

Summary
Hypoglycemia can be a serious condition caused by a variety of mechanisms, such as unintentional administration of antidiabetic agents, tumors, medications, and gastric bypass surgery. The management of hypoglycemia depends on its cause. This article discusses factitious and felonious hypoglycemia, diagnostic procedures for organic hypoglycemia syndromes, as well as the the causes and management of post-gastric bypass hypoglycemia.
- Hyperglycemia/Hypoglycemia
- Endocrinology
- Diabetes & Metabolic Syndrome
- Hyperglycemia/Hypoglycemia
Hypoglycemia can be a serious condition caused by a variety of mechanisms, such as unintentional administration of antidiabetic agents, tumors, medications, and gastric bypass surgery. The management of hypoglycemia depends on its cause.
Vincent Marks, MD, University of Surrey, Guildford, Surrey, United Kingdom, spoke about factitious and felonious hypoglycemia. Classical factitious hypoglycemia results from self-administered insulin, insulin analogs, insulin secretagogues, or sulfonylureas. Accidental insulin administration resulting in hypoglycemia occurs mainly in hospitals and is an important cause of medicolegal litigation. Felonious hypoglycemia results from administration of these agents by another, usually with criminal intent, and is less common than accidental administration. In almost all cases, clinical history will be unreliable. Therefore, laboratory data upon which the diagnosis is made must be reliable, and appropriate samples need to be obtained.
Current insulin immunoassays are not sufficiently specific and should not be used for forensic cases. Some commercial tests are not able to detect certain insulin analogs now in use, and kits vary in the minimal detectable level of insulin analogs [Owen WE, Roberts WL. Clin Chem. 2004]. Prof Marks recommends liquid chromatography-mass spectrometry assays for insulin and its analogs in forensic cases.
Prof Marks discussed several cases illustrating these points. In one, the husband of an insulin-dependent diabetic woman aged 75 years with dementia, who was paralyzed from multiple sclerosis, was suspected of administering an insulin overdose. The immunoreactive insulin level in postmortem peripheral venous blood was 3 times the expected level. However, the patient had been treated with porcine insulin, and the assay was calibrated for human insulin. A reassay with porcine standards yielded a normal insulin level, resulting in a finding of death by natural causes.
In another case of suspected murder by insulin injection, a nurse left her obese, paraplegic, but active husband at home while she attended a party and spent the night with a friend. The next morning, she could not contact him by telephone, and she had someone go to the house, where her husband, who had complained of feeling ill the evening before, was comatose. He had vomited and had a full catheter bag, which the wife, upon returning home, emptied. She was suspected to have given him a large dose of insulin before she left; however, he had called someone hours after that. His blood glucose at hospitalization was 0.7 mmol/L, and his insulin level was 887 pmol/L. Yet, the unreliability of insulin assays was not fully appreciated, and later samples were not obtained before his death. The administration of glucose had not reversed his hypoglycemia. Reasons to doubt an insulin overdose in this case include vomiting (rare in insulin-induced hypoglycemia), polyuria, and a rapid fall in plasma albumin that was greater than that observed in patients attempting suicide via insulin overdose. His plasma potassium concentration was > 4 mmol/L, which is rare in insulin-induced hypoglycemic coma. In the end, hypoglycemia can be the first sign of sepsis [Alamgir S et al. Am J Med. 2006], and this was believed to have caused the death of the nurse's husband, Prof Marks concluded.
In any case of hypoglycemia, a blood sample (peripheral venous—not central or cardiac for postmortem samples) should be taken for analysis as soon as possible and before glucose is administered. Capillary (finger stick) samples cannot be used in forensic investigation. In hospital practice, for any case of severe hypoglycemia for which the cause is not immediately apparent, blood must be collected as soon as possible and daily for at least a week. Plasma should be stored for analysis until a satisfactory explanation for the hypoglycemia is determined.
Michael Nauck, MD, Diabeteszentrum, Bad Lauterberg im Harz, Germany, discussed diagnostic procedures for organic hypoglycemia syndromes and reviewed publications. Tumors can result in hypoglycemia by producing insulin (insulinoma) or, more rarely, insulin-like growth factor (IGF) 1 or 2. Although the presence of insulinoma can be predicted by an amended insulin:glucose ratio after a prolonged, supervised fast [Nauck M et al. Ann Intern Med. 2012], there may be some false positives and negatives. Prof Nauck's unpublished review of the literature suggests that the preoperative procedure most sensitive for diagnosis is the glucagon-like peptide 1 (GLP-1) scintigram. One of its drawbacks is that malignant tumors do not always express GLP-1, although benign ones do [Christ E et al. J Clin Endocrinol Metab. 2009]. Surgical procedures are more sensitive for diagnosing insulinoma. Characteristics of hypoglycemia mediated by IGF-2 compared with IGF-1 are summarized in Table 1.
Differential Diagnosis of Tumor-Associated Hypoglycemia
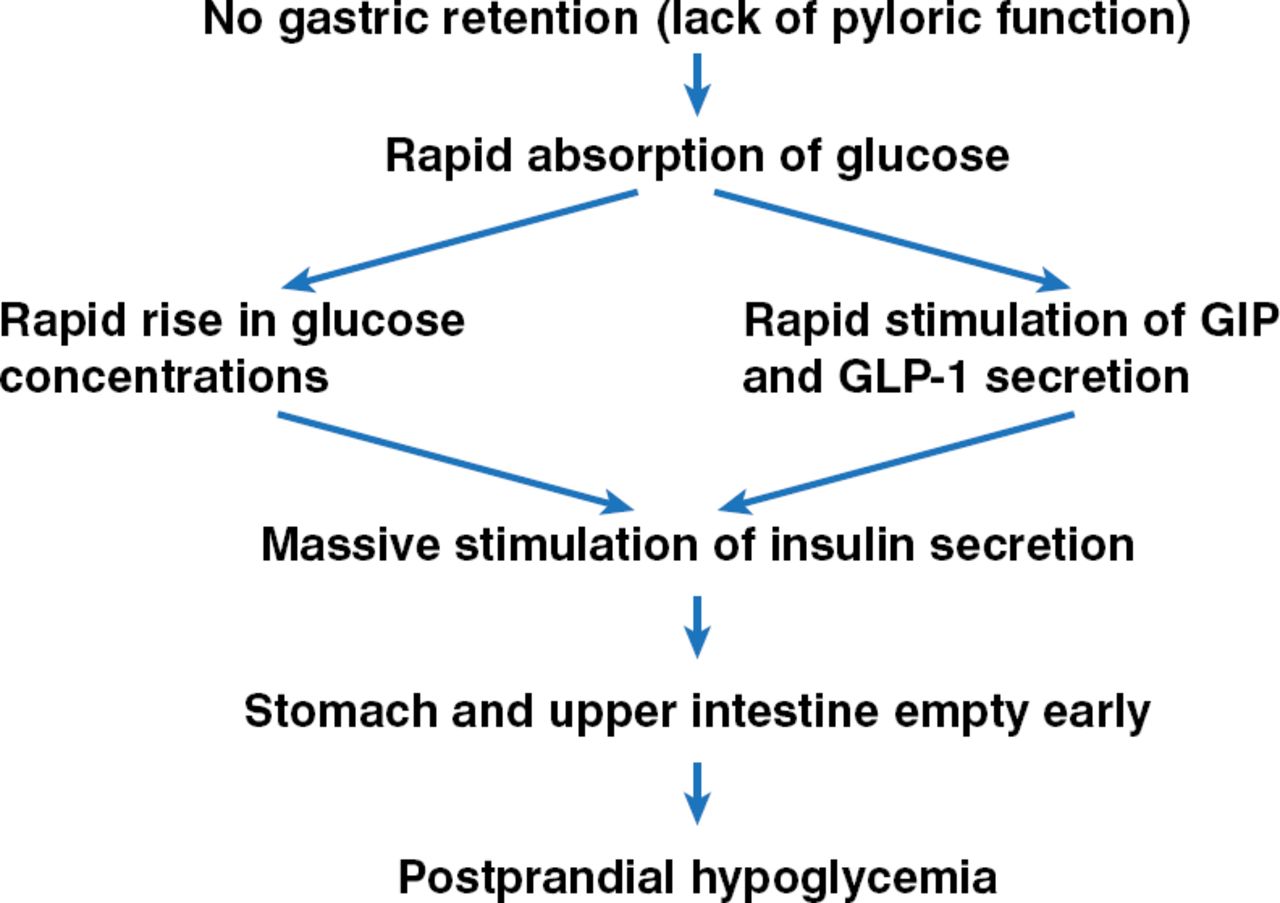
Reactive hypoglycemia includes late dumping syndrome observed after gastric resections—the pathophysiology of which is illustrated in Figure 1.

Pathophysiology of Late Dumping Syndrome After Gastric Surgery
GIP, gastric inhibitory peptide; GLP-1, glucagon-like peptide 1.
Reproduced with permission from M Nauck, MD.
Idiopathic reactive hypoglycemia (IRH) involves impaired counterregulatory responses, accelerated gastric emptying, and altered (increased) hypoglycemia awareness. Mean plasma glucose and insulin levels after an oral glucose load reach a higher initial peak, then drop lower for patients with IRH and for controls than they do after a meal test. Therefore, the oral glucose load is an artificial test and should not be used for diagnosis of IRH.
Clinicians should keep in mind that many medications are associated with hypoglycemia besides antidiabetic drugs, such as anti-infective drugs and cardiac medications [Murad MH et al. J Clin Endocrinol Metab. 2009].
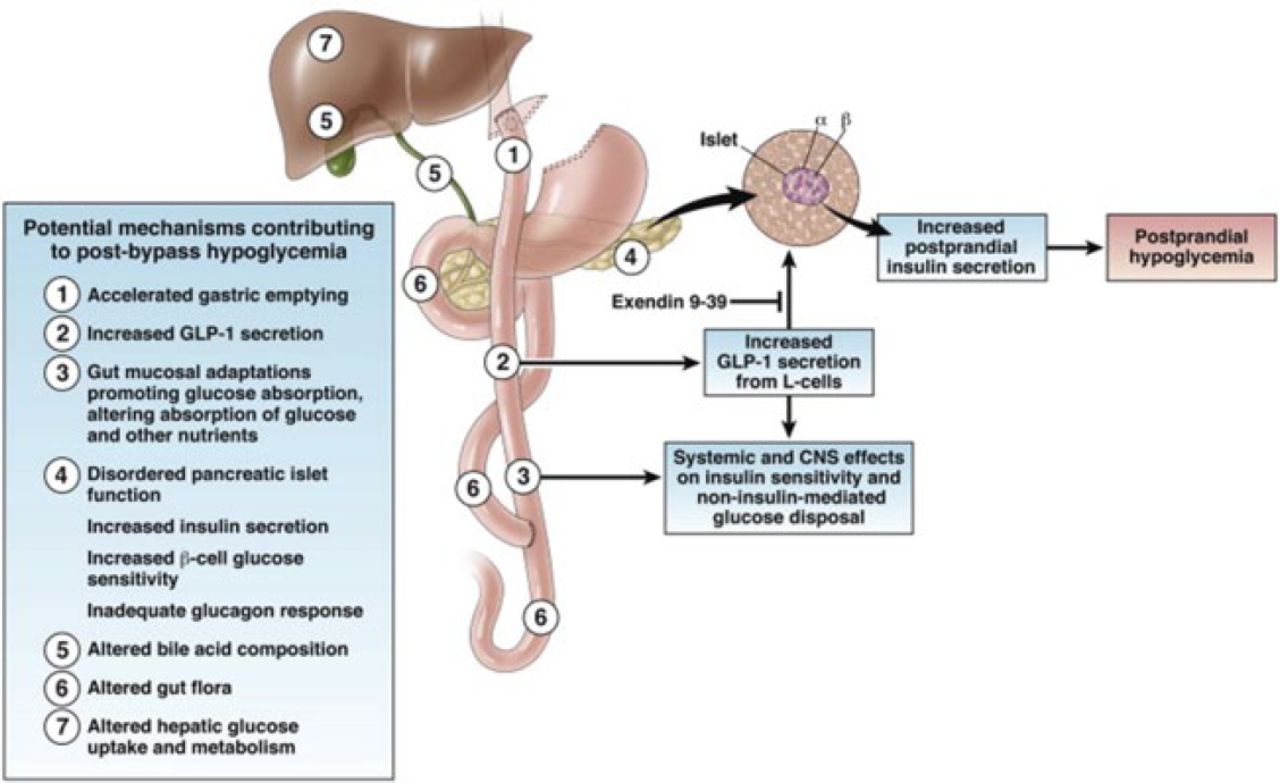
Helene Hanaire, MD, PhD, University of Toulouse III, Toulouse, France, reviewed the causes and management of post-gastric bypass hypoglycemia. Gastric bypass surgery can induce long-term remission of type 2 diabetes but can also induce abnormal glycemic patterns in previously unaffected patients. Prof Hanaire believes that clinicians should focus on symptomatic and severe hypoglycemia. A summary of the causes of severe and symptomatic hypoglycemia associated with gastric bypass is shown in Figure 2.

Causes of Severe and Symptomatic Hypoglycemia After Gastric Bypass
CNS, central nervous system; GLP-1, glucagon-like peptide 1.
Reprinted from Gastroenterology, 146, Patti M et al, Hypoglycemia After Gastric Bypass: The Dark Side of GLP-1, 605–608, Copyright 2014, with permission from AGA Institute.
Treatment of severe and symptomatic hypoglycemia associated with gastric bypass involves dietary modifications: dividing food into multiple meals, avoiding high glycemic index carbohydrates, limiting carbohydrates to 30 g per meal, observing a 30-minute break between food and fluid intake, increasing the viscosity of food items with pectin or guar gum, and avoiding stress. Although some medications have been tried when dietary modifications fail, evidence is anecdotal, involving only a few patients. Larger studies examining safety and efficacy are needed for medications as well as surgical intervention.
The treatment of hypoglycemia depends on its cause and therefore requires prompt and accurate diagnosis.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.