

Summary
Cardiogenic shock (CS) is a condition of severe tissue hypoperfusion caused by cardiac dysfunction. Given the high rate of in-hospital and short-term mortality associated with CS, a prediction score could prove useful for risk stratification to guide optimal resource utilization. The objective of the CardShock Study and Registry [NCT01374867] was to assess the contemporary clinical picture and outcomes of CS to develop a risk prediction score for short-term mortality.
- Heart Failure
- Cardiology Clinical Trials
- Heart Failure
- Cardiology & Cardiovascular Medicine
- Cardiology Clinical Trials
Cardiogenic shock (CS) is a condition of severe tissue hypoperfusion caused by cardiac dysfunction. Given the high rate of in-hospital and short-term mortality associated with CS, a prediction score could prove useful for risk stratification to guide optimal resource utilization. Johan Lassus, MD, PhD, Helsinki University Central Hospital, Helsinki, Finland, presented a new risk scoring system for patients with CS.
The objective of the CardShock Study and Registry [NCT01374867] was to assess the contemporary clinical picture and outcomes of CS to develop a risk prediction score for short-term mortality. Subjects were enrolled in the study within 6 hours of a diagnosis of CS (defined as systolic blood pressure [SBP] less than 90 mm Hg for 30 minutes or the need for vasopressor therapy to maintain adequate perfusion pressure) and more than or equal to 2 of the following signs of hypoperfusion: altered mental status/confusion, cold periphery, oliguria or blood lactate above 2 mmol/L. The primary outcome measure was all-cause mortality.
The mean age of the subjects (n=220) was 67 years, and 74% were male. Hypertension was present in 61% of participants; 28% had diabetes. Overall, cardiovascular comorbidities were not very prevalent. For many patients, CS was the first presentation of heart disease. About one-third (35%) of subjects had a prior history of coronary artery disease; 25% of subjects had a prior myocardial infarction (MI). The mean SBP at presentation was 78 mm Hg, and the mean ejection fraction was 33%. Clinical signs of hypoperfusion included cold periphery (95%), lactate levels above 2 mmol/L (70%), confusion or altered mental status (68%), and oliguria (55%). Acute coronary syndrome (ACS) was the cause of CS in 81% of subjects. Other etiologies included severe low-output heart failure (11% of subjects), valvular dysfunction (5%), myocarditis (2%), and apical ballooning syndrome (2%).
A coronary angiogram was performed in 81% of subjects (92% of those with ACS). The use of vasopressors (mostly norepinephrine) was common (85% of subjects). Inotropes were used for 65% of subjects. An intra-aortic balloon pump was used in 64% of patients. In-hospital mortality was 37% (n=81).
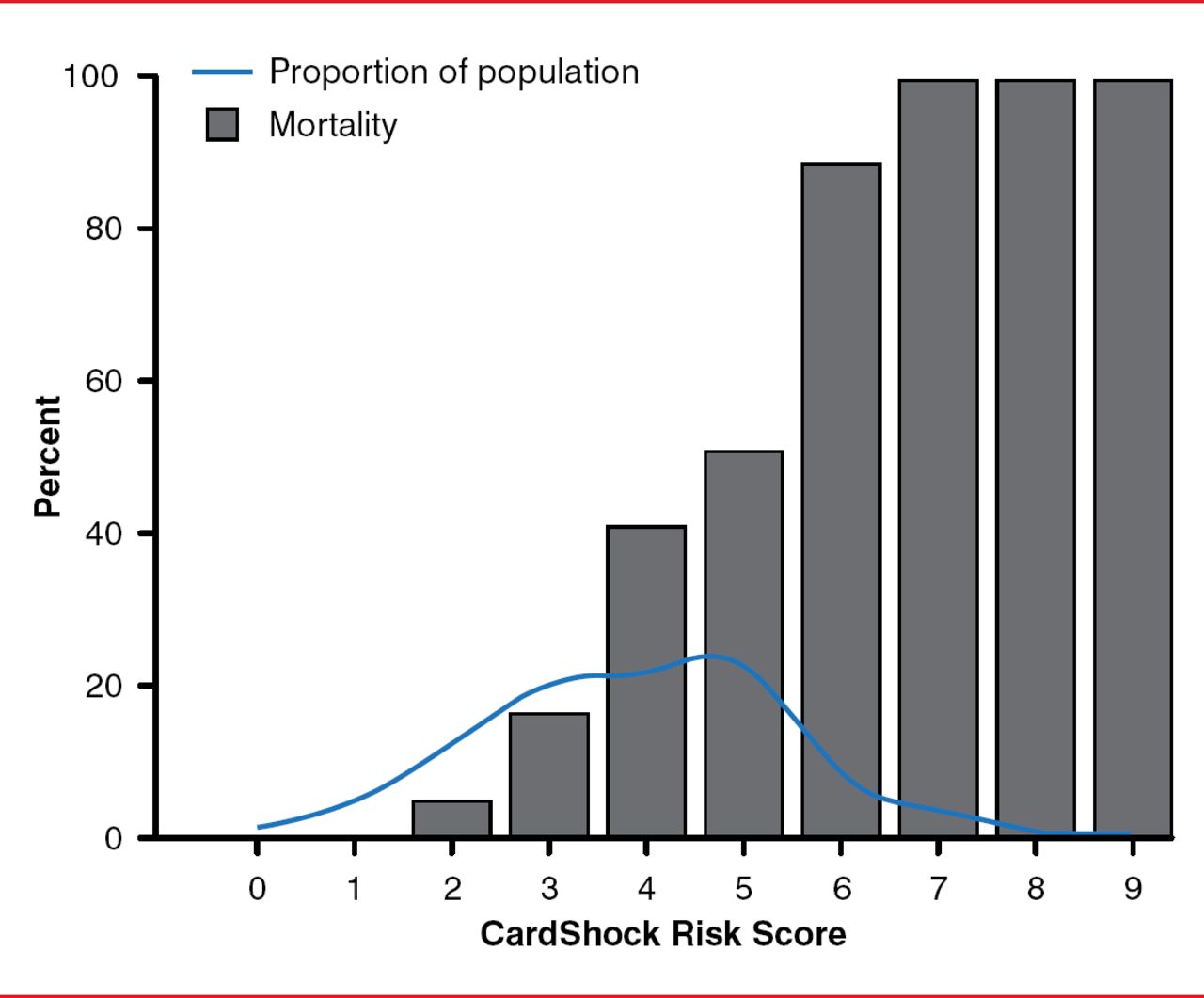
A stepwise analysis was conducted, and 7 predictors of in-hospital mortality for patients with CS were identified. Each variable was assigned a score of 1 or 2 based on their relative contribution to mortality, with a maximum score of 9 (Table 1). The distribution of patients by risk score is shown in Figure 1.
Predictors of In-Hospital Mortality. CardShock Score
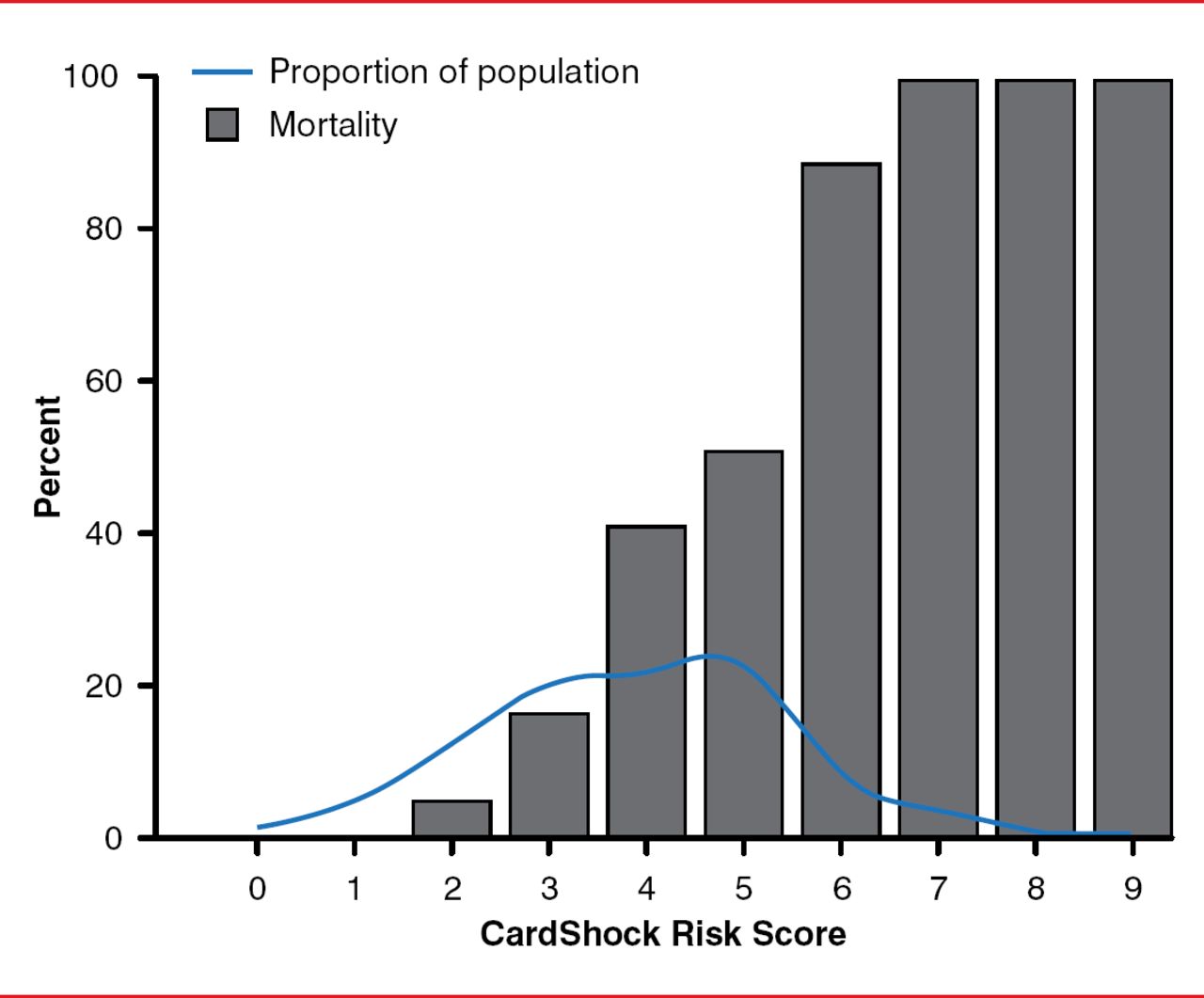
CardShock Score: Mortality Distribution by Score
Reproduced with permission from J Lassus, MD, PhD.
The investigators compared the CardShock scoring system with the Sleeper score, which was developed in the Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock Trial Registry [SHOCK] to predict mortality in CS complicating MI [Sleeper LA et al. Am Heart J 2010]. Although the predictor variables are similar (eg, age, clinical evidence of hypoperfusion, prior coronary artery bypass graft, and left ventricular function), Dr. Lassus argued that the CardShock score had an advantage of greater simplicity. The area under the receiver operating characteristic score for the CardShock risk score was 0.86 as compared with 0.76 for the Sleeper score when applied to the CardShock cohort.
The in-hospital mortality rate of CS remains very high in the contemporary era, and there is utility in the early identification of those patients at highest risk of death. Using clinical variables readily available on presentation, the CardShock risk score is able to identify those with low- (0 to 2 points), medium- (3 to 5 points), and high-risk (6 to 9 points) of short-term mortality with reasonable discrimination.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.