

Summary
Accurate clinical staging of patients with non—small cell lung cancer (NSCLC) is essential to optimize treatment and outcomes. This article discusses current perspectives on the surgical treatment of lung cancer, including the revised European Society of Thoracic Surgeons guidelines for preoperative mediastinal lymph node staging for NSCLC. Also discussed are how improvements in imaging and the use of computed tomography imaging for diagnostic workup and screening have led to many small lung cancers being found.
- Tomography
- Cancer
- Radiography
- Respiratory Cancers
- Tomography
- Cancer
- Radiography
- Respiratory Cancers
- Oncology
Accurate clinical staging of patients with non-small cell lung cancer (NSCLC) is essential to optimize treatment and outcomes. Paul De Leyn, MD, PhD, University Hospitals Leuven, Belgium, launched a series of presentations that covered current perspectives on the surgical treatment of lung cancer, including the revised European Society of Thoracic Surgeons (ESTS) guidelines for preoperative mediastinal lymph node (MLN) staging for NSCLC.
Lung cancer staging is a critical step in patients with potentially resectable NSCLC in terms of both correct prognosis and therapy, and it comprises an important part of patient care. In the absence of distant metastases, mediastinal involvement is the most important prognostic factor. Ruling out MLN involvement enables consideration of the patient for surgery. Pathological staging remains the gold standard to quantify the extent of locoregional and MLN involvement.
With this in mind, in 2007, the ESTS published clinical practice guidelines on preoperative mediastinal staging to aid treatment decision making, integrating imaging, endoscopic, and surgical techniques. New data with important implications for mediastinal staging techniques have been available since 2007, however, including the new lymph node (LN) map of the lungs and mediastinum released by the International Association for the Study of Lung Cancer (IASLC) in 2009. In addition, new information on restaging and techniques for mediastinal restaging has emerged. Consequently, a revision of the 2007 ESTS guidelines was initiated [De Leyn P et al. Eur J Cardiothorac Surg 2014].
The updated ESTS guidelines recommend routine biopsy of at least the right and left lower paratracheal LNs (stations 4R and 4L) and the subcarinal LNs (station 7) as minimal requirements for MLN staging, with biopsy of the right and left upper paratracheal stations (2R and 2L) if present. Biopsy of the LN stations below the azygos vein (10R) and below the upper rim of the left pulmonary artery (10L) can be performed if indicated.
Invasive preoperative mediastinal staging is advised for tumors larger than 3 cm (especially in cases of adenocarcinoma with a high standardized uptake value), central tumors or N1 nodes, and restaging. It is not required, however, in cases of peripheral T1a-b category disease.
In cases of computed tomography (CT)-enlarged or positron emission tomography (PET)-positive MLNs, confirmation of disease in the tissue is indicated. When possible, endosonography (endobronchial ultrasonography or esophageal ultrasonography) with fine-needle aspiration is the technique of choice because it is minimally invasive and has high sensitivity. If the tissue is negative, surgical staging is necessary, and the revised guidelines advise that a combination of endoscopic staging and surgical staging results in the highest accuracy. Consequently, optimal MLN staging involves a multidisciplinary team approach, and the staging technique chosen will depend on availability and expertise to meet the minimal requirements for staging.
The lung cancer field is therefore undergoing many changes, and Hisao Asamura, MD, National Cancer Center Hospital, Tokyo, Japan, discussed how improvements in imaging and the use of CT imaging for diagnostic workup and screening have led to many small lung cancers being found. This has inevitably changed the management and surgical approach to lung cancer. Although the traditional standard of care for early-stage lung cancer is a lung lobectomy, its appropriateness for early-stage disease is now being questioned, and less radical treatments such as limited resection are currently being explored.
In the immediate future, data from ongoing studies will help to address some questions on outcomes in sublobar resection in early-stage lung cancer. Two clinical trials are currently underway in Japan, conducted by the Japan Clinical Oncology Group (JCOG) and West Japan Oncology Group (WJOG).
A Phase 3 randomized clinical trial (JCOG0802/WJOG4607L) is ongoing to compare surgical treatments for relatively early disease. The aim of this study is to evaluate the noninferiority in overall survival (OS) of limited resection compared with lobectomy in patients with small-sized (≤2 cm) peripheral NSCLC with a ground-glass opacity portion of less than 25%, excluding radiologically determined noninvasive cancer. The primary endpoint is OS, and secondary endpoints include postoperative respiratory function and proportion of patients who successfully undergo limited resection. As of March 2014, 995 of a target 1,100 patients have been enrolled [Nakamura K et al. Jpn J Clin Oncol 2014].
A Phase 2 trial (JCOG0804/WJOG4507L) also aims to investigate the feasibility of wedge resection for peripheral early disease (≤2 cm) with a ground-glass opacity portion of more than 75%. This trial is still recruiting participants, and the target sample size is 330 patients.
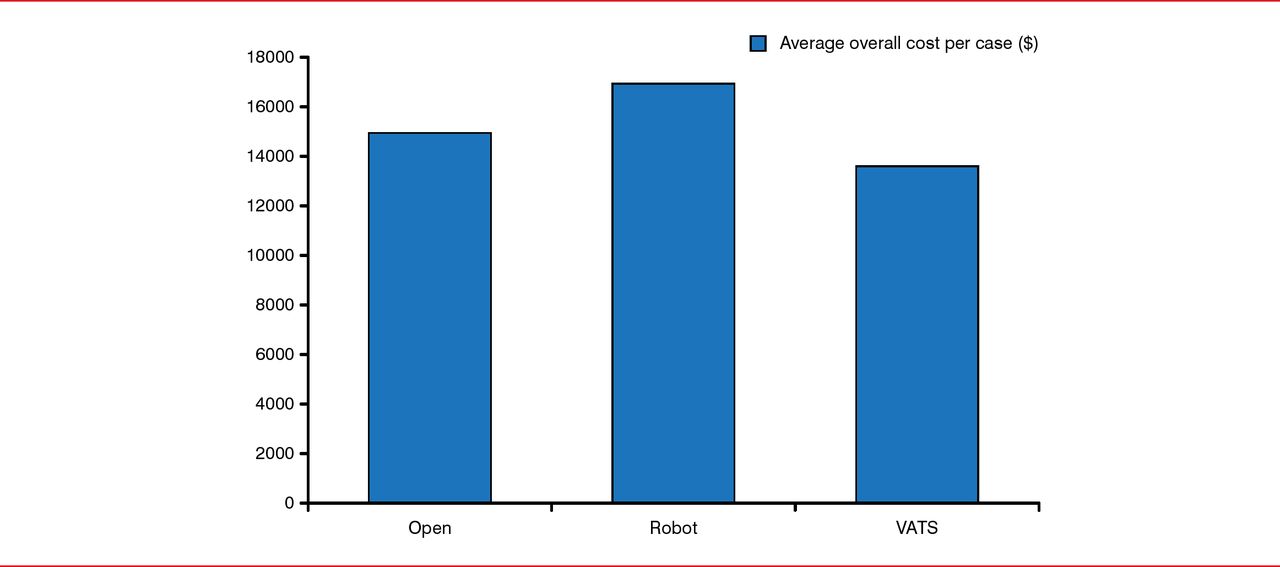
Overall, the 3 surgical platforms are appropriate options for lung resection, although the robotic technique currently appears to be the most costly, whereas video-assisted thoracoscopic surgery seems to be the least expensive approach (Figure 1) [Deen SA et al. Ann Thorac Surg 2014]. According to experts, however, open thoracotomy is still a good treatment option in select cases. Dr. Asamura advised against compromising on an optimal cancer surgery, emphasizing that a technological approach should be chosen only if it represents the optimum surgical technique.

Cost Comparison of Surgical Approaches to Lung Resection
VATS=video-assisted thoracoscopic surgery.
Overall cost per case comparison: open versus robot (p=0.058), open versus video-assisted thoracoscopic (VATS; p = 0.227*), and robot versus VATS (p<0.001).
Reproduced from Deen SA et al. Defining the cost of care for lobectomy and segmentectomy: a comparison of open, video-assisted thoracoscopic, and robotic approaches. Ann Thorac Surg 2014;97(3):1000–1007. With permission from Elsevier.
*On December 1, 2014, this was changed from 0.2271 to 0.227.
Thoracic surgery, therefore, remains a major diagnostic and therapeutic modality for patients with NSCLC, although many controversial issues remain regarding its precise role and application. Dr. Asamura concluded that more definitive recommendations on the surgical treatment choice can be made only when the results of large randomized studies such as the JCOG trials become available.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.