

Summary
This article summarizes Caribbean Heart Care Medcorp, St. Clair, Trinidad and Tobago 4-year experiences with the surgical treatment of adult ventricular septal defects (VSDs).
- Myocardial Infarction
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
- Myocardial Infarction
- Interventional Techniques & Devices
- Cardiology Clinical Trials
Giovanni Teodori, MD, Caribbean Heart Care Medcorp, St. Clair, Trinidad and Tobago, summarized the institution's 4-year experience with the surgical treatment of adult ventricular septal defects (VSDs).
Adult VSDs can be congenital or can arise following a myocardial infarction (MI). The tissue surrounding defects is usually strong in congenital cases but is markedly fragile in post-acute MI VSDs. Treatment differs as well. Congenital adult VSD involves patching or direct suturing following access through the aortic valve or right atrium, whereas post-acute MI VSD access is treated using single stitches to suture a patch or gluing of a double patch following mainly through the infarct, right atrium, and tricuspid annulus. Treatment of congenital VSD carries the risk for atrioventricular block. Post-acute MI VSD surgery carries the risk for bleeding, and treatment can fail.
From January 2010 to February 2014, 9 patients with adult VSDs were treated at Caribbean Heart Care Medcorp. Of these, 5 cases were congenital (perimembranous) and 4 were post-MI VSDs (3 were acute and 1 was chronic, following a surgical procedure conducted in 2006). Eight cases were diagnosed by preoperative echocardiography, while the remaining case was incidentally diagnosed during intraoperative echocardiography.
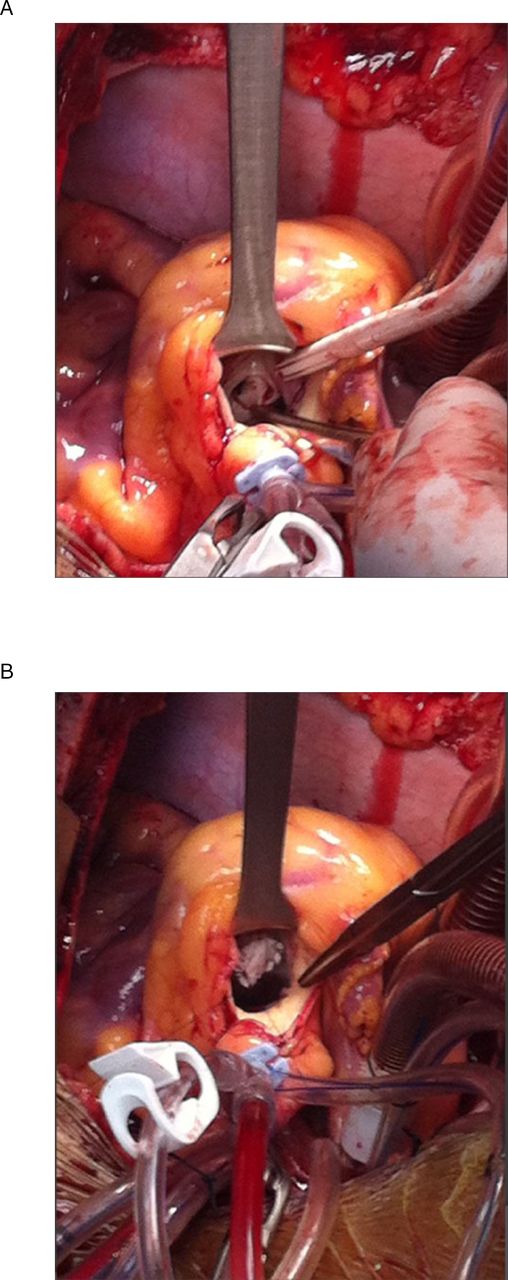
The 5 congenital cases involved patients aged 22 to 56 years (mean age, 37.5 years). Four cases were treated using a GORE-TEX™ (W. L. Gore and Associates, Newark, Delaware) patch with pledgetted single stitches, with the remaining case treated by direct suture. One case is presented in Figure 1.
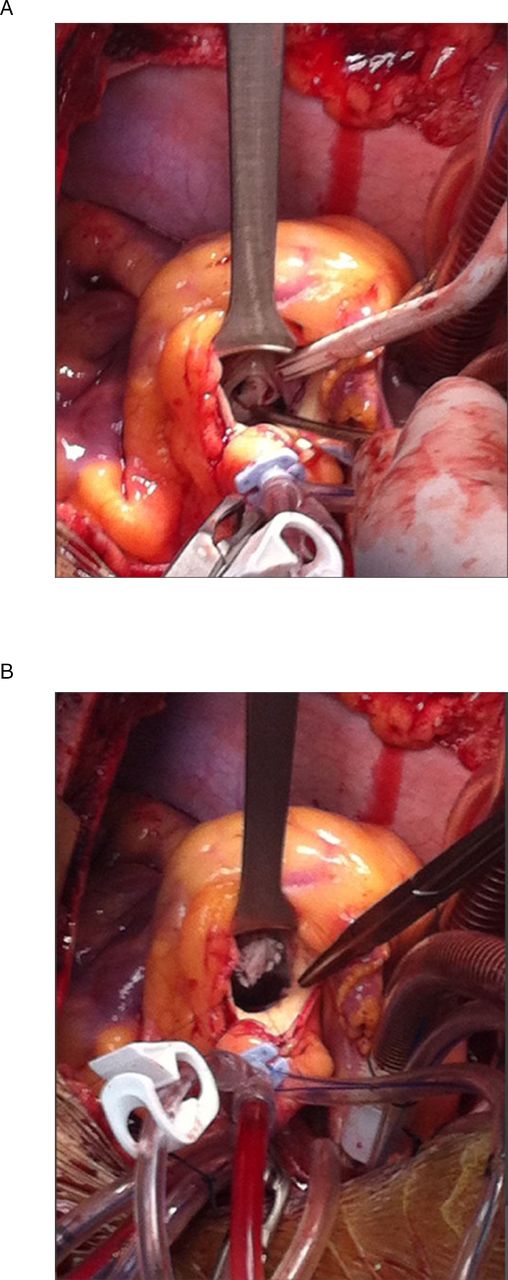
Case of Perimembranous Ventricular Septal Defect Prior to Repair (a) and Following Repair (b)
Reproduced with permission from G Teodori, MD.
Reproduced with permission from G Teodori, MD.
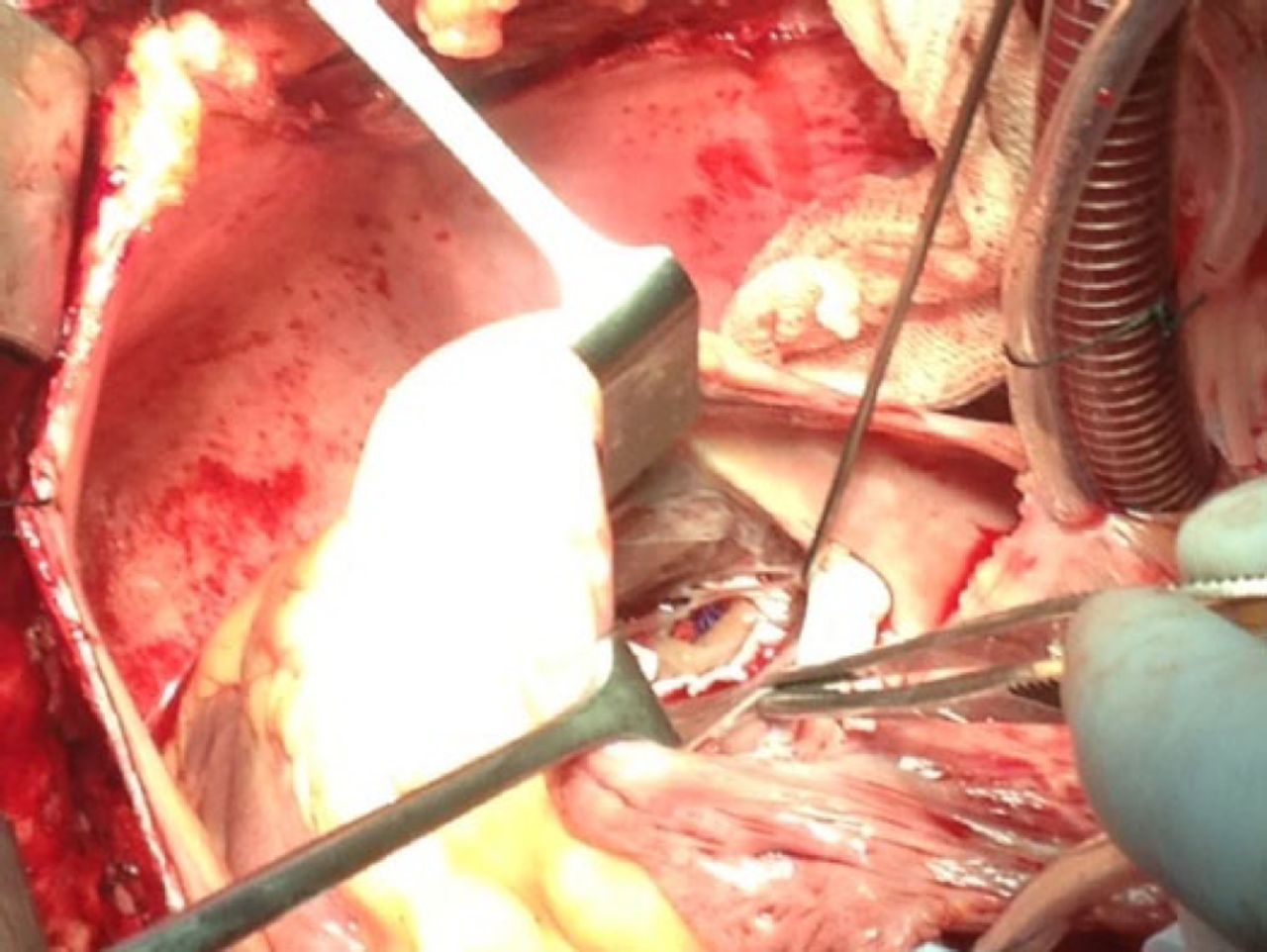
The 4 cases of postinfarct VSD involved patients aged 45 to 68 years (mean age, 61 years). The time from diagnosis to surgery was 3 days in 2 patients and 9 days in another patient, with the remaining patient presenting with chronic VSD. Preoperative clinical condition was the use of an intra-aortic balloon pump (n = 2) and New York Heart Association (NYHA) functional classes III (n=1) and IV (n = 1). Surgical access was through the area of infarct (n = 3) or the tricuspid annulus (n = 1) (Figure 2). Surgery involved a single patch (n = 2), a double patch with the use of glue (n = 1), and the reinforcement of a prior repair (n = 1).
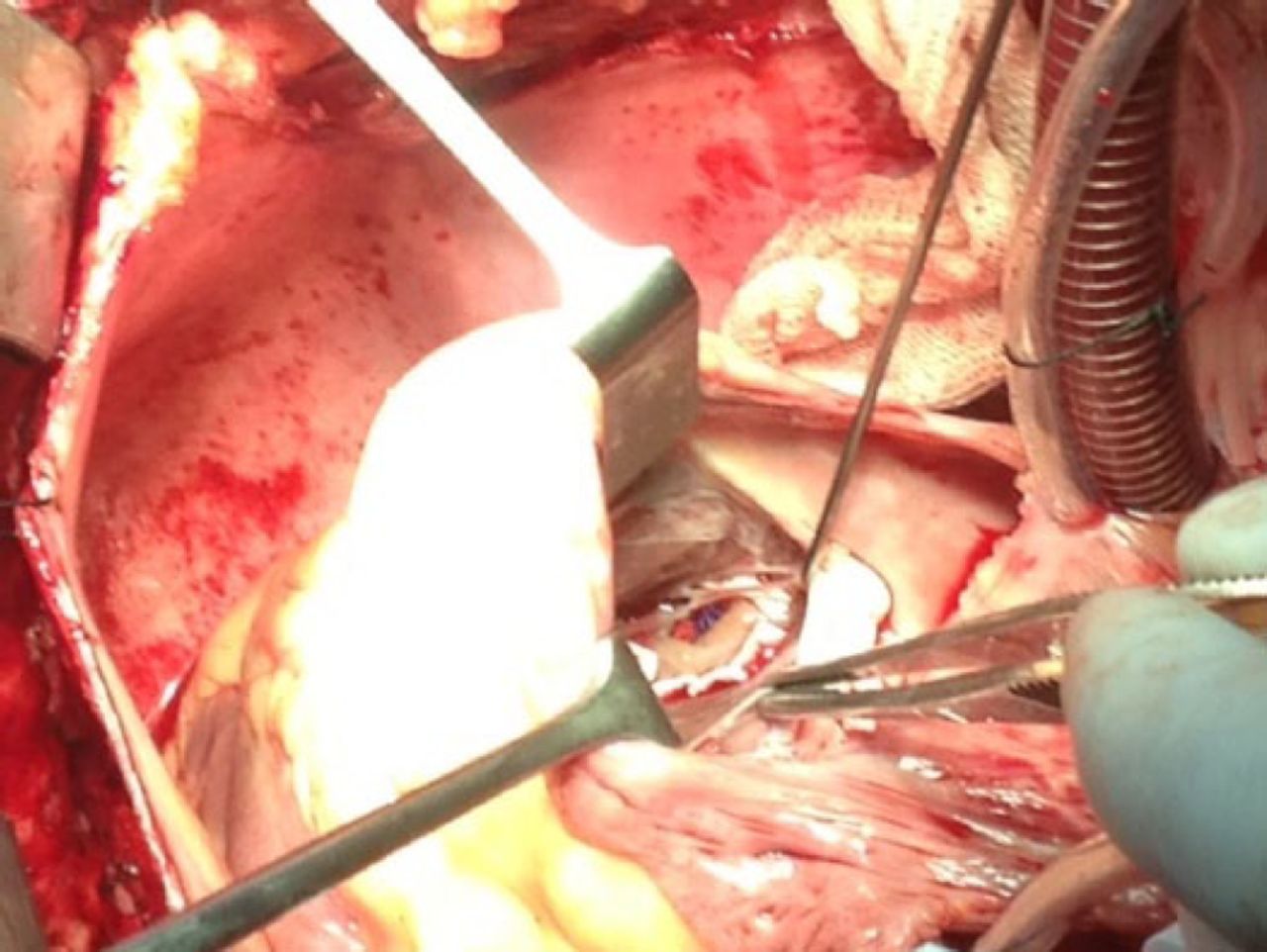
Transtricuspid Repair of a Post-Myocardial Infarction Ventricular Septal Defect
Reproduced with permission from G Teodori, MD.
All the patients were discharged with no residual VSDs, which was maintained at 6 months. One patient died 8 months following surgery because of bowel infarction, with the remaining 8 alive and assessed as NYHA classes I and II.
Although limited by the small number of cases and anatomic variations from patient to patient, the variation in VSD type encountered in the study indicates challenges in terms of the surgical technique used and the operative risks.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.