

Summary
This article discusses the significance of exacerbations and rehospitalizations in chronic obstructive pulmonary disease (COPD) in contributing to the high mortality rate associated with the disease. Recent data were also highlighted, showing that human rhinovirus (HRV) infection is common in frequent exacerbators, and how secondary bacterial infection may represent a mechanism for exacerbation recurrence and therefore a potential target for novel therapies.
- Chronic Obstructive Pulmonary Disease
- Pulmonary & Critical Care
- Chronic Obstructive Pulmonary Disease
Gerard. J. Criner, MD, Temple University School of Medicine, Philadelphia, Pennsylvania, USA, launched a series of sessions that discussed the significance of exacerbations and rehospitalizations in chronic obstructive pulmonary disease (COPD) in contributing to the high mortality rate associated with the disease. Recent data were also highlighted, showing that human rhinovirus (HRV) infection is common in frequent exacerbators, and how secondary bacterial infection may represent a mechanism for exacerbation recurrence and therefore a potential target for novel therapies.
COPD is a major cause of morbidity and mortality worldwide, and it results in a significant economic and social burden. It is the third leading cause of death in the United States and the third leading cause of rehospitalization within 30 days of discharge. Dr. Criner, however, emphasized that although ∼12.7 million adults in the United States carry the diagnosis, a total of ∼24 million have impaired lung function, suggesting significant underdiagnosis.
THE IMPACT OF EXACERBATIONS AND REHOSPITALIZATIONS ON CHRONIC OBSTRUCTIVE PULMONARY DISEASE
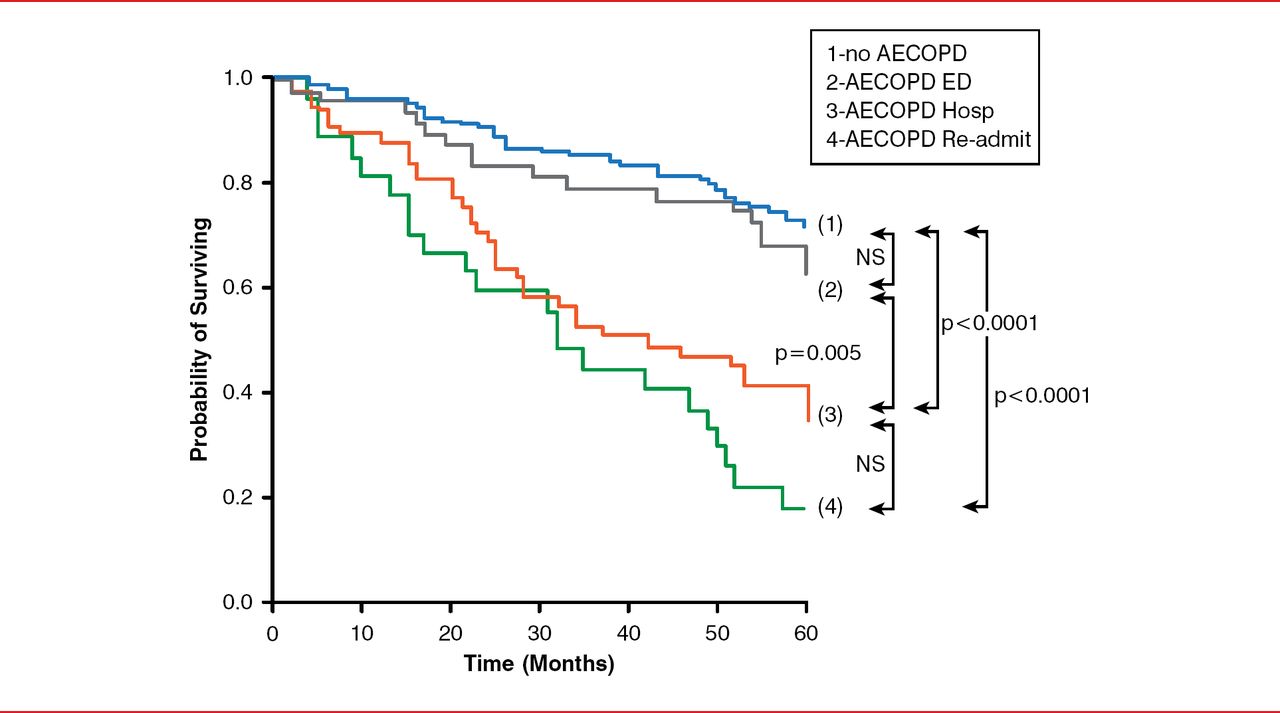
According to Dr. Criner, in 2010, COPD was responsible for the deaths of >134,000 people and accounted for an estimated $49.9 billion in health care costs—approximately 75% of which were related to exacerbation episodes. Acute exacerbations of COPD (AECOPD) that require hospitalization not only account for the majority of these costs but also represent an independent indicator of a poor prognosis in patients with COPD, with the greatest mortality risk being in patients having ≥3 AECOPD (HR, 4.13; 95% CI, 1.80 to 9.41; Figure 1) [Soler-Cataluna JJ et al. Thorax 2005].
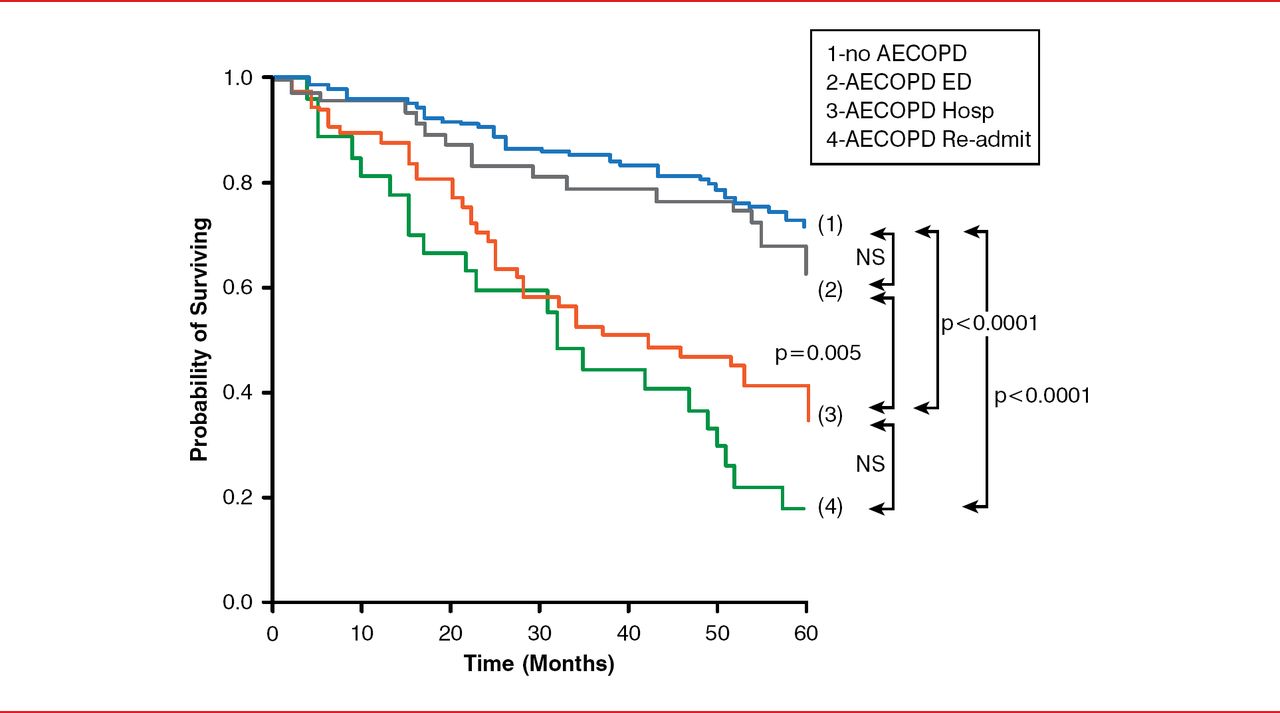
Severity of AECOPD and Mortality Risk
NS=statistically nonsignificant; AECOPD=acute exacerbations of chronic obstructive pulmonary disease; 1-no AECOPD=no AECOPD; 2-AECOPD
ED=AECOPD requiring emergency department visit; 3-AECOPD Hosp=patients with AECOPD requiring one hospitalization; 4-AECOPD Re=admit=patients with AECOPD requiring rehospitalizations.
Reproduced from Soler-Cataluna JJ et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005; 60(11):925–931. With permission from the BMJ Publishing Group.
RISK FACTORS FOR AECOPD
Dr. Criner discussed some of the various factors known to predispose patients with COPD to hospitalization and then readmission, including, for example, increasing age, female sex, reduced physical activity, and race. Evidence of chronic bronchitis is also a significant risk factor, not only for frequency of exacerbation but also for severe exacerbations that require hospitalization. A history of frequent exacerbation and hospitalization is a strong clinical predictor of who is going to be hospitalized in the future.
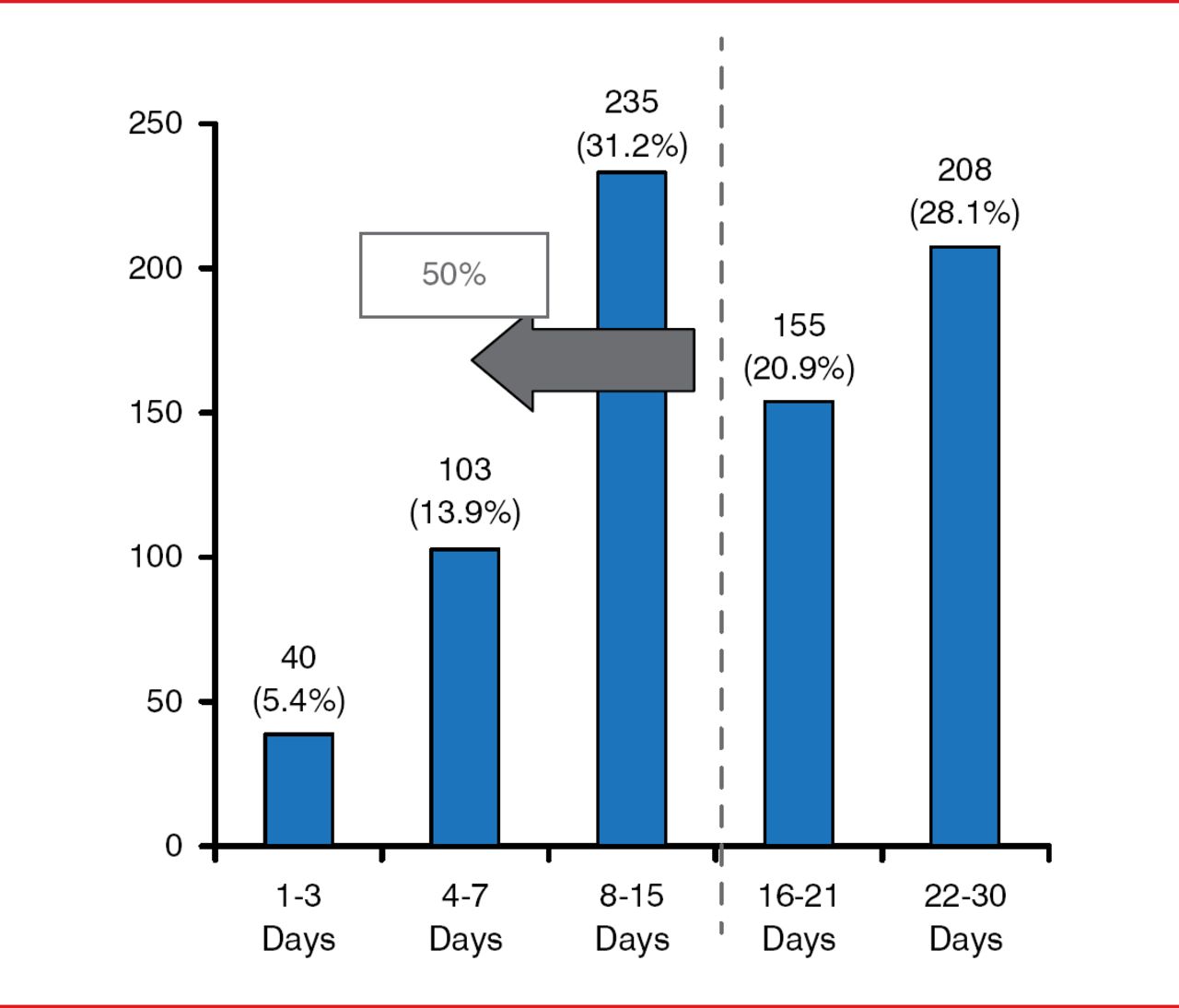
In the United States, 1 in 11 patients aged 40 to 64 years hospitalized with COPD is readmitted within 30 days of discharge, half of whom are readmitted within the first 2 weeks (Figure 2). Patient factors (history of heart failure, lung cancer, osteoporosis, and depression), provider factors (no prescription of statins within 12 months of the index hospitalization, and no prescription of short-acting bronchodilator, oral steroid, and antibiotic on discharge), and system factors (length of stay <2 or >5 days, and no follow-up visit in an outpatient setting within 30 days of discharge) have been shown to be associated with these early rehospitalizations [Sharif R et al. Annals ATS 2014].
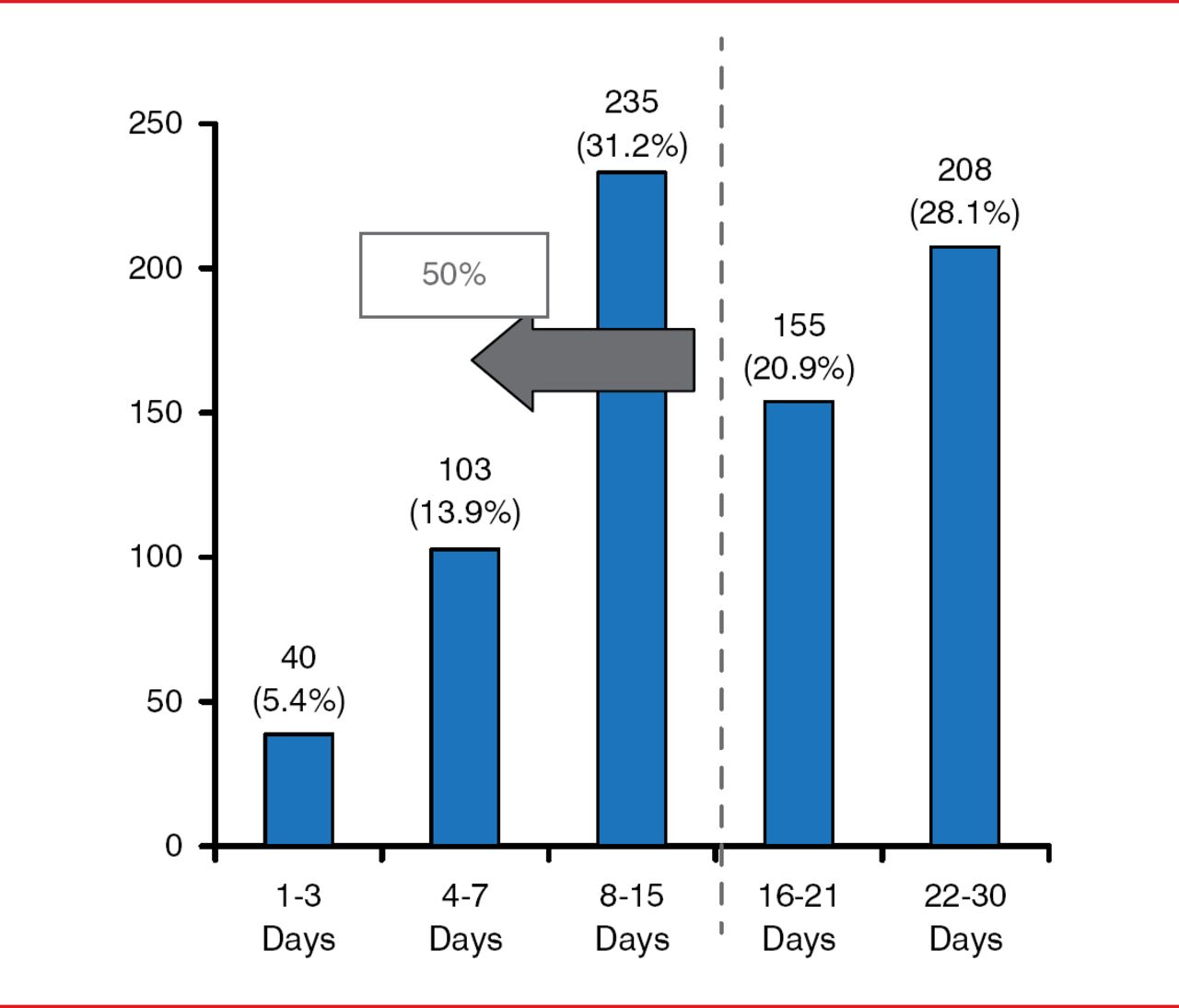
30-Day Rehospitalization Rate in Patients With Chronic Obstructive Pulmonary Disease, Aged 40–64 Years
Reproduced from Sharif R et al. No access predictors of early readmission among patients 40 to 64 years of age hospitalized for chronic obstructive pulmonary disease. Annals ATS 2014;11:685–694. With permission from the American Thoracic Society.
RADIOGRAPHIC MARKERS AND EXACERBATION RISK
With increasing recognition of AECOPD as a major burden to both patients with COPD and society in general, MeiLan K. Han, MD, MS, University of Michigan Health System, Ann Arbor, Michigan, USA, addressed the potential role of quantitative imaging in helping physicians to manage AECOPD.
Dr. Han noted that the use of quantitative computed tomography (QCT) holds value in COPD beyond just its ability to identify structural abnormalities in the lungs. Pulmonary vascular abnormalities may also occur relatively early in the course of COPD and have clinical significance. In recent years, research has shown that QCT can provide a significant amount of information about the vasculature that may be used to identify patients at risk of AECOPD. For example, in a study to examine the relationship between exacerbations and a QCT measure of pulmonary vascular disease, measurements were taken of the diameters of the pulmonary artery (PA) and the aorta (A).
PA enlargement, as defined by a PA:A ratio of >1, not only was independently associated with AECOPD but also identified a subpopulation at high risk for hospitalization for these events [Wells JM et al. N Engl J Med 2012]. The use of QCT in identifying COPD phenotypes is therefore now increasingly appreciated, not only to establish prognosis but also to identify patients with common underlying disease mechanisms that may ultimately require specific therapies.
HOW CLINICAL HISTORY CAN PREDICT EXACERBATION RISK
John. R. Hurst, MBChB, PhD, University College London Medical School, London, United Kingdom, shared data from the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints observational study [ECLIPSE] that recruited >2000 patients aged 40 to 75 years who were prospectively followed for 3 years [Hurst JR et al. N Engl J Med 2010]. The results of this study showed that exacerbation frequency and severity increased with increased COPD severity. In the first year of follow-up, exacerbation rates were 0.85 per person in patients with Global Initiative for Chronic Obstructive Lung Disease (GOLD) Stage 2 COPD, 1.34 for patients with Stage 3, and 2.00 for patients with Stage 4. Frequent exacerbations occurred in 22% of patients with Stage 2 disease, 33% with Stage 3, and 47% with Stage 4.
The severity of the underlying COPD was not the only significant factor, however. Among all GOLD stages of disease, the data showed that as COPD severity increases, the most important predictor of frequent exacerbations is a history of exacerbations. Other factors that independently predicted exacerbation risk were poorer quality of life, a history of gastroesophageal reflux, and increased peripheral white blood cell count. Importantly, the data also showed that exacerbation frequency was relatively stable during the 3 years of the study and could be predicted based on the patients' recall of previous treated exacerbations in the year prior to the study.
Patients in the study who were frequent exacerbators in Years 1 and 2 had a 71% chance of being a frequent exacerbator in Year 3, whereas, of those who did not have frequent exacerbations in Years 1 and 2, 74% remained exacerbation free in Year 3. Although Prof. Hurst suggested that this indicates that there is a group of individuals that is intrinsically susceptible and also a group intrinsically resistant to exacerbations, he stressed that, even if a patient is inherently susceptible, a sufficient trigger is still required to result in an exacerbation.
Exacerbation frequency is important clinically with respect to targeting therapy and also for the recruitment of patients into clinical trials. The London COPD Cohort study has shown that patients are reliable at recording the actual number of exacerbations they have in a year, allowing them to be stratified into frequent or infrequent exacerbator groups [Quint JK et al. ERJ 2010]. Patient estimates of their exacerbation number during the year prior to study entry were compared with the number recorded on diary cards collected during the first year of study. There was no difference between the exacerbation number recalled prior to the study and the number detected during Year 1 (median, 2.0 [interquartile range, 1.0 to 4.0] and 2.0 [IQR, 1.0 to 4.0]; expected agreement, 76.4%; agreement, 84.6%; κ=0.3469); in addition, there was no difference between the number recalled by patients and the number recorded on diary cards during the same 1-year period (median, 2.0 [IQR, 1.0 to 4.0] for both groups; expected agreement, 74.9%; actual agreement, 93.3%; κ=0.6146).
TREATMENT OF AECOPD
Early detection and prompt treatment of COPD exacerbations are essential to ensure optimal patient outcomes and to reduce the health and economic burdens of COPD. Implementing prevention measures in patients at risk is therefore a major goal in the management of this disease. Reaching a diagnosis of COPD is therefore essential for its appropriate management. Although this can be established by a combination of a medical history and spirometry results, Bartolome R. Celli, MD, Brigham and Women's Hospital, Harvard University, Boston, Massachusetts, USA, noted that ∼70% of patients admitted with a diagnosis of COPD have never even undergone spirometry. Although numerous treatment options are available for AECOPD, Dr. Celli emphasized the importance of reaching a diagnosis of COPD before initiating any therapy.
Even though inhaled corticosteroids (ICSs) have been widely used for the treatment of AECOPD, their effectiveness remains somewhat controversial. Despite their reduction of the inflammation associated with COPD exacerbations, Dr. Celli stressed that ICSs should not be administered alone and that they perform better in combination with a long-acting beta agonist (LABA). In one study, combination inhalers reduced the frequency of exacerbations compared with their LABA component alone, from, for example, an average of one exacerbation per year with a LABA alone to an average of 0.76 exacerbations per year on combined inhalers; however, there was evidence of an overall increased risk of pneumonia, from about 3 per 100 people per year on LABA to 4 per 100 per year on combined inhalers [Nannini L et al. Cochrane Database Syst Rev 2007]. In addition, in a recent Cochrane Database review, considering a baseline risk of death of 15.2% from the placebo arm of the TOwards a Revolution in COPD Health trial [TORCH], to prevent 1 extra death, the 3-year number-needed-to-treat for an additional beneficial outcome (NNTB) with fluticasone–salmeterol was 42 (95% CI, 24 to 775) [Nannini LJ et al. Cochrane Database Syst Rev 2013].
The nonsteroidal anti-inflammatory drug roflumilast also has a role to play as a secondary drug in treating AECOPD, proving effective at further preventing exacerbations when added to LABA or long-acting muscarinic antagonists (LAMAs). It is also considered more useful in patients with cough and sputum production. In a pooled analysis of data from 2 placebo-controlled, double-blind, multicenter trials in patients with COPD, compared with placebo, prebronchodilator forced expiratory volume in 1 second increased by 48 mL with roflumilast (p<0.0001) [Calverley PMA et al. Lancet 2009].
Long-acting bronchodilator therapy is having a significant impact in preventing COPD exacerbations, explained Antonio Anzueto, MD, University of Texas, San Antonio, Texas, USA [Donohue JF, Jones PW. Int J Chron Obstruct Pulmon Dis 2011]. This reduced rate of exacerbations subsequently translates to a reduced rate of hospitalization, as demonstrated by the results from a 4-year trial of tiotropium in COPD, in which tiotropium was associated with a significant reduction in the probability of exacerbation (HR, 0.86; 95% CI, 0.81 to 0.91) and time to first hospitalization for an exacerbation (HR, 0.86; 95% CI, 0.78 to 0.95) [Tashkin DP et al. N Engl J Med 2008].
HOSPITAL-AT-HOME SCHEMES: EFFICACY AND IMPLEMENTATION
Hospital-at-home schemes have been recently adopted as a method of service delivery for the management of AECOPD. Jadwiga A. Wedzicha, MD, PhD, National Heart and Lung Institute, Imperial College London, London, United Kingdom, discussed data of moderate quality suggesting their ability to reduce rehospitalization in this patient population (risk ratio [RR], 0.76; 95% CI, 0.59 to 0.99; p=0.04), as well as showing a trend toward reduced the mortality rate compared with conventional inpatient hospitalization treatment (RR, 0.65; 95% CI, 0.40 to 1.04; p=0.07) [Jeppesen E et al. Cochrane Database of Systematic Reviews 2012].
In explaining the significance of why so many patients are rehospitalized at ∼2 weeks, Prof. Wedzicha shared data from a recent study that suggest viral infection and secondary bacterial infection as triggers of AECOPD [George SN et al. ERJ 2014]. Human rhinovirus (HRV) prevalence and load increased at the time of AECOPD and then resolved during recovery. HRV load was higher in patients with cold symptoms (p=0.046) or sore throats (p=0.006) compared with those without. By Day 14, 73% of bacterium-negative but HRV-positive AECOPD were bacterium-positive. Patients in whom HRV was detected at exacerbation had a higher exacerbation frequency (3.01; IQR, 2.02 to 5.30) per year compared with HRV-negative patients (2.51; IQR, 2.00 to 3.51; p=0.038). The fact that secondary bacterial infection is common after HRV infection therefore provides a possible mechanism for exacerbation recurrence, as well as a potential target for novel therapies. Prompt diagnosis during follow-up is therefore essential, and patients who suffer AECOPD should be seen again at around the 2-week mark, she concluded.
THE ROLE OF PATIENT EDUCATION IN DECREASING CHRONIC OBSTRUCTIVE PULMONARY DISEASE REHOSPITALIZATION
The symptoms of COPD gradually worsen throughout the years, leading to reduced health-related quality of life. Yet, according to Jean Bourbeau, MD, RECRU, Montreal Chest Institute, McGill University, Montreal, Canada, although these patients often know a lot about what they should be doing to manage their COPD, they often fail to adopt these important behaviors.
Study data have shown that self-management interventions and/or integrated disease management (IDM) in patients with COPD can be associated with a reduction in COPD hospital admissions, but not all-cause hospital admissions [Zwerink M et al. Cochrane Database of Systematic Reviews 2014]. Self-management training is therefore becoming increasingly important in the treatment of COPD because it teaches patients the skills and behaviors needed to successfully manage their disease. Because of heterogeneity among the trials analyzed, however, it is difficult to formulate clear recommendations regarding the most effective form and content of self-management in COPD, and there remains insufficient evidence to recommend education alone to prevent rehospitalizations from AECOPD, concluded Dr. Bourbeau.
The editors would like to thank the many members of the 2014 American Thoracic Society presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
- Article
- Summary
- THE IMPACT OF EXACERBATIONS AND REHOSPITALIZATIONS ON CHRONIC OBSTRUCTIVE PULMONARY DISEASE
- RISK FACTORS FOR AECOPD
- RADIOGRAPHIC MARKERS AND EXACERBATION RISK
- HOW CLINICAL HISTORY CAN PREDICT EXACERBATION RISK
- TREATMENT OF AECOPD
- HOSPITAL-AT-HOME SCHEMES: EFFICACY AND IMPLEMENTATION
- THE ROLE OF PATIENT EDUCATION IN DECREASING CHRONIC OBSTRUCTIVE PULMONARY DISEASE REHOSPITALIZATION
- Figures & Data
- Info & Metrics
- eLetters
Cited By...
- No citing articles found.