

Summary
This article discusses the current evidence from guidelines and surveys that provide guidance for daily clinical practice on the management of patients with implanted devices.
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Interventional Techniques & Devices
In a session at the European Heart Rhythm Association (EHRA) EuroPace conference, a panel of experts discussed the current evidence from guidelines and surveys that provide guidance for daily clinical practice on the management of patients with implanted devices.
INDICATIONS FOR IMPLANTABLE CARDIOVERTER-DEFIBRILLATORS FOR CARDIOMYOPATHY
Alessandro Proclemer, MD, University Hospital, Udine, Italy, summarized the main results of 2 surveys conducted by the EHRA on risk stratification for sudden cardiac death (SCD) and the indications for an implantable cardioverter-defibrillator (ICD) in patients with ischemic and nonischemic cardiomyopathy [Proclemer A et al. Europace 2013; Europace 2014].
Key results of the EHRA surveys highlighted by Prof. Proclemer include the following: (1) most European centers participating in the surveys have screening evaluation programs for the prevention of SCD; (2) selection of candidates for ICDs was based primarily on clinical risk assessment and less on noninvasive and invasive diagnostic tests or implantable loop recorders, which were considered in only a minority of patients or for research purposes; and (3) most centers find specific ICD programming features useful, such as the slow ventricular tachycardia (VT) zone, activation of the long VT detection window, antitachycardia pacing (ATP) before shock, and supraventricular tachycardia discriminators.
PREVENTING CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICE INFECTIONS
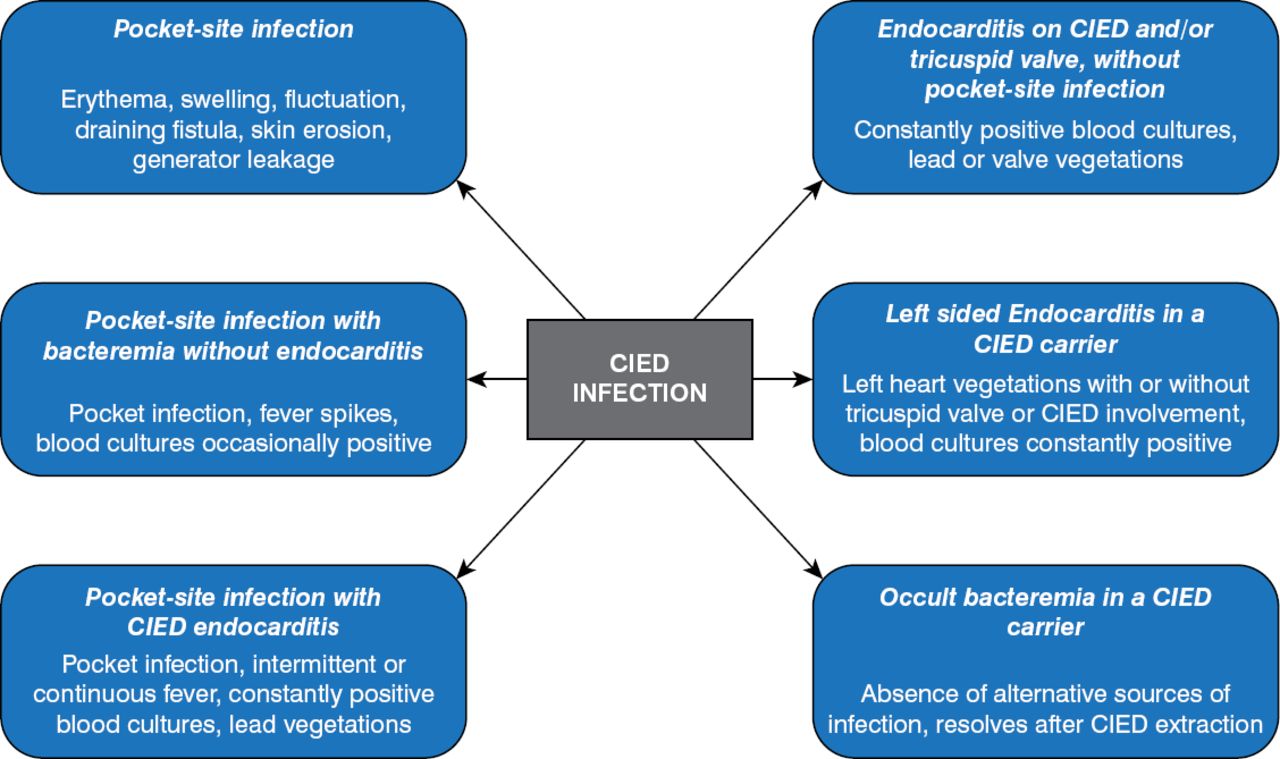
In her talk on managing problems associated with cardiac electronic devices, Maria Grazia Bongiorni, MD, University Hospital, Pisa, Italy, focused on the major problem of cardiovascular implantable electronic device (CIED) infections. Saying that the rate of CIED use is rising, she emphasized the need for accurate diagnosis for appropriate treatment (Figure 1).
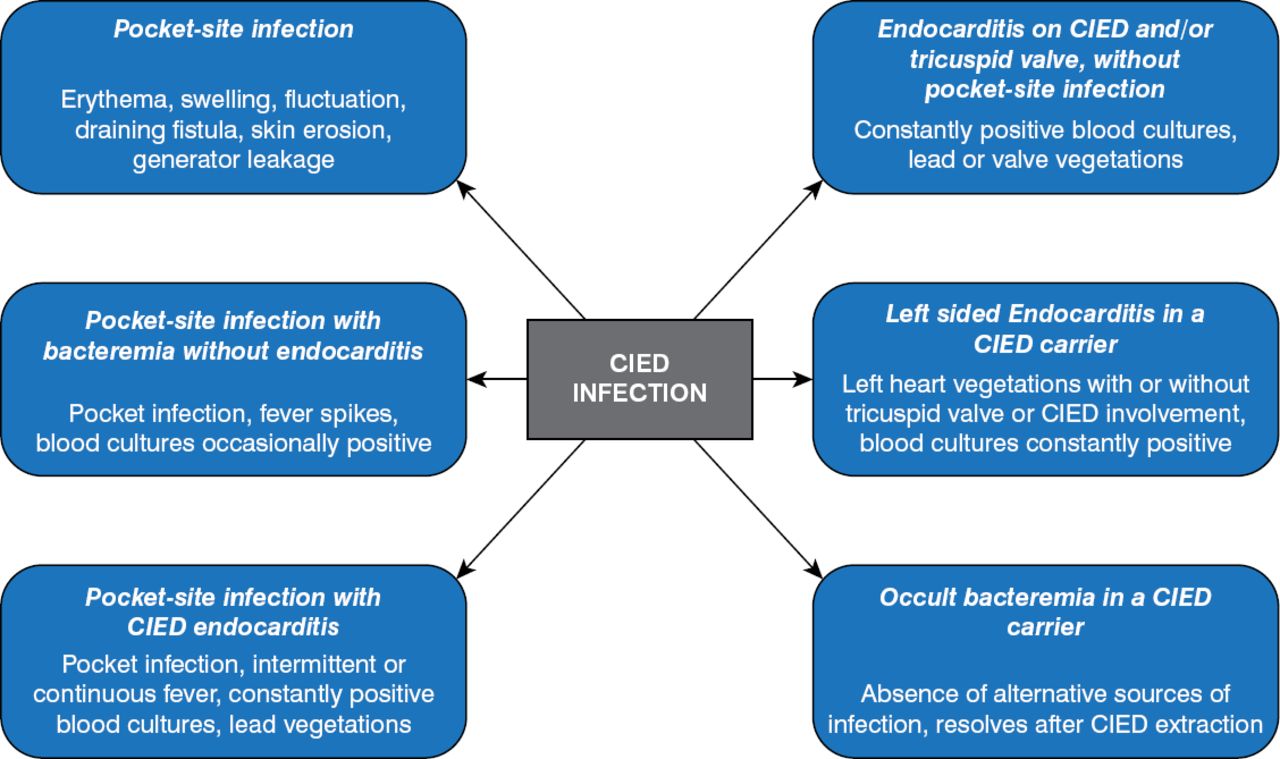
Diagnosis of CIED Infection
CIED=cardiovascular implantable electronic device.
Reproduced with permission from Springer from Durante-Mangoni E, Mattucci I, Agrusta F, Tripodi MF, Utili R. Current trends in the management of cardiac implantable electronic device (CIED) infections. Intern Emerg Med 2012;8:465–476.
Despite optimal treatment, however, Prof. Bongiorni emphasized that morbidity and mortality from CIED infection remain significant.
A major focus of her talk was therefore on the mandatory need for prevention and the evidence to support it. Data show a significant reduction in CIED infection with the use of perioperative systemic antibiotics plus antiseptics given 1 hour prior to implantation [Darouiche R et al. Pacing Clin Electrophysiol 2012].
According to recommendations from the American Heart Association and the Heart Rhythm Society (HRS), the antibiotic selected for use in this setting must have in vitro activity against staphylococci. The recommendation states that if cefazolin is chosen, it should be administered intravenously <1 hour before incision for CIED implantation. If vancomycin is chosen, it should be administered intravenously <2 hours before incision [Baddour LM et al. Circulation 2010].
As to the choice of antiseptic, Prof. Bongiorni pointed to evidence from a trial showing a 40% reduction in surgical-site infections with the use of chlorhexidine-alcohol [Darouiche RO et al. N Engl J Med 2010].
Additional ways to prevent CIED infection are to shorten the implantation time and to use the least amount of hardware possible. Unnecessary hardware has the potential not only to increase the risk for infection, she emphasized, but also to increase the risk for major complications during the extraction procedure. She therefore advocated the use of a single-lead VDD, an atrial-inhibited pacemaker when the Wenckebach cycle length is acceptable, and a single-chamber ICD for primary prevention.
MANAGEMENT OF VENTRICULAR TACHYCARDIA IN PATIENTS WITH STRUCTURAL HEART DISEASE
Derick Todd, MD, Liverpool Heart and Chest Hospital, Liverpool, United Kingdom, reviewed management of VT in patients with structural heart disease (SHD), focusing largely on the most common scenario, in which patients already have ICDs in place. He highlighted that catheter ablation is increasingly being used to treat VT in these patients and that indications for its use have been published in an expert consensus statement by the EHRA and HRS (Table 1) [Aliot EM et al. Europace 2009; Heart Rhythm 2009].
Indications for Catheter Ablation of VT in Consensus Statement
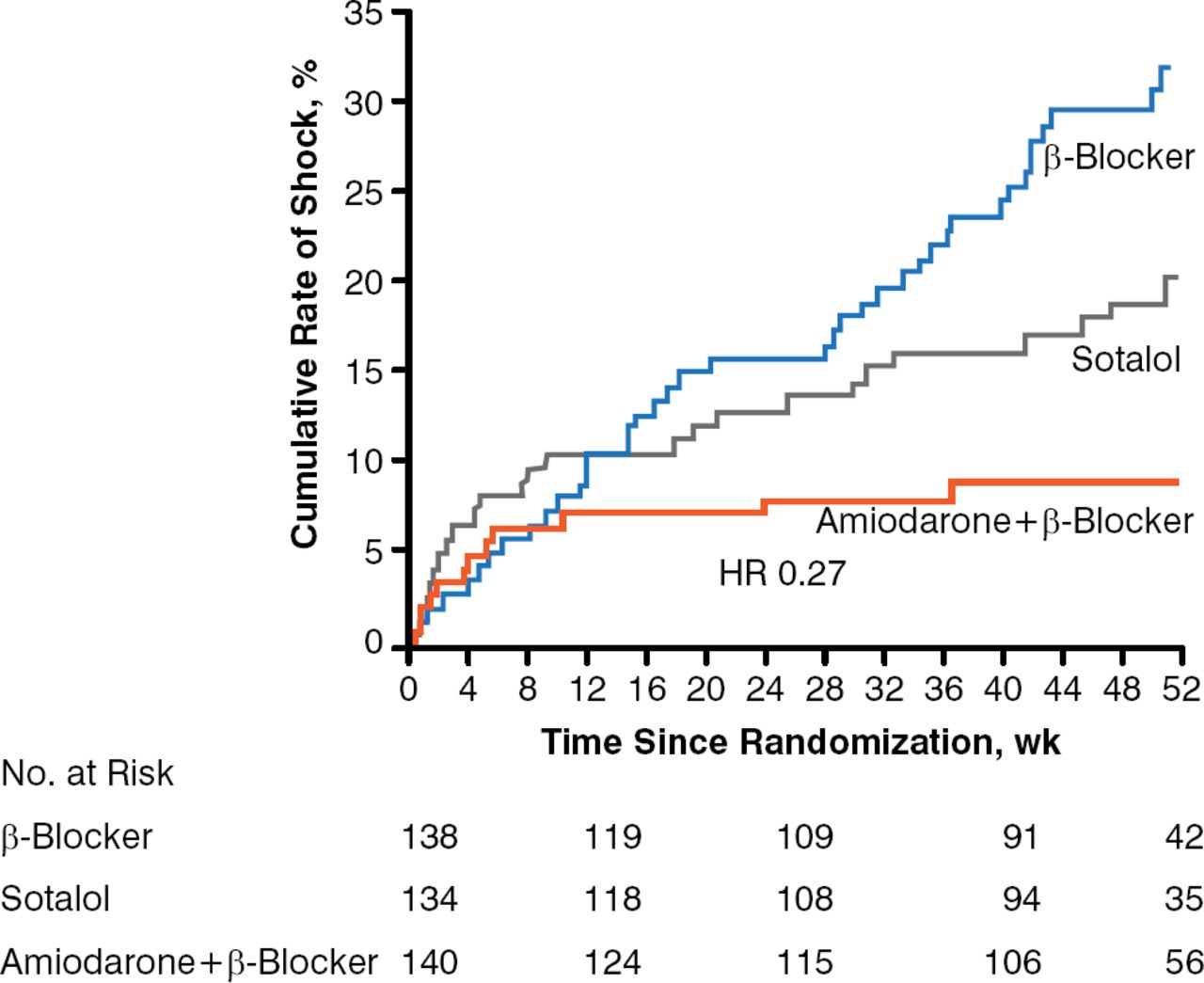
For patients in whom ablation is not an option or is not preferred, the multinational Optimal Pharmacological Therapy in Implantable Cardioverter Defibrillator Patients study [OPTIC] showed that amiodarone plus a β-blocker reduced the cumulate rate of shocks at 1 year compared with sotalol alone or a β-blocker alone after treatment (Figure 2) [Connolly SJ et al. JAMA 2006].
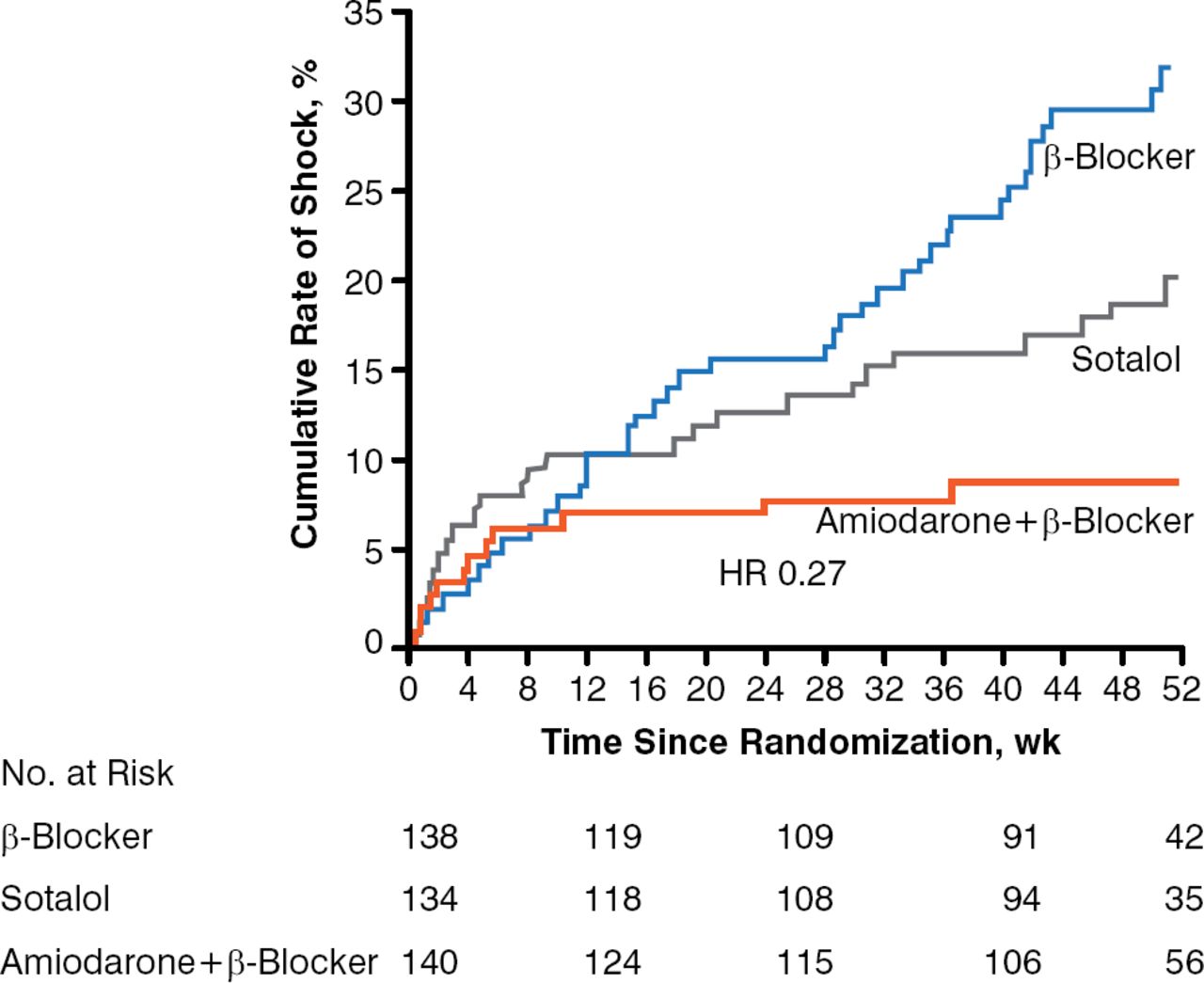
Amiodarone Plus a β-Blocker Reduced Shocks in Patients With VT and Structural Heart Disease
VT=ventricular tachycardia.
Reproduced from Connolly SJ, Dorian P, Roberts RS, et al; Optimal Pharmacological Therapy in Cardioverter Defibrillator Patients (OPTIC) Investigators. Comparison of beta-blockers, amiodarone plus beta-blockers, or sotalol for prevention of shocks from implantable cardioverter defibrillators: the OPTIC Study: a randomized trial. JAMA 2006;295(2):165–171. Copyright © 2006 American Medical Association.
Using data from his own institution, Prof. Todd described the indications for VT ablation and recent outcomes. Indications for ablation for VT include patients with ≥1 shock or frequent ATP episodes, incessant or recurrent VT, or slow VT, and patients in whom amiodarone is ineffective or poorly tolerated or not preferred, and who are younger. Table 2 shows outcomes in 52 patients who underwent ablation for VT between 2012 and 2013 at his institution. Acute success was defined as no VT or ventricular fibrillation with only 5 extra stimuli, or VT with 2 extra stimuli than at baseline.
Liverpool Heart and Chest Hospital: Acute Procedural Results With Ventricular Tachycardia Ablation (n=52)
In patients with SHD who do not have ICDs, which is a less common situation, ablation is used to treat incessant VT. Prof. Todd emphasized that these patients will need ICDs even if the ablation results are good, and if magnetic resonance imaging is considered important, it should be performed prior to implantation.
In conclusion, ablation is increasingly being used to treat VT in patients with SHD with encouraging results. In patients not treated with ablation, amiodarone combined with a β-blocker is the best medical treatment for patients in whom ablation is not performed.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.