

Summary
Ankle fractures are common injuries that result in pain, swelling, and, often, the need to take narcotic pain medication. The prospective randomized Aspiration for Pain Relief Following Ankle Fracture trial [NCT01484535], as discussed in this article, was conducted to assess the impact of aspiration of ankle fracture hemarthrosis on pain relief and need for pain medication.
- Foot & Ankle Conditions
- Orthopaedic Pain Management
- Orthopaedics Clinical Trials
- Orthopaedics
- Foot & Ankle Conditions
- Orthopaedic Pain Management
- Orthopaedics Clinical Trials
Although aspiration of fracture hemarthrosis has been shown to decrease pain when used for fractures of the radial head and femoral neck, Stephen A. Sems, MD, Mayo Clinic, Rochester, Minnesota, USA, presented data demonstrating that aspiration for acute ankle fractures does not result in decreased patient-reported pain scores or opioid use.
Ankle fractures are common injuries that result in pain, swelling, and, often, the need to take narcotic pain medication. The prospective randomized Aspiration for Pain Relief Following Ankle Fracture trial [NCT01484535] was conducted to assess the impact of aspiration of ankle fracture hemarthrosis on pain relief and need for pain medication.
In this double-blind, placebo-controlled trial, patients with AO-Müller/OTA fracture classification 44 and fractures presenting within 24 hours of injury were eligible to participate, provided they were skeletally mature and able to provide consent. Patients with other injuries, including soft tissue wounds that precluded aspiration, were excluded. Ankle aspiration was accomplished through either the anterolateral or anteromedial portal and was continued until no more fluid could be removed. Control was achieved through a sham aspiration procedure in which a needle was advanced to the level of the subcutaneous tissue, held in place for a count of 10, and then removed; that is, no fluid was removed.
The primary outcome was pain (measured via a self-reported Numeric Rating Scale Pain Scale based on a score of 0 to 10) and narcotic use (self-recorded in a custom diary, then converted to oral morphine equivalents [OMEs]) for the first 72 hours). Secondary outcomes included limb volume (as measured by fluid displacement), 6-month Olerud-Molander Ankle Score, Short Musculoskeletal Function Assessment (SMFA), and complications.
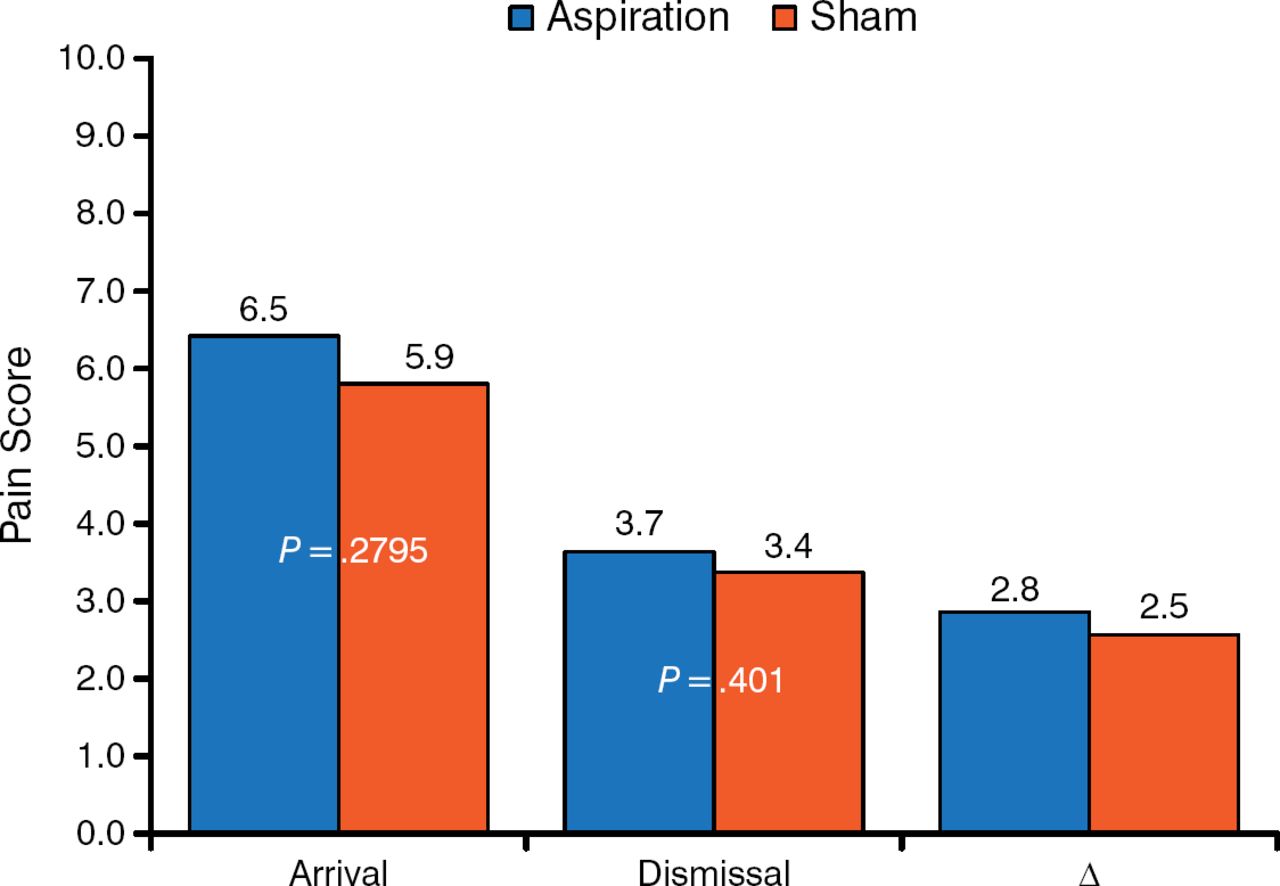
Patients were enrolled October 2011 to January 2014 and included 124 patients (61 randomized to aspiration; 63 to control). Participants had a mean age of 52 years and were mostly women (79 of 124). Similar proportions of patients went on to surgical treatment (72.1% of the aspiration group; 69.8% of controls). Pain scores on arrival in the emergency department (ED) and at discharge were the same for both groups, as was the change in pain score (Figure 1). Patient-reported pain scores over the next 96 hours were also evaluated and were found to be similar at all time points.

Pain Scores in the Emergency Department
Reproduced with permission from SA Sems, MD.
Patients were discharged from the ED with a prescription for pain medication and asked to record their medication use over the next 96 hours. The total amount of pain medication used was similar (89 OMEs for the aspiration group; 103 OMEs for controls; P = .43). No differences were seen in secondary outcomes—including limb volume, 6-month SMFA score, and Olerud-Molander Ankle Score—or complications. Complications were rare (2 infections in the aspiration group) and not significantly different between the 2 groups (P = .5).
Strengths of this study include its design and size. Weaknesses include the fact that many otherwise eligible patients (n = 108) declined enrollment, which may indicate a selection bias, and the fact that pain scores were self-reported.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.