

Summary
Remote monitoring using a multiparametric alert algorithm in patients with heart failure (HF) and a cardiac resynchronization therapy device (CRT-D) or implanted cardiac defibrillator (ICD) results in a decrease in all-cause mortality. This article presents data from a post hoc analysis of the Influence of Home Monitoring on the Clinical Status of Heart Failure Patients With an Impaired Left Ventricular Function trial [IN-TIME; NCT00538356].
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Heart Failure
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Heart Failure
Remote monitoring using a multiparametric alert algorithm in patients with heart failure (HF) and a cardiac resynchronization therapy device (CRT-D) or implanted cardiac defibrillator (ICD) results in a decrease in all-cause mortality. Gerhard Hindricks, MD, PhD, Herzzentrum Leipzig, Leipzig, Germany, presented data from a post hoc analysis of the Influence of Home Monitoring on the Clinical Status of Heart Failure Patients With an Impaired Left Ventricular Function trial [IN-TIME; NCT00538356].
Patients with HF have a high risk of experiencing substantial morbidity, with a generally poor prognosis. Interestingly, certain clinical parameter trends frequently occur prior to patient re-hospitalization or death due to worsening HF [Hindricks G et al. ESC 2013]. The purpose of the IN-TIME trial was to evaluate the utility of remote monitoring on clinical outcomes using a multiparametric alert approach in patients with HF and a CRT-D or an ICD.
In the multicenter, open-label, Phase 4 IN-TIME trial, 664 patients with HF, who required a CRT-D or dual-chamber ICD, were randomly assigned to home monitoring (n=333) or to conventional monitoring (n=331) groups. Patients were classified as New York Heart Association (NYHA) Class II or III with a left ventricular ejection fraction (LVEF) of less than or equal to 35%, and were on stable drug therapy. Patients were excluded if they had permanent atrial fibrillation. The mean age of patients with a CRT-D was 67 years; of these, 78% were male, 26% were NYHA Class II, 61% had coronary artery disease (CAD), and 34% had renal insufficiency. The mean intrinsic QRS duration for these patients was 148 ms. By comparison, the mean age of patients with an ICD was 63 years; of these, 85% were male, 67% were NYHA Class II, 80% had CAD, and 24% had renal insufficiency. The mean LVEF in these patients was 27%, and the mean intrinsic QRS duration was 114 ms.
The primary end point was the modified Packer score—a clinical composite that comprises mortality, NYHA class global self-assessment, and the need for overnight hospitalization for worsening heart failure. The major secondary end point was all-cause mortality. The patient's condition was considered to be “worsened” if the following criteria occurred: death, overnight hospitalization for worsening HF, worsening in NYHA class, and deterioration in global self-assessment score.
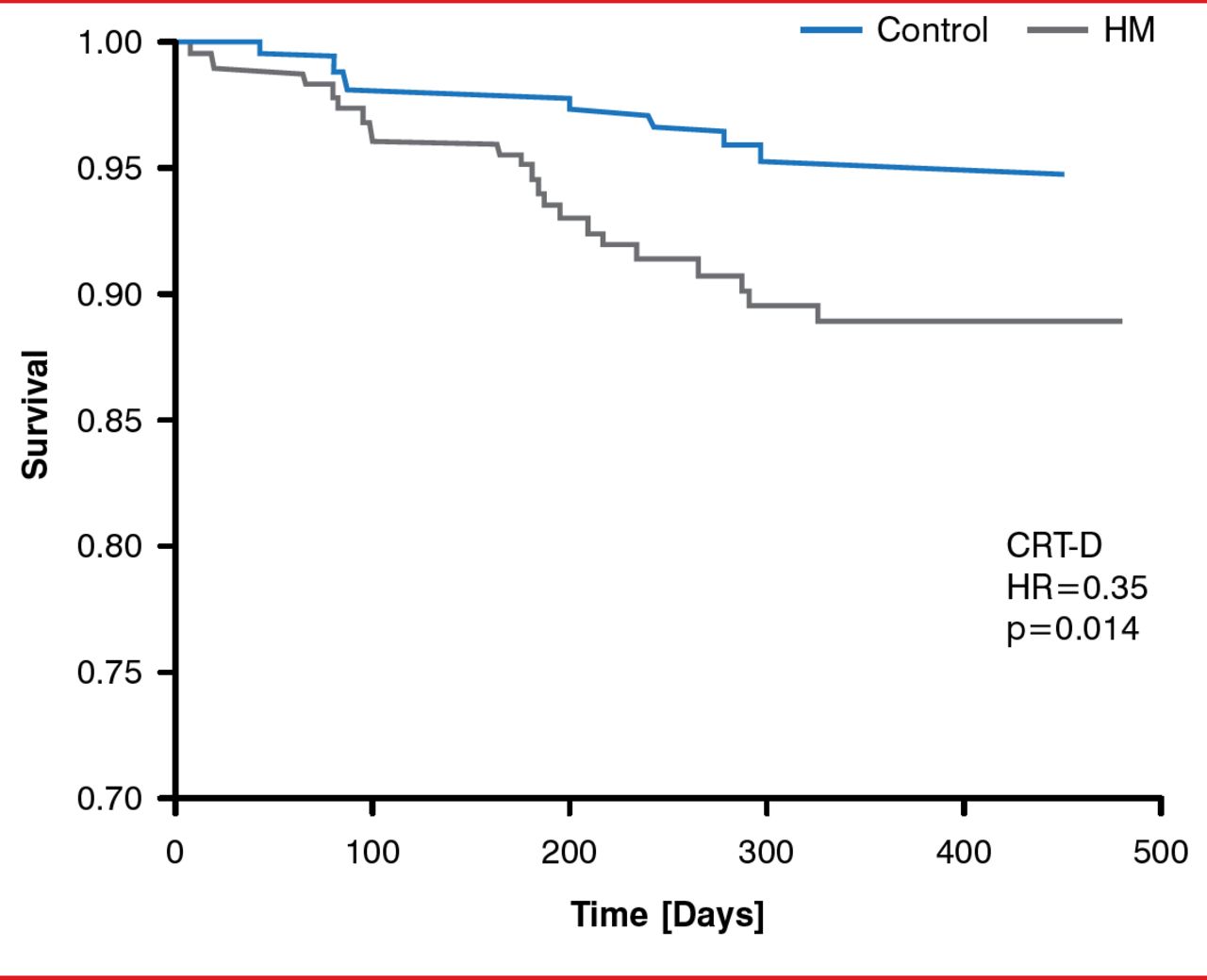
There was no significant difference in the modified Packer score between patients in the conventional and home monitoring groups, regardless of the device type (30% vs 23%, p=0.10 for CRT-D; 23% vs 14%, p=0.06 for ICD). However, mortality rates was significantly lower for patients with CRT-D in the home monitoring group as compared with those in the conventional monitoring group (HR, 0.35; p=0.014; Figure 1); similar lower mortality rates were observed for patients with an ICD in the home monitoring group as compared with those in the conventional monitoring group.
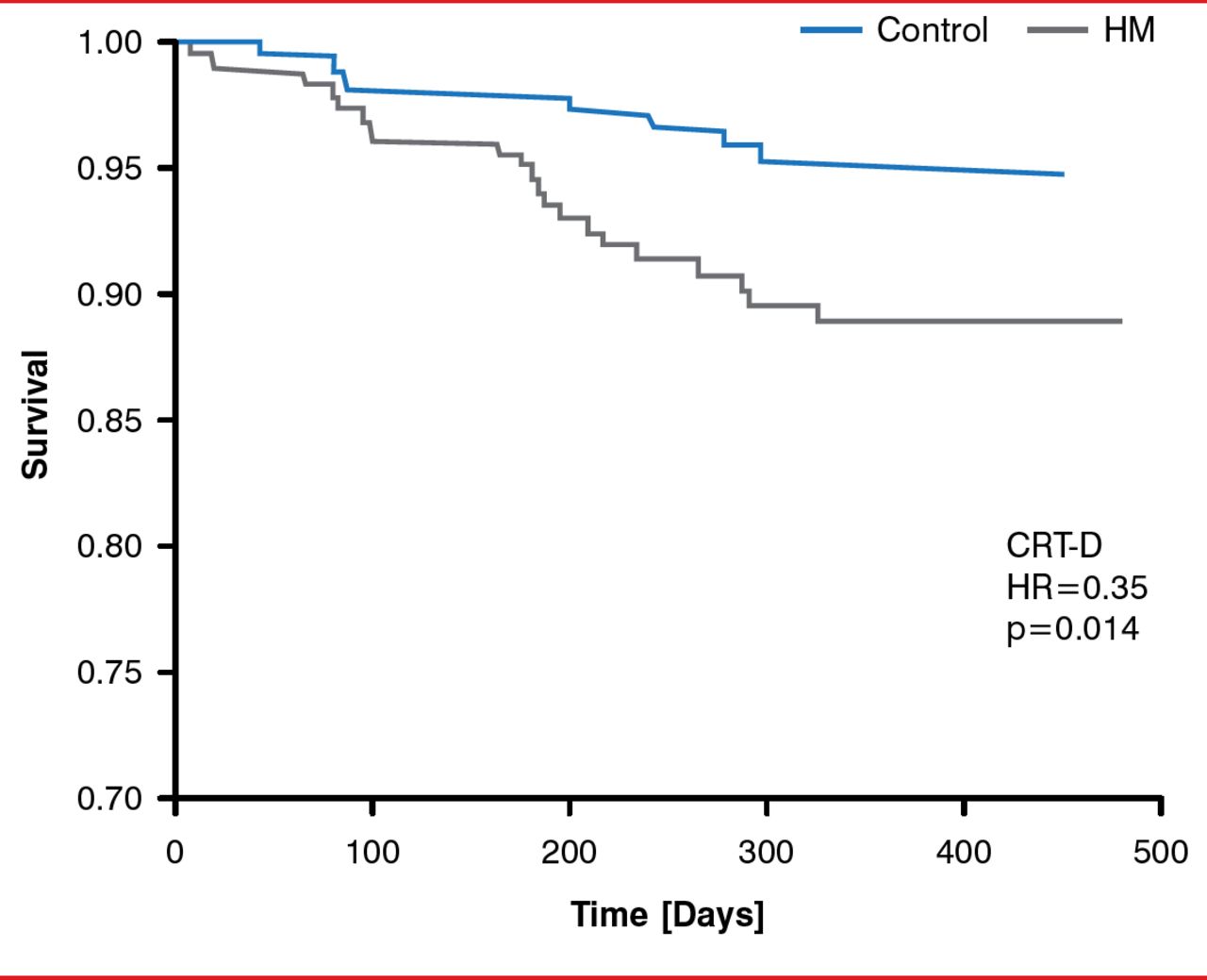
Effect of Remote Home Monitoring on Mortality in Patients With CRT-D
CRT-D=cardiac resynchronization therapy device; HM=home monitoring.
Reproduced with permission from G Hindricks, MD, PhD.
In patients with a CRT-D or an ICD in the home monitoring group, 1.7 and 1.1 clinical events per patient-year were detected, respectively. The commonly detected clinical events included atrial fibrillation, CRT (in CRT-D group) and lead parameters. In addition, technical and medical issues were identified in 291 and 146 of patients with a CRT-D and an ICD in the home monitoring group, respectively.
Prof. Hindricks concluded that there is a clinical benefit in using remote home monitoring for implantbased devices, regardless of the type of device employed (CRT-D or ICD).
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.