

Summary
This article disuccses medical conditions and devices addressed in the most recent European Heart Rhythm Association (EHRA) scientific documents, which typically deal with novel areas that lack a sufficient evidence base to support firm guidelines. The aim of these documents is to provide sound advice from experts, based on the available scientific data, for emerging areas in the management of arrhythmias in Europe.
- Interventional Techniques & Devices
- Heart Failure
- Arrhythmias
- Cardiology
- Myocardial Infarction
- Interventional Techniques & Devices
- Heart Failure
- Arrhythmias
- Cardiology & Cardiovascular Medicine
- Myocardial Infarction
In a session about medical conditions and devices addressed in the most recent European Heart Rhythm Association (EHRA) scientific documents, Michael Glikson, MD, Sheba Medical Center, Tel Hashomer, Israel, explained that these documents typically deal with novel areas that lack a sufficient evidence base to support firm guidelines. The aim of these documents is to provide sound advice from experts, based on the available scientific data, for emerging areas in the management of arrhythmias in Europe.
LEFT ATRIAL APPENDAGE OCCLUSION DEVICES
In patients with nonvalvular atrial fibrillation (NVAF), embolic stroke is considered to be associated with left atrial appendage (LAA) thrombosis. Prof. Glikson highlighted some of the evidence supporting the EHRA/European Association of Percutaneous Cardiovascular Interventions position statement on the use of LAA occlusion devices.
Although 4 LAA occlusion devices are used in Europe, Prof. Glikson emphasized that only the Watchman device is currently being considered for approval by the US Food and Drug Administration and that it is the device with the most scientific evidence.
The Watchman Left Atrial Appendage System for Embolic Protection in Patients With Atrial Fibrillation trial [PROTECT AF; NCT00129545] was the first randomized controlled trial (RCT) to show that the Watchman device was noninferior to warfarin for stroke thromboembolic protection in patients with NVAF (mean CHADS2 score, 1.8). At 1065 patient-years of follow-up, the primary composite end point of stroke, cardiovascular death, and systemic embolism was 3.0 per 100 patient-years (95% credible interval [CrI], 1.9 to 4.5) in the device group and 4.9 per 100 patient-years (95% CrI, 2.8 to 7.1) in the control group (rate ratio [RR], 0.62; 95% CrI, 0.35 to 1.25) [Holmes DR et al. Lancet 2009]. However, primary safety events related to excessive bleeding were more frequent in the device group (7.4 per 100 patient-years; 95% CrI, 5.5 to 9.7) than in the control group (4.4 per 100 patient-years; 95% CrI, 2.5 to 6.7), with a RR of 1.69 (95% CrI, 1.01 to 3.19).
The prospective randomized Evaluation of the Watchman LAA Closure Device in Patients With Atrial Fibrillation Versus Long Term Warfarin Therapy trial [PREVAIL; NCT01182441] was conducted subsequently to further assess the efficacy of the Watchman device and to address some of the related safety concerns. Patients with NVAF who were at risk of stroke were randomly assigned 2:1 to receive either the device or warfarin therapy. The CHADS2 score was used to assess stroke risk. The trial met its safety end point, showing that the device can be safely implanted by new operators. Early safety events occurred in 2.2% of the device group, significantly lower than in PROTECT AF, satisfying the safety performance goal. The rate of adverse effects was lower in PREVAIL than in PROTECT AF (4.2% vs 8.7%; p=0.004), based on a broader, more inclusive definition of adverse effects [Holmes DR Jr et al. J Am Coll Cardiol 2014]. These results add to the extensive amount of published data confirming the safety profile of the Watchman device as an option for the reduction of stroke in patients at high risk of bleeding on anticoagulants, Prof. Glikson stated.
NEW DEVICES IN HEART FAILURE
Andreas Metzner, MD, Hanseatic Heart Centre, Hamburg, Germany, discussed the current EHRA report on new devices for the treatment of heart failure (HF), in which special attention was given to patients with New York Heart Association class III and IV HF and a narrow QRS complex, who compose a larger group in HF compared with those with a wide QRS complex [Kuck KH et al. Europace 2014].
Various innovative therapeutic and monitoring devices are now in use or under evaluation for the treatment of HF, including cardiac contractility modulation (CCM), cervical vagal stimulation, intracardiac atrioventricular nodal vagal stimulation, spinal cord stimulation, carotid sinus nerve stimulation, and implantable hemodynamic monitoring devices. However, evidence based on RCT data is lacking, with only some data present for CCM. Clinical trials are underway to investigate the benefits and potential complications for the other devices.
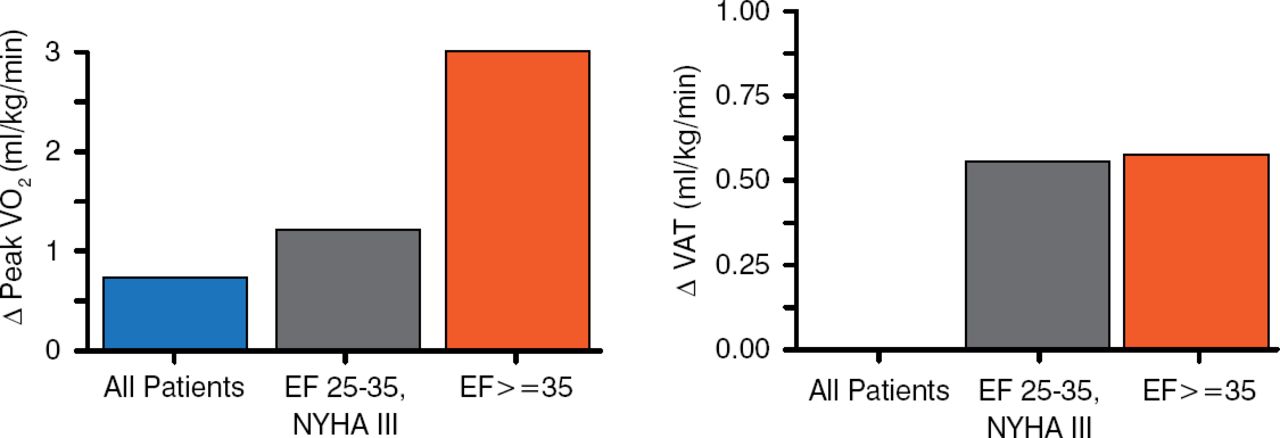
Prof. Metzner presented data from FIX-CHF-5, a prospective parallel-group RCT that evaluated the safety and efficacy of CCM at 12 months in 428 patients with New York Heart Association class III to IV HF, an ejection fraction <35%, and narrow QRS. Participants were randomly assigned to CCM or no CCM therapy on top of optimal medical therapy. There was a significant difference favoring CCM compared with no CCM for the primary end point of peak oxygen consumption, ventilatory anaerobic threshold (VAT), and quality of life. A subgroup analysis of the patients with New York Heart Association class III HF showed that the patients with an ejection fraction between 25% to 35% and ≥35% had the greatest benefit in improvement in oxygen consumption and VAT (Figure 1) [Kadish A et al. Am Heart J 2011].
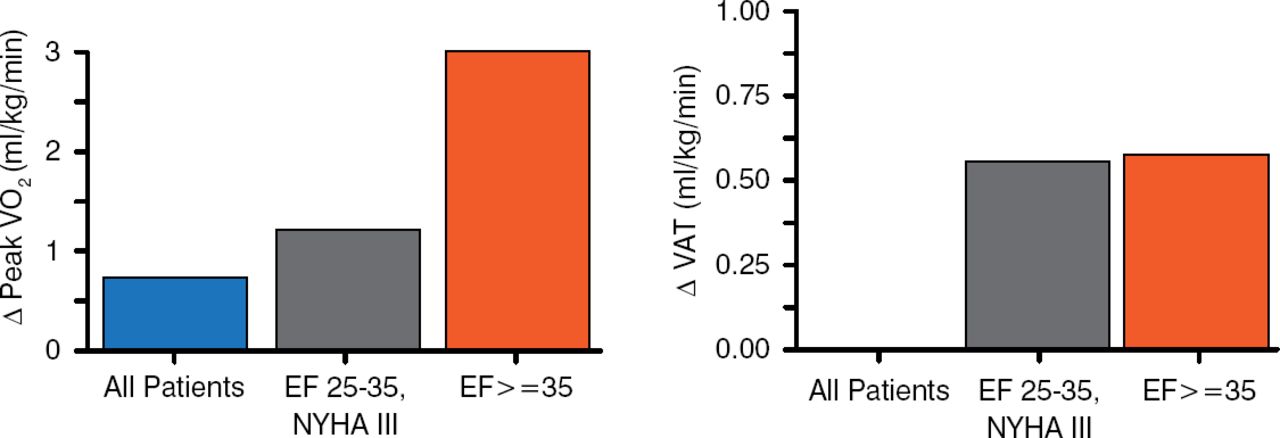
FIX-CHF-5: Subgroup Analysis of Primary Outcomes
ΔPeakVO2=change in peak oxygen consumption; EF=ejection fraction; NYHA III=New York Heart Association class III heart failure.
Source: Kadish A et al. Am Heart J 2011.
ARRHYTHMIAS IN ACUTE CORONARY SYNDROME
Bulent Gorenek, MD, Eskisehir Osmangazi University, Eskisehir, Turkey, addressed some of the arrhythmias and conduction disturbances that complicate the management of patients with acute coronary syndrome (ACS), particularly acute myocardial infarction (AMI), with an emphasis on the underlying mechanisms.
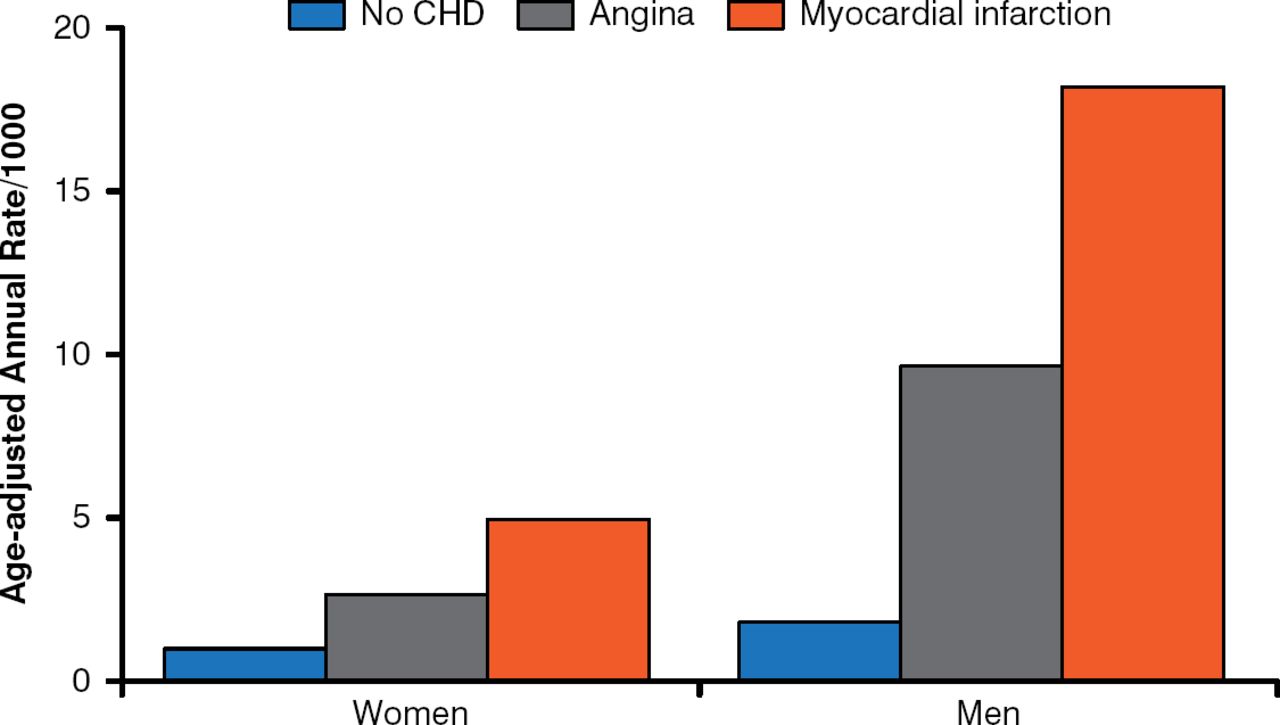
AMI is the leading cause of sudden cardiac death (SCD; Figure 2), and it becomes increasingly common with advancing age, especially in men. The risk of SCD seems to be higher with ST elevation myocardial infarction (STEMI) than non-STEMI, and 50% to 70% of SCD is due to ventricular arrhythmias.
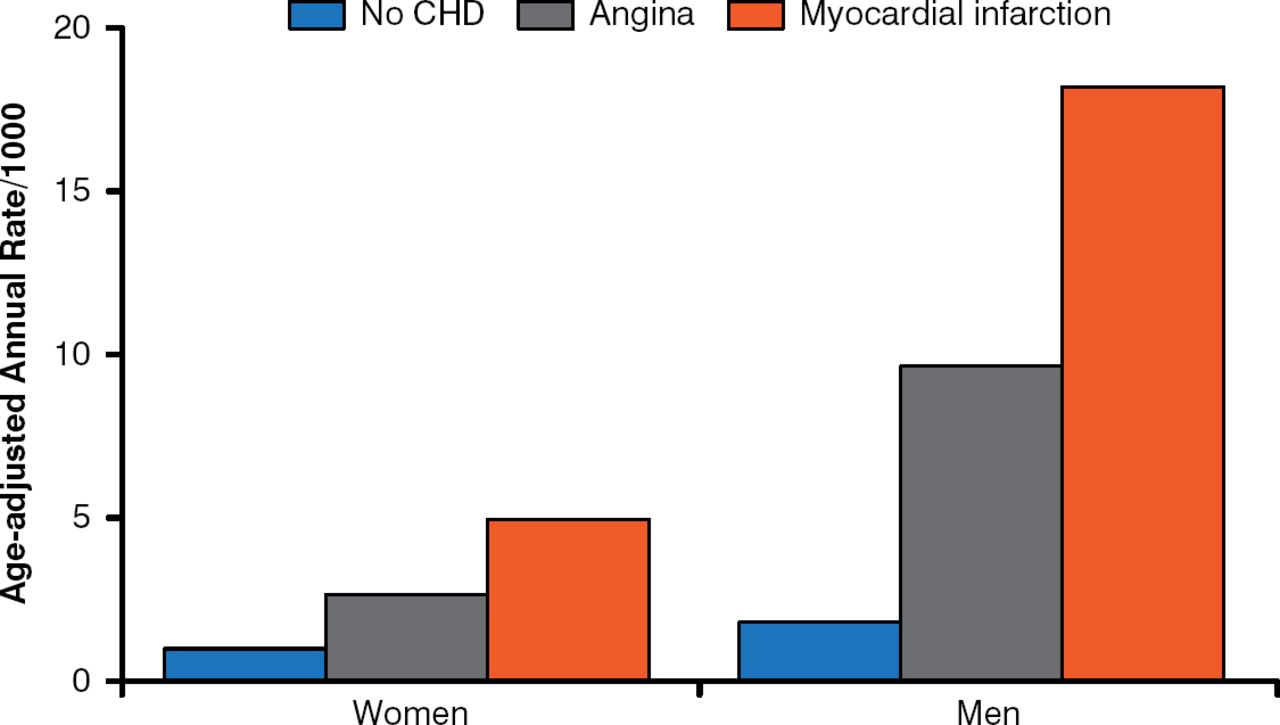
Risk of Sudden Cardiac Death by Clinical Manifestation and Sex
CHD=coronary heart disease; SCD=sudden cardiac death.
Reproduced from Kannel WB et al. Sudden coronary death in women. Am Heart J. 2009;136(2):206–212. With permission from Elsevier.
In the APEX AMI trial involving 5745 STEMI participants with a planned percutaneous coronary intervention, 329 (5.7%) experienced ventricular tachycardia or ventricular fibrillation, mostly occurring within the first 48 hours. Data from numerous trials have shown that AF occurs in ∼10% of patients with AMI [Gorenek B, Kudaiberdieva G. Curr Cardiol Rev 2012].
The 3 main mechanisms responsible for ventricular arrhythmias are automaticity, triggered activity, and reentry; other contributing factors include autonomic imbalance, electrolyte disturbances, and reperfusion. And while identifying the mechanism can be challenging, it is key to the development of an appropriate diagnosis and treatment strategy [Gorenek B, Kudaiberdieva G. Minerva Med 2013].
Arterial thromboembolism is the most significant complication associated with AF in patients with ACS, especially stroke, which can arise at any point in the clinical course of AF. Arrhythmia and conduction disturbance are also important considerations, with atrioventricular (AV) block and bundle-branch block occurring in ∼7% and 5% of cases of STEMI, respectively. AV block is also associated with an increased in-hospital and late mortality rate compared with those without AV conduction disturbance, due to the degree of myocardial damage required to develop the heart block, rather than the actual disturbance itself [Van de Werf F et al. Eur Heart J 2008; Meine TJ et al. Am Heart J 2005].
Management of arrhythmias in patients with ACS typically requires a multidisciplinary approach. Consequently, the need for a consensus document stems from the heterogeneity of their clinical course, which typically presents a dilemma to cardiovascular specialists and other physicians who care for them, Prof. Gorenek concluded.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.