

Summary
There have been significant advances in the management of atrial fibrillation (AF), the most common irregular heart rhythm. In a special session, data were presented from a series of surveys conducted to enhance the understanding of clinical practice patterns in the management and treatment of AF in the member countries of the European Society of Cardiology (ESC) and the results' concordance with ESC guidelines.
- Interventional Techniques & Devices
- Cardiology
- Arrhythmias
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Arrhythmias
There have been significant advances in the management of atrial fibrillation (AF), the most common irregular heart rhythm. In a special session, data were presented from a series of surveys conducted to enhance the understanding of clinical practice patterns in the management and treatment of AF in the member countries of the European Society of Cardiology (ESC) and the results' concordance with ESC guidelines.
ASSESSMENT OF STROKE AND BLEEDING RISK IN PATIENTS WITH AF
Torben Bjerregaard Larsen, MD, Aalborg University Hospital, Aalborg, Denmark, shared the results of the recent European Heart Rhythm Association (EHRA) survey regarding the assessment of the risk of stroke and bleeding in patients with AF in clinical practice, particularly the use of risk evaluation schemes [Larsen TB et al. Europace 2014]. A response to the survey was received from 47 centers, of which 74.5% were university hospitals and 17% were private hospitals.
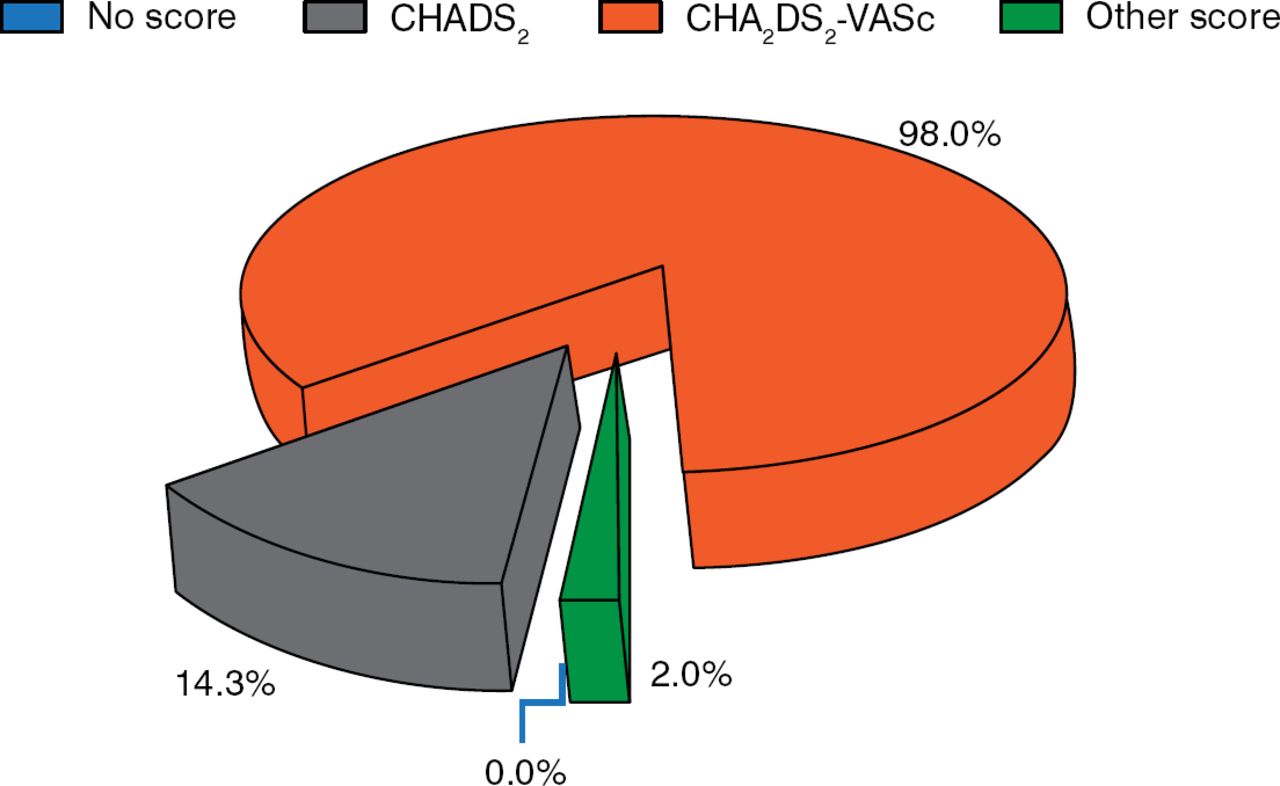
All centers routinely estimated stroke risk in their patients, with 98% using the CHA2DS2-VASc score, as recommended by ESC guidelines (Figure 1). This risk stratification model has been shown to reliably identify patients at low risk for thromboembolism. While the CHADS2 scoring system incorporates the risk factors of congestive heart failure, hypertension, age >75 years, diabetes mellitus, and previous stroke or transient ischemic attack, the CHA2DS2-VASc score incorporates the additional risk factors of age 65 to 74 years, presence of vascular disease, and female sex.
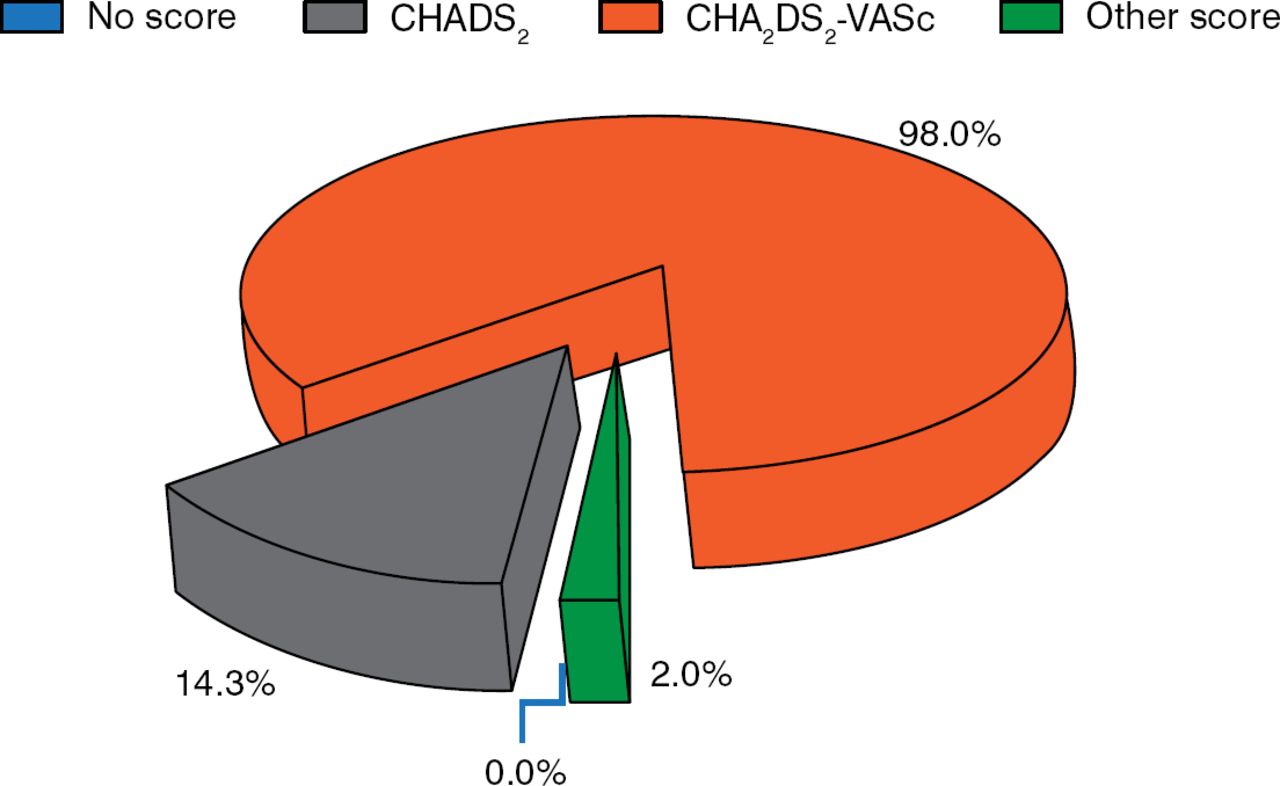
Routine Use of Stroke Risk Scores in Clinical Practice
Reproduced from Larsen TB et al. Stroke and bleeding risk evaluation in atrial fibrillation: results of the European Heart Rhythm Association survey. Europace 2014;16:698–702. With permission from the European Society of Cardiology.
Nearly 80% of centers routinely estimated bleeding risk using the HAS-BLED score, while the remainder said that they would use any score. The HAS-BLED score incorporates numerous bleeding risk factors, including uncontrolled systolic blood pressure >160 mm Hg, abnormal renal or liver function, previous stroke, prior bleeding history or predisposition, labile international normalized ratios, being elderly, and concomitant drugs or excess intake of alcohol. Interestingly, 82.6% of centers indicated that the HAS-BLED score did not affect their decision to initiate or continue anticoagulant therapy, and 70.8% did not take creatinine clearance values into account when initiating oral anticoagulation (OAC) therapy. However, due to the increasing use of novel OAC agents, more attention should be paid to renal function, Prof. Larsen concluded.
ANTIARRHYTHMIC DRUGS AND CARDIOVERSION
Laurent Pison, MD, PhD, Maastricht University Medical Center, Maastricht, The Netherlands, noted that the ESC guidelines recommend rhythm control in patients with symptomatic AF (EHRA score ≥2) despite adequate rate control. The guidelines also state that while rhythm control is acceptable for controlling symptoms in patients, antithrombotic therapy for underlying heart disease should also continue [Camm AJ et al. Eur Heart J 2012; Camm AJ et al. Eur Heart J 2010]. The survey revealed that rhythm control is more widely applied in clinical practice than expected, with ≥70% of responding centers applying this strategy to patients with significant AF-related symptoms despite rate control [Dagres N et al. Europace 2013; Hernández-Madrid A et al. Europace 2013]. Electrical cardioversion seems to be the preferred mode of rhythm control compared with pharmacologic cardioversion (68% vs 19% of respondents).
β-blockers are not typically recommended by the ESC guidelines for long-term antiarrhythmic drug therapy, as they are only moderately effective in preventing recurrent AF with the exception of exercise-induced or thyrotoxicosis-associated cases. Nevertheless, the survey revealed that β-blockers are frequently used in clinical practice in the context of hypertension and left ventricular (LV) hypertrophy for 43% of centers, coronary artery disease and normal LV ejection fraction for 51%, stable heart failure (HF; New York Heart Association [NYHA] I and II) for 51%, and advanced HF (NYHAIII and IV) for 38%. In contrast, very few centers (11%) use dronedarone for long-term antiarrhythmic drug therapy.
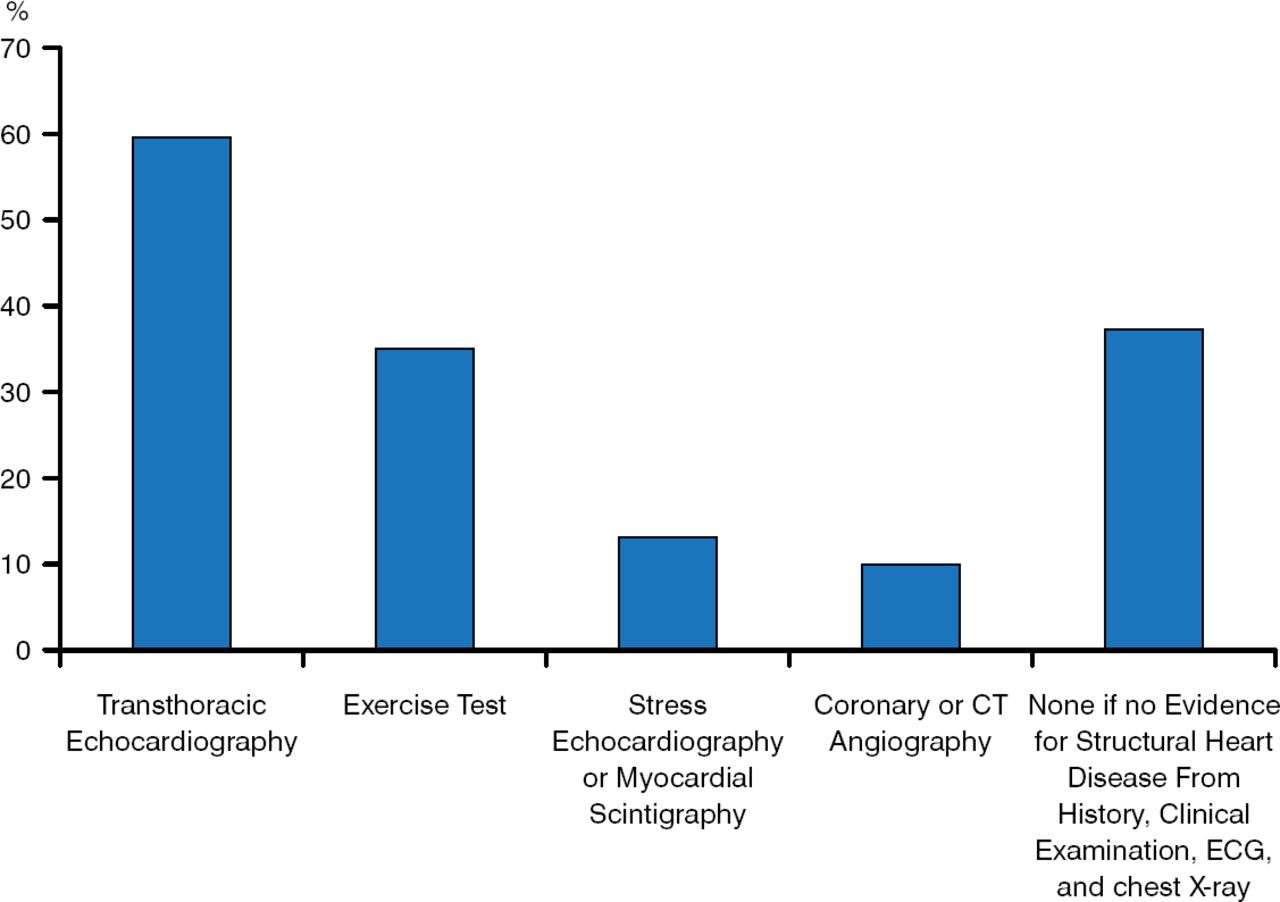
While ∼60% of the responding centers use transthoracic echocardiography as part of the diagnostic workup before prescribing class 1c anti-arrhythmic drugs, interestingly, ∼40% of centers did not perform any diagnostic procedure unless there was clinical evidence of structural heart disease by history, exam, electrocardiogram, or radiograph (Figure 2).
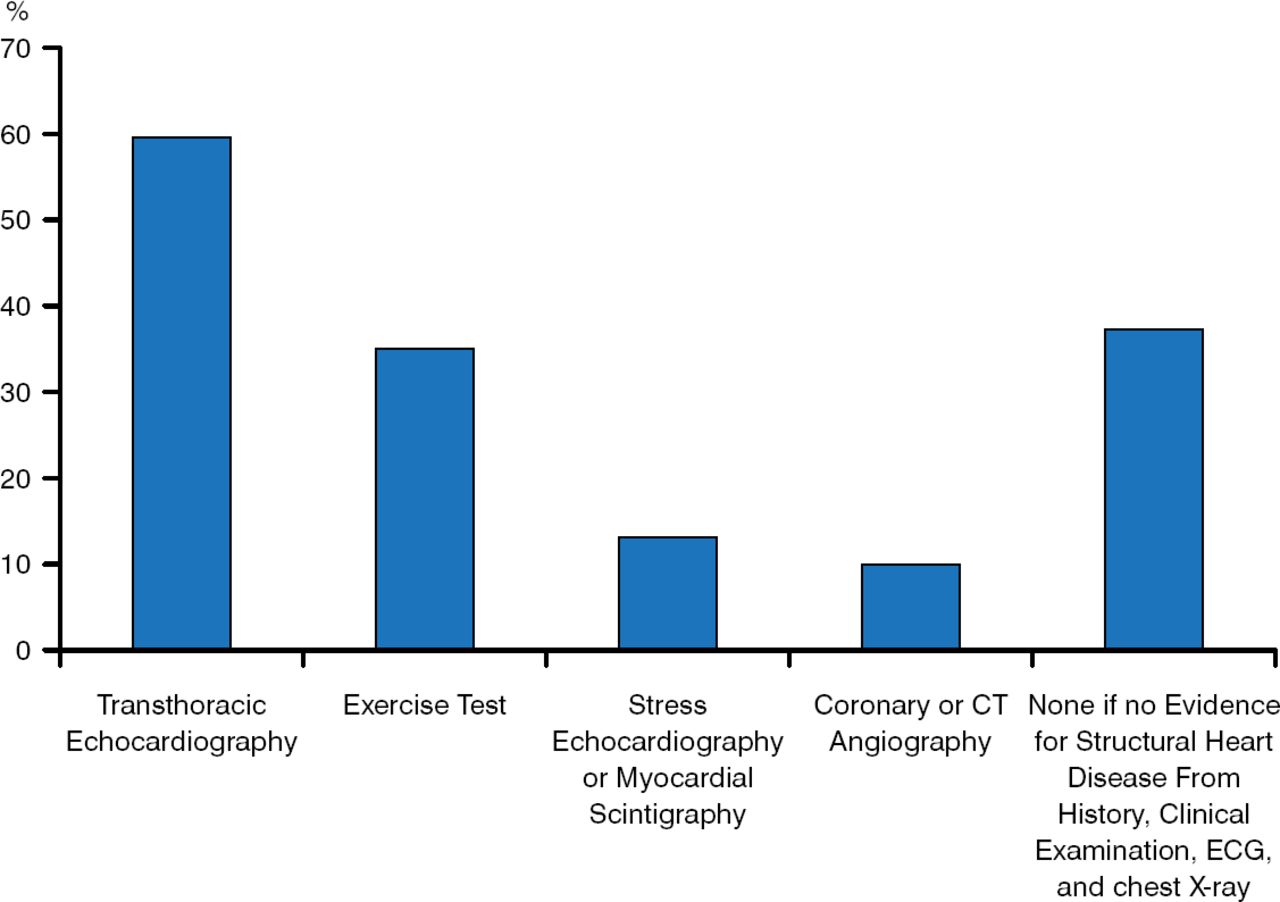
Type of Diagnostic Workup Performed Before Prescribing Class 1c Drugs
CT=computed tomography; ECG=electrocardiography.
Reproduced from Dagres N et al. Current practice of antiarrhythmic drug therapy for prevention of atrial fibrillation in Europe: the European Heart Rhythm Association survey. Europace 2013;15:478–481. With permission from the European Society of Cardiology.
CATHETER ABLATION STRATEGY AND PERIPROCEDURAL MANAGEMENT OF PATIENTS
Prof. Pison reported that according to the results from several surveys [Chen J et al. Europace 2014; Pison L et al. Europace 2013; Lip GY et al. Europace 2012; Pison L et al. Europace 2012], most European centers are following the guideline recommendations with regard to catheter ablation strategy and periprocedural management of AF [Calkins H et al. Heart Rhythm 2012; Camm AJ et al. Eur Heart J 2012; Camm AJ et al. Eur Heart J 2010]. However, he highlighted some interesting survey findings.
Current guidelines recommend that anticoagulation therapy be continued after ablation in patients who are at high risk of stroke based on the CHADS2 or CHA2DS2VASC scores. However, some centers reported that OAC therapy was discontinued after successful ablation, even in patients with a CHA2DS2VASC score ≥2 (6% of centers at 3 to 6 months; 10% at 6 to 12 months) or a CHADS2 score ≥2 (8% of centers at 3 to 6 months; 6% at 6 to 12 months).
Differences in catheter ablation management of AF were also reported. Ablation for AF was performed more frequently as first-line therapy in patients who had not failed an antiarrhythmic drug in high-volume centers (200 to 399 procedures/year) compared with extremely high-volume centers (>400 procedures/year) or medium-volume centers (100–199 procedures/year; 39.1% vs 30.0% vs 18.8%, respectively).
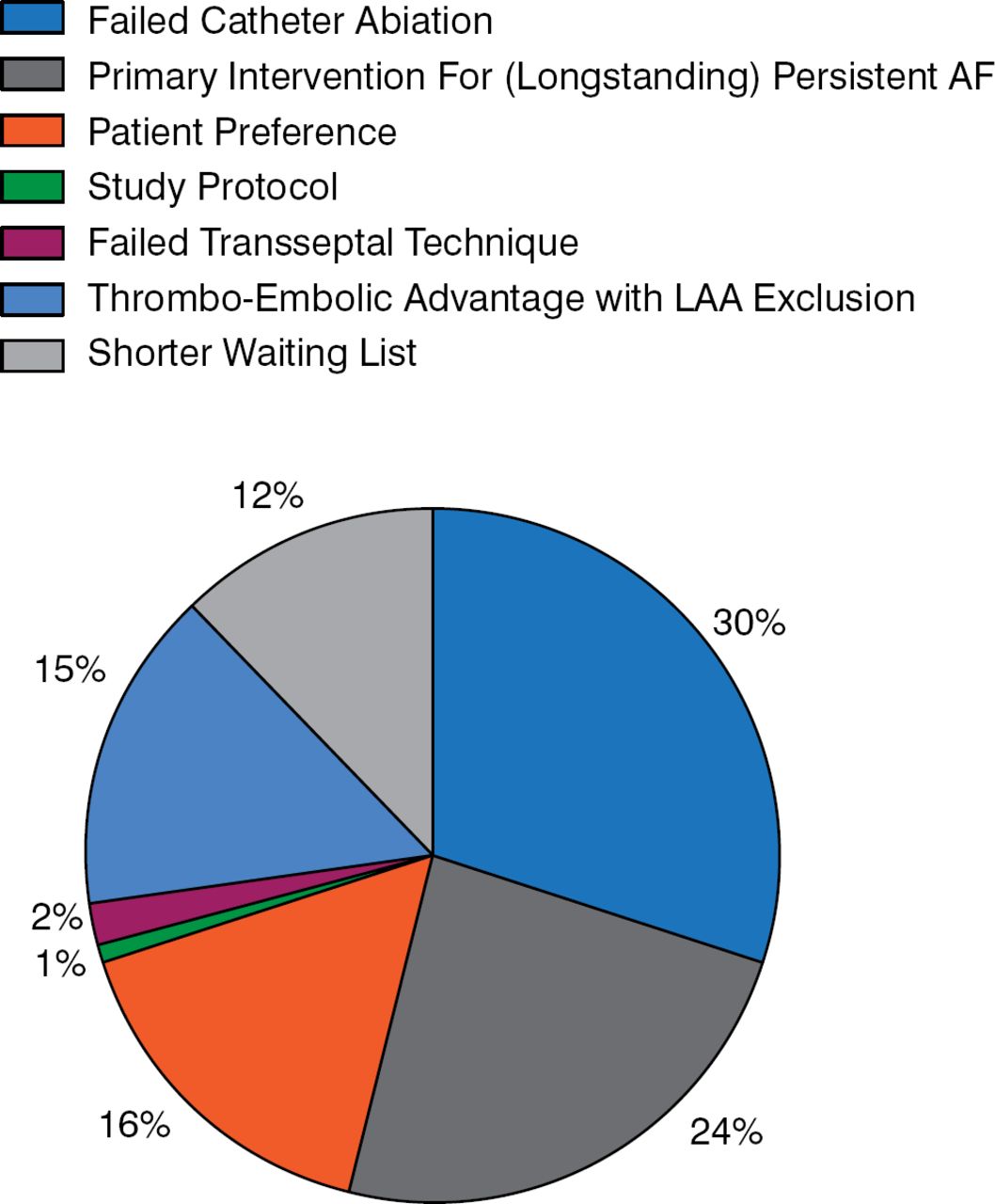
Prof. Pison also noted that surgical and hybrid ablation for AF was performed in a minority of centers. Surgical ablation as a stand-alone procedure was used by only 46% of responding centers. The most common indications for surgical or hybrid ablation were a failed catheter ablation (30%) and as a primary intervention for long-standing persistent AF (24%; Figure 3).
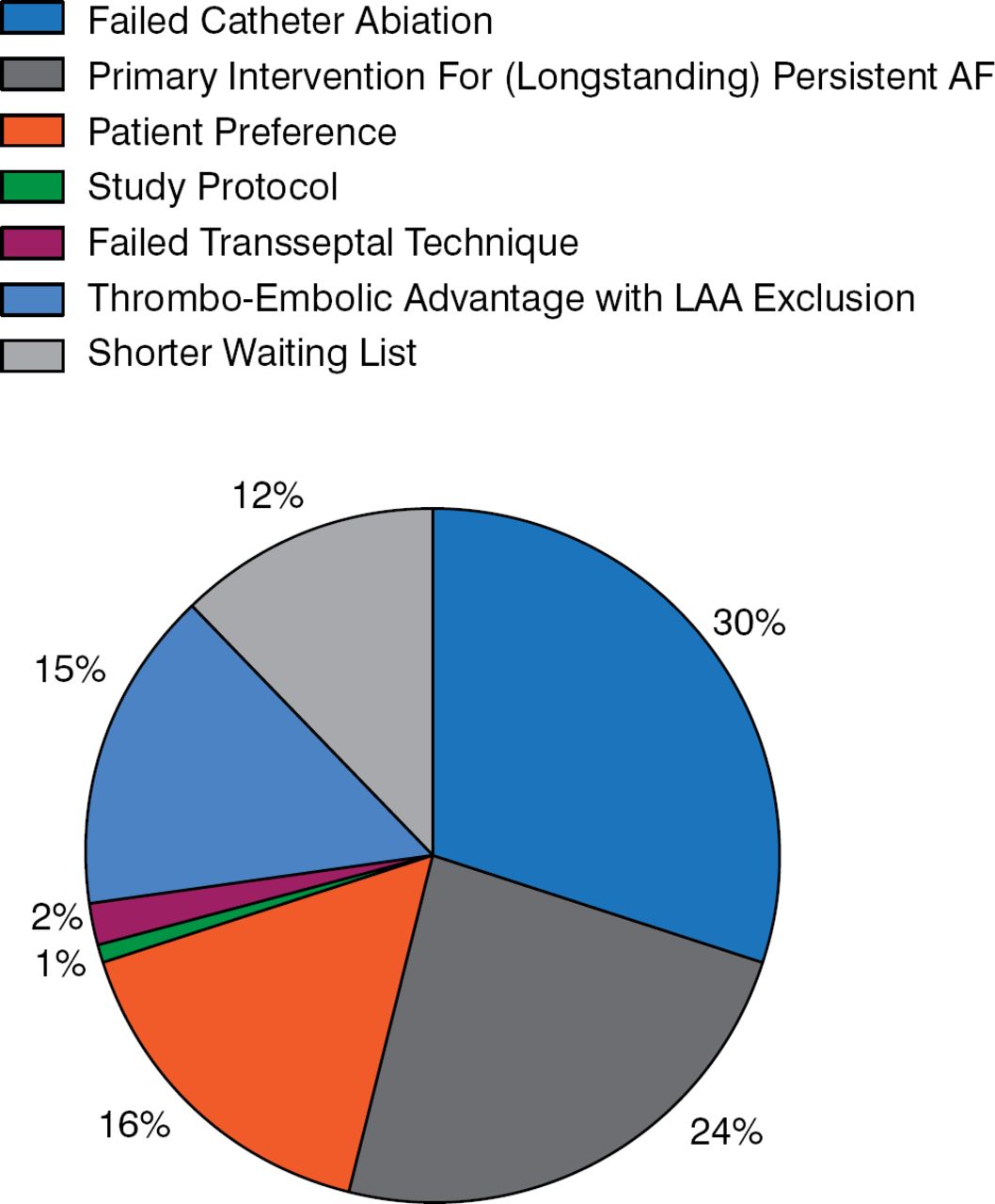
Survey: Indications Reported for Performing Surgical and Hybrid Ablation for Atrial Fibrillation
AF=atrial fibrillation; LAA=left atrial appendage.
Reproduced from Pison L et al. Surgical and hybrid atrial fibrillation ablation procedures. Europace. 2012;14:939–941. With permission from the European Society of Cardiology.
CARDIAC RESYNCHRONIZATION THERAPY
The European Cardiac Resynchronization Therapy Survey I [CRT Survey I] was conducted to describe the use of cardiac resynchronization therapy (CRT) implantation in clinical practice [Dickstein K et al. Eur Heart J 2009]. Data were collected from 141 centers in 13 European countries, with a total of 2438 patients who were successfully implanted with a CRT device, with or without an implantable cardioverter-defibrillator (ICD). Thirty-one percent of patients were aged ≥75 years, 23% had AF, and 19% had a QRS duration <130 milliseconds. Twenty-six percent of patients with a CRT had a prior pacemaker or ICD. Seventy-three percent of patients received a CRT-with-defibrillation device. The remaining patients who received CRT-with-pacing devices were mostly older. The patients in the CRT Survey I shared similarities with patients in randomized clinical trials of CRT. Notable differences include more elderly patients and more patients with AF, device upgrade, or a narrow QRS.
Cecilia Linde, MD, PhD, Karolinska University Hospital, Stockholm, Sweden, said that the objective of the planned CRT Survey II is to assess current clinical practice, capture essential logistical and procedural details, evaluate safety measures, and assess health care resource utilization. The survey will also provide information for hospitals and others to benchmark their practice against national and international practice. The CRT Survey II will collect data similar to those in the first survey but will also focus on the diagnostic workup for CRT implantation.
The CRT Survey II will be conducted by the EHRA and the Heart Failure Association of the ESC during the first 6 months of 2015. The goal is to include 20,000 patients from 45 member countries of the ESC and to report the results in September 2015.
SUMMARY
Overall, current practice in management and treatment of AF in the member countries of the ESC is in line with the ESC guidelines.

The editors would like to thank the many members of the Cardiostim EHRA Europace 2014 presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.