

Summary
The European Society of Hypertension and European Society of Cardiology (ESH—ESC); the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC-8); and the American Society of Hypertension and International Society of Hypertension (ASH—ISH) have each published guidelines on hypertension in the past year. This article discusses and debates the relative merits of each guideline.
- Hypertensive Disease
- Cardiology Guidelines
- Cardiology & Cardiovascular Medicine
- Hypertensive Disease
- Cardiology Guidelines
The European Society of Hypertension and European Society of Cardiology (ESH—ESC); the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC-8); and the American Society of Hypertension and International Society of Hypertension (ASH—ISH) have each published guidelines on hypertension in the past year. In a session at the Joint Meeting of the European Society of Hypertension (ESH) and International Society of Hypertension (ISH), a panel of experts discussed and debated the relative merits of each guideline. One central focus of the discussions, which is also focused on in this review, was on the process by which guidelines are generated and how this leads to different recommendations.
ESH—ESC GUIDELINES
Giuseppe Mancia, MD, University of Milano-Bicocca, Milan, Italy, one of the two chairpersons of the ESH-ESC guidelines, focused his talk on a comparison between the ESH—ESC and JNC-8 guidelines and the more restrictive criteria for study selection used in the JNC-8 guidelines (Table 1).
Different Criteria for Study Inclusion Used in JNC-8 and ESH—ESC Hypertension Guidelines
Although both guidelines were based on an extensive review of the literature and gave the highest priority to randomized controlled trials (RCTs) for study inclusion, Dr. Mancia highlighted potential drawbacks of the JNC-8 guidelines' more restrictive data set. One drawback is the exclusion of studies that included both hypertensive (HT) and normotensive (NT) persons. He emphasized that the decisions about the blood pressure threshold for drug treatment need to consider RCTs that involve HT and NT persons and that several landmark RCTs have included patients with a normal-to-high entry blood pressure range.
He also challenged the inclusion of RCTs only with hard outcomes, highlighting the clinical and practical relevancy of evaluating treatment effects on such things as subclinical organ damage, new-onset diabetes, and treatment adherence.
Dr. Mancia also questioned how the JNC-8 could deny the scientific value of observational studies, when, for example, these types of studies have provided the only evidence for lifetime hypertensive treatment. He emphasized that if the JNC-8 guidelines based their recommendations only on RCTs, their recommendation would be to stop treatment after 5 to 6 years.
Although the JNC-8 claims to be rigorously based on evidence, 6 out of their 10 recommendations were defined as “expert opinion,” in line with the low level of evidence attributed to most recommendations in the ESH—ESC guidelines. He emphasized that all guidelines are based more on opinion and consensus than on evidence, that no good science is available for a great part of daily medical practice, and that recommendations must make large use of common sense and clinical experience.
Based on these differences, he concluded that the ESH—ESC guidelines try to help doctors tailor treatment when possible despite the infeasibility of individualizing treatment in all patients.
JNC-8 GUIDELINES
John B. Kostis, MD, John G. Detwiler Professor of Cardiology, Director, Cardiovascular Institute, Rutgers Robert Wood Johnson Medical School, New Brunswick, NJ, USA, also discussed the differences among the guidelines in terms of the types of evidence used as the foundation for recommendations and rating their strength. He highlighted that the limited number of recommendations in the JNC-8 is based on the decision by the panel to review the evidence from RCTs on only a limited number of questions deemed to be of highest priority.
Overall, he emphasized a number of problems with guidelines (Table 2) and concluded that more focus in RCTs needs to be on primordial disease prevention instead of events.
Points to Consider When Weighing the Evidence Used to Generate Guidelines
ASH—ISH 2014 GUIDELINES
Ernesto L. Schiffrin, MD, PhD, President of the International Society of Hypertension; Canada Research Chair in Hypertension and Vascular Research, Lady Davis Institute for Medical Research; Physicianin-Chief, Jewish General Hospital; and Professor and Vice Chair, Department of Medicine, McGill University, Montreal, Canada, emphasized that the publication of several guidelines is good because it generates needed discussion on blood pressure control and a critical review of the evidence. Instead of focusing on the evidence of each guideline, however, he highlighted that a main aim of the ASH—ISH guidelines was to offer short and easy-to-implement recommendations that are particularly useful in low- and middle-income countries with resource-poor healthcare systems [Weber MA et al. J Hypertens 2014]. Unlike this approach, the ESH—ESC guidelines are very long and include diagnostic approaches such as intima-media thickness and pulse wave velocity that are of unproven value in terms of improving outcomes, and the JNC-8 guidelines are very limited and offer few recommendations, which despite being titled evidence-based guidelines, are in fact largely based on expert opinion.
He emphasized the need to better address how to implement guidelines in a simple way to improve blood pressure control around the world and not to focus on the minor differences among guidelines or the need to strive for perfect evidence.
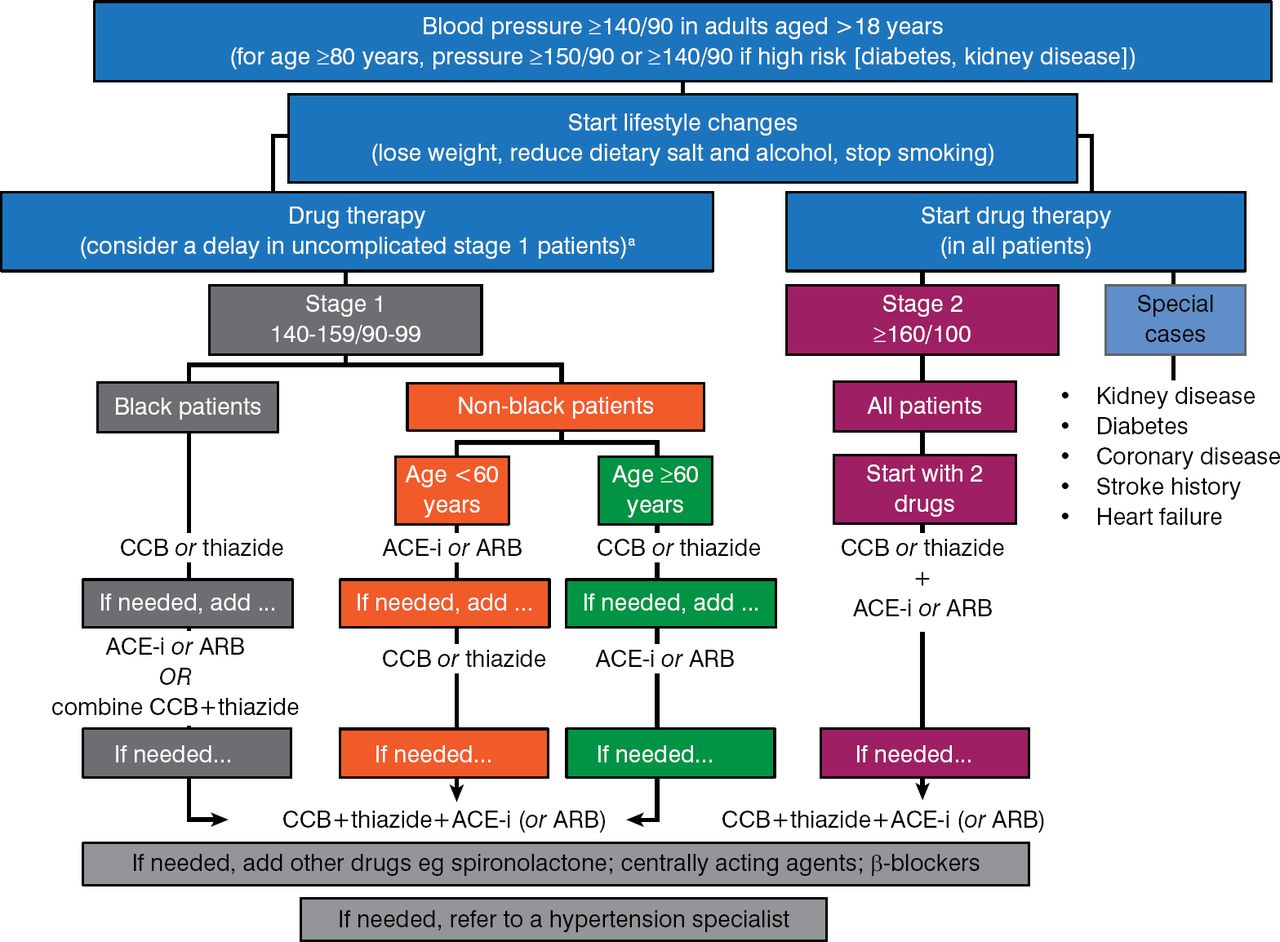
To this end, the ASH—ISH offers a simple algorithm that he said can be carried in one's pocket or placed in the clinic to facilitate implementation of blood pressure—reducing strategies (Figure 1).
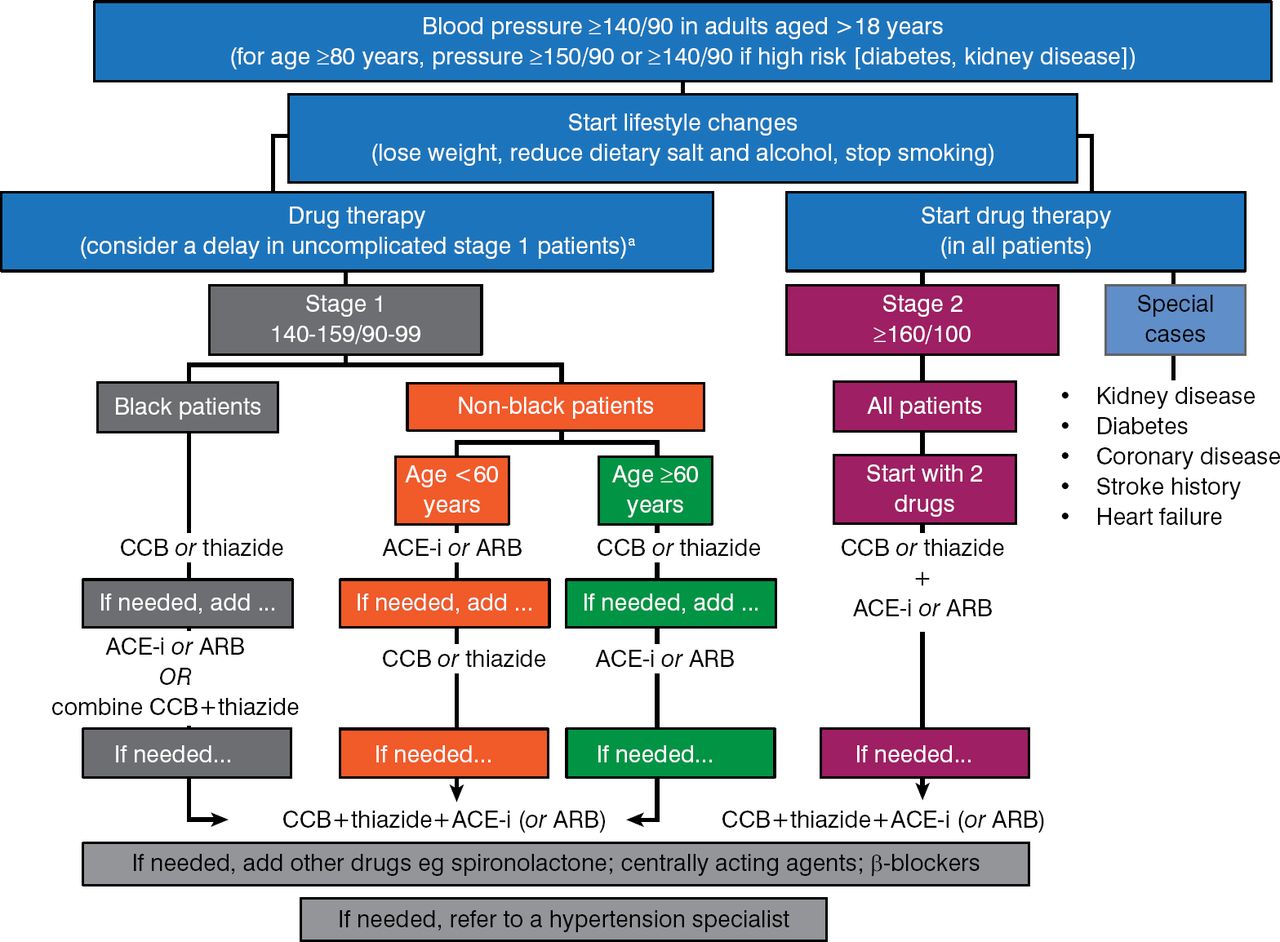
Algorithm From the ASH—ISH Guidelines for Blood Pressure Control in Adults
a In stage 1 patients without other cardiovascular risk factors or abnormal findings, some months of regularly monitored lifestyle management without drugs can be considered.
Reproduced from Weber MA et al. Clinical practice guidelines for the management of hypertension in the community a statement by the American Society of Hypertension and the International Society of Hypertension. J Hypertens 2014;32(1):3–15. With permission from Lippincott Williams and Wilkins.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.