

Summary
This article discusses advances in osteoporosis in postmenopausal women, in glucocorticoid-induced osteoporosis, and secondary to rheumatic diseases.
- Bone Density & Structure Disorders
- Metabolic Bone Disease
- Metabolic Bone Disease
- Bone Density & Structure Disorders
- Rheumatology
Willem F. Lems, MD, VU University Medical Center and Reade, Amsterdam, The Netherlands, discussed advances in osteoporosis in postmenopausal (PM) women, in glucocorticoid-induced osteoporosis (GIOP), and secondary to rheumatic diseases (RDs).
POSTMENOPAUSAL OSTEOPOROSIS
The bisphosphonates (BSP) alendronate, risedronate (RISE), and zoledronic acid, and the monoclonal antibody denosumab (DEN), are the only agents shown to reduce vertebral and nonvertebral fractures. It is not known if patients with PM osteoporosis who have received 5 years of BSP therapy should continue or stop treatment; data for the long-term effects of BSP are lacking.
Atypical femoral fracture (AFF) is a serious adverse event (AE) related to the duration of BSP therapy, and it is also associated with DEN. AFFs are stress fractures in the femoral shaft (or occasionally another location), are usually preceded by prodromal pain, and heal poorly [Shane E et al. J Bone Miner Res 2014]; histology shows bone remodeling in the absence of healing. Prof. Lems said that the benefit of fracture reduction with BSP and DEN nevertheless surpasses the risks of AEs like AFF and osteonecrosis of the jaw (ONJ). In a study titled the Effect of Teriparatide on Fracture Healing in Patients With Incomplete Atypical Femur Fractures [NCT01896011], which was conducted with PM women with bilateral (n=17) or unilateral (n=5) AFF who had used BSP for a mean of 12 years, treatment with teriparatide (TERI; recombinant parathyroid hormone) for a mean of 18.8 months was associated with healed (n=2), healing (n=5), or stable (n=12) AFF.
DEN treatment resulted in a continued increase in bone mineral density (BMD) and a stable, low incidence of vertebral and nonvertebral fractures; this was seen at ≥8 years (5 years in patients who crossed over from placebo to DEN) of follow-up in the extension of FREEDOM, a Study to Evaluate Denosumab in the Treatment of Postmenopausal Osteoporosis [NCT00089791].
New anti-osteoporotic agents are under development. In a Phase 2 trial comparing romosozumab (ROMO), a monoclonal antibody against sclerostin, with placebo, alendronate, or TERI in PM women with low BMD [McClung MR et al. N Engl J Med 2014], the highest dose of ROMO increased BMD in the lumbar spine, hip, and femoral neck to a greater extent than the other treatments. Odanacatib, a cathepsin K inhibitor, increased lumbar spine and femoral neck BMD and reduced a marker of bone resorption in PM women with low BMD [Brixen K et al. J Clin Endocrinol Metab 2013]. Two years of therapy with the combination of DEN plus TERI in PM women with osteoporosis showed increased BMD in the lumbar spine, femoral neck, and total hip compared with either agent alone in the DATA extension study [Leder BZ et al. J Clin Endocrinol Metab 2014]. These agents will be studied further for efficacy and safety.
A case–control study showed that after 5 years of follow-up, femoral strength correlated with the femoral neck area BMD T-score, and it defined a threshold for hip fracture ∼T≤–1.3 [Kopperdahl DL et al. J Bone Miner Res 2014]. Prof. Lems said that treatment increasing BMD to this level in patients with osteoporosis might indicate treatment success.
Genetic studies of osteoporosis risk are ongoing. For example, some mutations in the gene for plastin 3 (PLS3), an actin-bundling protein, are associated with X-linked osteoporosis with fractures [van Dijk FS et al. N Engl J Med 2013].
OSTEOPOROSIS IN PATIENTS TREATED WITH GLUCOCORTICOIDS
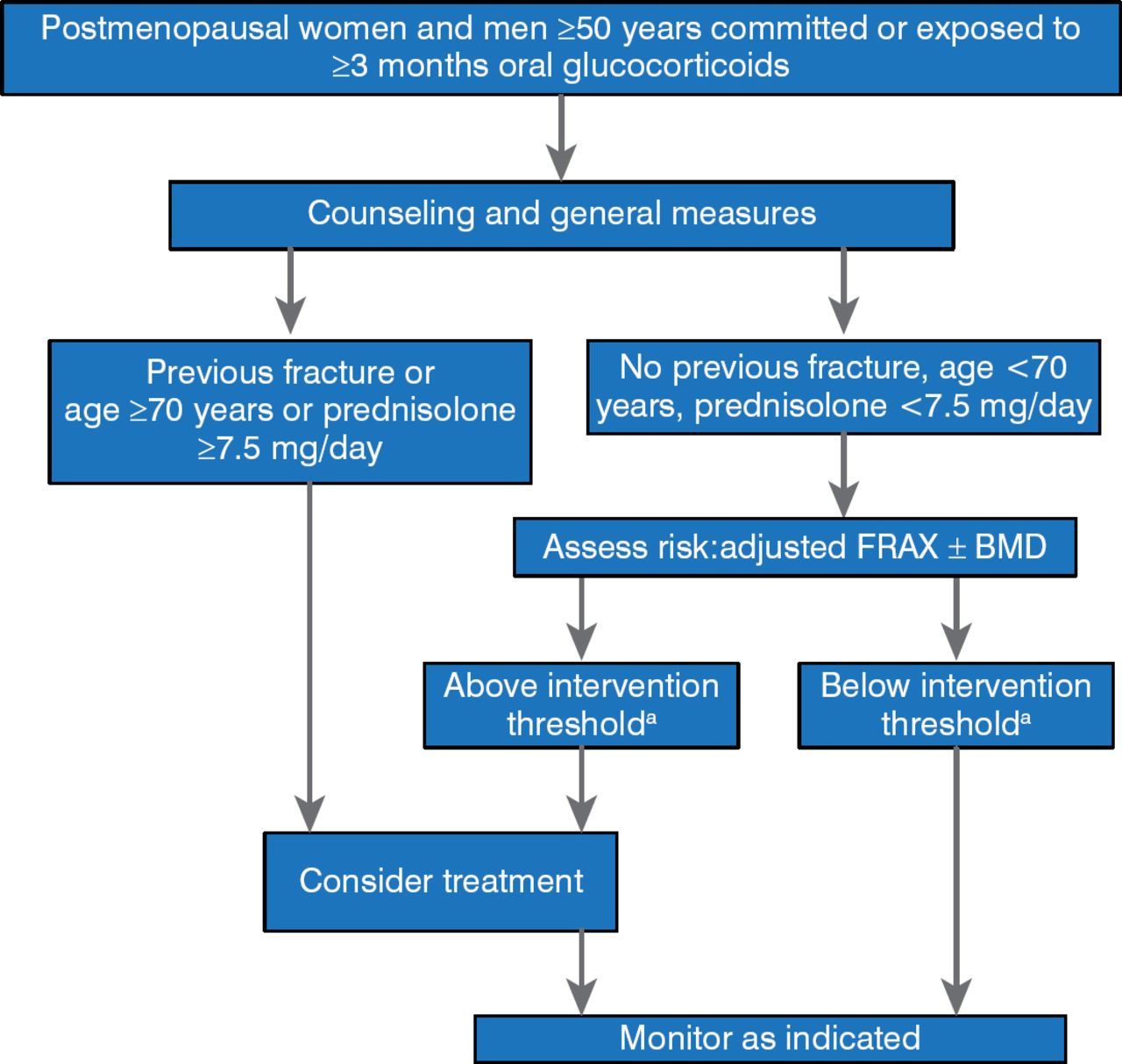
The fracture rate in patients treated with high-dose glucocorticoids (GCs) is high and dose related; GCs increase bone resorption and decrease bone formation. In patients with RDs, the disease itself as well as the GCs used in treatment may have a negative effect on BMD. Treatment with lower dose GCs and with BSPs might prevent osteoporosis, but this depends on achieving effective control of the RD with lower dose GCs. A framework for the development of guidelines for the management of GIOP is shown in Figure 1 [Lekamwasan S et al. Osteoporos Int 2012].

Guidelines for Glucocorticoid-Induced Osteoporosis
BMD=bone mineral density.
a Threshold will vary according to country.
Reproduced from Lekamwasan S et al. A framework for the development of guidelines for the management of glucocorticoid-induced osteoporosis. Osteoporos Int 2012;23:2257–2276. With permission from Springer Verlag.
EuroGIOPS is a study of men with GIOP treated with TERI or RISE [Gluer CC et al. J Bone Miner Res 2013], and it is one of the few studies of osteoporosis in men. At 18 months, RESI significantly increased lumbar spine trabecular BMD and vertebral strength compared with RISE. Changes in bone strength correlated positively with bone turnover markers in the group treated with TERI [Farahmand P et al. Osteoporos Int 2013].
OSTEOPOROSIS SECONDARY TO RHEUMATIC DISEASES
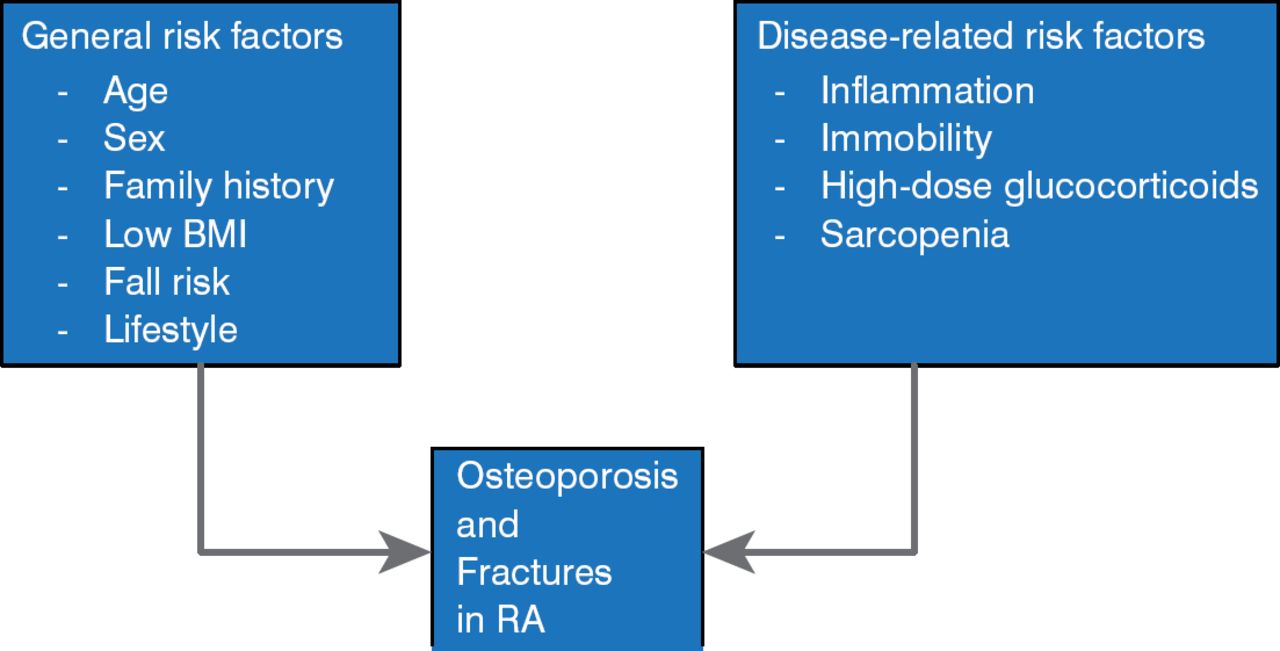
As mentioned, osteoporosis in patients with RD may be secondary to their disease itself. In patients whose disease is not adequately treated, inflammatory molecules (eg, tumor necrosis factors and interleukins) may affect bone remodeling. Upregulated osteoclasts may increase bone resorption, and downregulated osteoblasts may decrease bone formation. Risk factors for generalized bone loss and fractures in patients with rheumatoid arthritis (RA) are shown in Figure 2 [Vis M et al. Osteoporos Int 2013].

Risk Factors of Generalized Bone Loss and Fractures in Rheumatoid Arthritis
BMI=body mass index; RA=rheumatoid arthritis.
Reproduced from Vis M et al. Can bone loss in rheumatoid arthritis be prevented? Osteoporos Int 2013;24:2541–2553. With permission from Springer Verlag.
If inflammation does play a role in osteoporosis in RA, then agents that decrease inflammation should improve BMD. In patients with RA treated with adalimumab, those whose disease responded well had an increased BMD, whereas those whose disease did not respond or responded only moderately lost BMD in both the hip and spine. [Krieckaert CL et al. Rheumatology (Oxford) 2013].
New methods of bone imaging with higher resolution, low-radiation dosage, and decreased acquisition time, such as high-resolution peripheral quantitative computed tomography (HR-pQCT), should improve the ability to visualize bone and joint microarchitecture at baseline and during treatment and fracture healing. The equipment to perform HR-pQCT currently is very expensive, however, and it is being used in the research setting.
Decreased BMD is also seen in patients with RA who have anticitrullinated protein antibodies [Kleyer A et al. Ann Rheum Dis 2014]. The presence of these antibodies, and the cortical bone changes associated with them, can occur before RA symptoms appear, supporting the role of RA in causing osteoporosis.
BPs and DEN are effective agents for treating osteoporosis, although the optimal duration of therapy is unknown. Newer agents with different mechanisms of action are being developed. In addition to treating osteoporosis after it develops, adequate treatment of the inflammation associated with RA helps to reduce disease-associated bone loss.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.