.
In conclusion, many important questions and exciting developments continue to evolve in the area OHCA, prognostic risk stratification, therapeutic hypothermia, and other interventions to improve patient outcomes.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.