

Summary
This article discusses the use of an oral anticoagulant over aspirin for stroke prevention in patients with atrial fibrillation, even among older patients.
- Cerebrovascular Disease
- Cardiology Clinical Trials
- Arrhythmias
- Cardiology & Cardiovascular Medicine
- Cerebrovascular Disease
- Cardiology Clinical Trials
- Arrhythmias
Leif Friberg, MD, PhD, Karolinska Institute, Stockholm, Sweden, laid out an argument in favor of an oral anticoagulant (OAC) over aspirin for stroke prevention in patients with atrial fibrillation (AF), even among older patients.
The reluctance to use anticoagulants with patients with AF dates back to the 1980s, said Prof. Friberg, when the risk was perceived to be too high in large segments of the population, even in patients with mitral stenosis. During this same period, the utility of aspirin to prevent myocardial infarction was being discovered [Seshasai SR et al. Arch Intern Med 2012], and this utility was routinely extrapolated to include stroke prevention by AF as a milder alternative to OACs. The use of aspirin by patients with AF was bolstered by a meta-analysis of a series of small studies, most enrolling <1200 patients, showing it to be superior to placebo in reducing stroke risk in AF. The largest of these studies, the United Kingdom Transient Ischaemic Attack Aspirin trial, in which 2435 patients were enrolled, found no significant effect of aspirin compared with placebo, and a trend toward a negative effect of aspirin on fatal stroke. None of the individual trials, except for the Stroke Prevention in Atrial Fibrillation study [SPAF], achieved significance in favor of aspirin, he noted. Overall, there was no significant effect of aspirin when disabling or fatal strokes were counted.
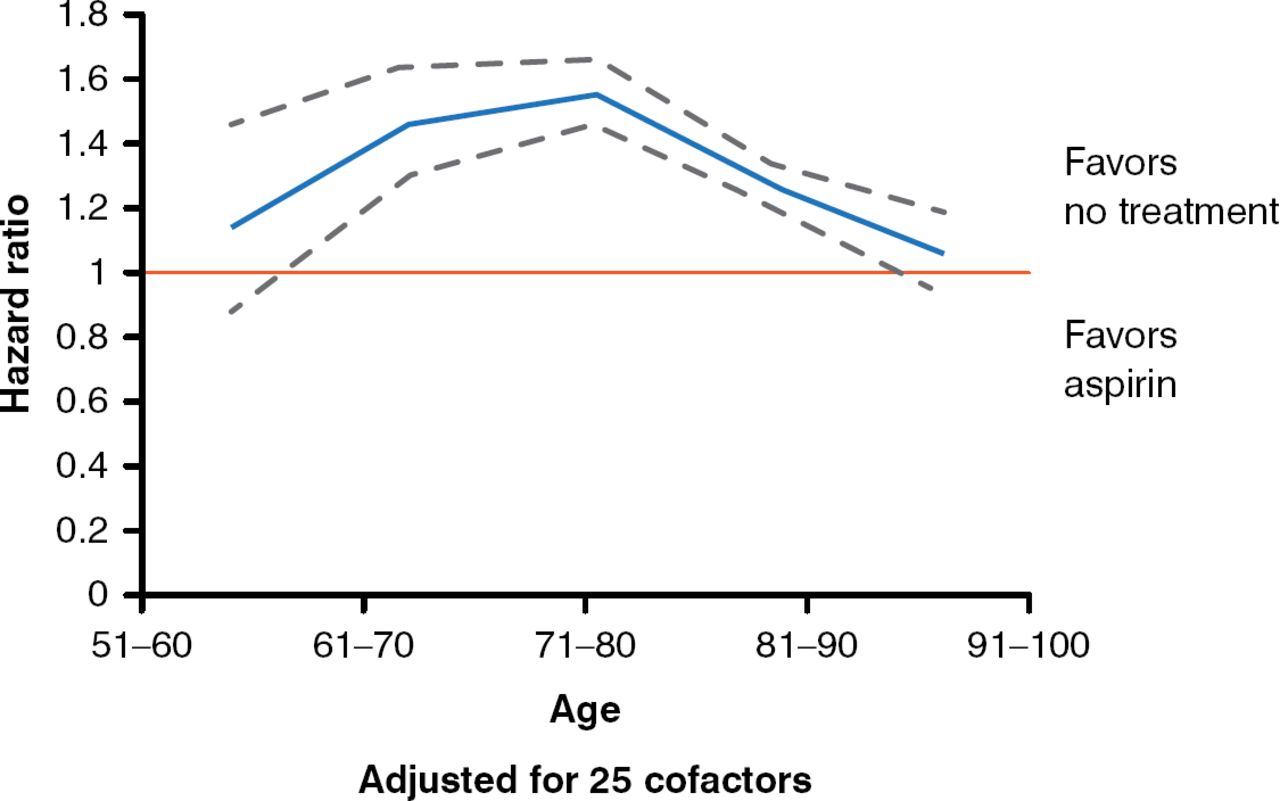
An analysis of all individuals with a diagnosis of AF from 2005 to 2008 in the National Swedish Patient register, of whom 58,671 were treated with aspirin as monotherapy and 56,514 received no antithrombotic treatment, found no benefit with aspirin in preventing thromboembolism or ischemic stroke, with a mean follow-up of 1.5 years, compared with no treatment [Själander S et al. Europace 2014]. Patients on aspirin were older and had more comorbidities, but adjustment for cofactors did not change the results (Figure 1).
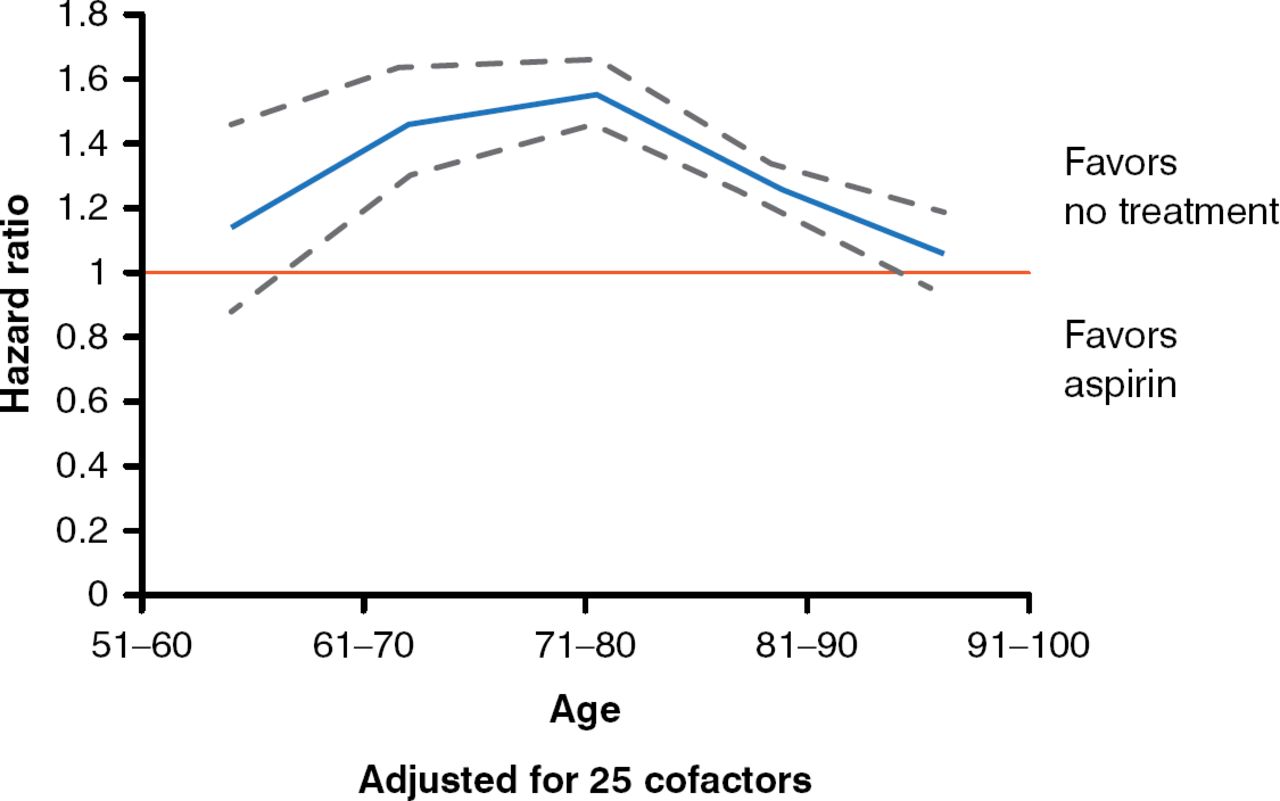
Adjusted Rates of Thrombembolism by Aspirin Treatment or No Treatment
Reproduced from Själander S et al. Atrial fibrillation patients do not benefit from acetylsalicylic acid. Europace 2014;16:631–638. With permission from the European Society of Cardiology.
A reanalysis of 12 randomized controlled trials found no protective effect of aspirin on ischemic stroke after age 75 years [van Walraven C et al. Stroke 2009]. The Copenhagen AFASAK (aspirin vs warfarin standard dose) study found more bleeding events in warfarin-treated patients with AF than in those treated with aspirin, but the warfarin group spent only 42% of the time in the therapeutic range (TTR), defined as an international normalized ratio (INR) of 2.8 to 4.2. The Atrial Fibrillation Clopidogrel Trial With Irbesartan for Prevention of Vascular Events trial [ACTIVE W] found that the TTR has to be >65% for warfarin to be superior to aspirin in preventing stroke in AF [The ACTIVE Writing Group. Lancet 2006]. This finding is confirmed in the Birmingham Atrial Fibrillation Treatment of the Aged Study, in which patients had a mean age of 81.5 years; their TTR was 67%, with a target INR of 2.0 to 3.0 [Mant J et al. Lancet 2007].
Among the new OACs, no significant difference in the rate of major bleeding events was found between apixaban and aspirin [Connolly SJ et al. N Engl J Med 2011], noted Prof. Friberg.
These data led the European Society of Cardiology to advise against the use of aspirin for the management of AF and to use anticoagulation in appropriately selected patients at risk for embolic stroke [Camm AJ et al. Europace 2012].
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.