

Summary
The 2013 European Society of Hypertension (ESH)/ European Society of Cardiology (ESC) guidelines for the management of hypertension have recently been released [Mancia G et al. Blood Press 2013; Eur Heart J 2013; J Hypertens 2013]. This article provides an overview of these guidelines.
- Cardiology Guidelines
- Hypertensive Disease
- Cardiology Guidelines
- Exclusive Article - For home page
- Cardiology & Cardiovascular Medicine
- Hypertensive Disease
The 2013 European Society of Hypertension (ESH)/European Society of Cardiology (ESC) guidelines for the management of hypertension have recently been released [Mancia G et al. Blood Press 2013; Eur Heart J 2013; J Hypertens 2013]. Josep Redon, MD, PhD, Hospital Clinico, University of Valencia, Valencia, Spain, gave an overview of these guidelines.
Previous versions of the guidelines were issued in 2003 [ESH–ESC Guidelines Committee. J Hypertens 2003] and 2007 [Mancia G et al. J Hypertens 2007], and a reappraisal of the guidelines was issued by the ESH in 2009 [Mancia G et al. J Hypertens 2009]. Prof. Redon said that for the development of the 2013 guidelines, over an 18-month period, task force members sought to revise previous recommendations where necessary and provide recommendations based on appropriately conducted studies selected from a thorough review of the literature. Data from randomized trials and their meta-analyses were given the highest priority, but results from observational and other studies of appropriate scientific caliber were also considered, especially those with a diagnostic focus. In addition to internal reviewers, the content was reviewed twice by a panel of 40 European experts. For the first time, evidence and recommendations were also graded (Table 1).
Evidence Grade and Definitions
The 2013 guidelines include sections on epidemiological aspects, diagnostic evaluation, treatment approaches and strategies, treatment of associated risk factors, follow-up, improvement of blood pressure (BP) control in hypertension, hypertension disease management, and gaps in evidence and need for future trials.
Robert H. Fagard, MD, PhD, Katholieke Universiteit Leuven, Leuven, Belgium, provided a summary of the 2013 ESH/ESC guideline recommendations regarding diagnosis and lifestyle changes in patients with hypertension. To put the guidelines in perspective, Dr. Fagard gave a brief overview of the epidemiology of hypertension in Europe. The prevalence of hypertension in Europe is approximately 30% to 45% [Pereira M et al. J Hypertens 2009]. There are notable differences in the average BP levels across countries, making it difficult to compare results among countries and longitudinally, said Prof. Fagard. For this reason, it has been suggested that stroke mortality be used as a surrogate marker of hypertension status [Cooper RS. Hypertension 2007]. Based on statistics from the World Health Organization, stroke mortality has decreased in western European countries but increased in eastern European countries [Redon J et al. Eur Heart J 2011].
Per the 2013 ESH/ESC guidelines, total cardiovascular (CV) risk stratification using the Systemic Coronary Risk Evaluation (SCORE) model is strongly recommended as a minimal requirement for asymptomatic hypertensive patients with no evidence of CV disease, chronic kidney disease, or diabetes. Furthermore, clinicians are advised to look for evidence of organ damage, especially in patients with moderate risk, as there is evidence that asymptomatic organ damage predicts CV death independently of SCORE. Treatment strategies should be based on the initial level of total CV risk. While total CV risk stratification is traditionally based on BP readings taken in the office, the new guideline has a provision for considering out-of-office BP in the risk stratification model to elucidate which patients may have white-coat (or isolated office) hypertension or masked (isolated ambulatory) hypertension.
The initial assessment of patients with hypertension should confirm the diagnosis of hypertension, detect causes of secondary hypertension, and evaluate CV risk factors, asymptomatic organ damage, and concomitant medical conditions. Prof. Fagard reviewed the best practices for BP measurement. BP should preferably be measured at the upper arm, with the cuff adjusted to arm circumference. After the patient has sat for 3 to 5 minutes, ≥2 BP measurements should be taken 1 to 2 minutes apart. Additional measurements should be obtained if the first 2 are very different. Heart rate should be determined after the second BP reading. In cases where orthostatic hypotension is suspected, such as in the elderly and patients with diabetes, BP should be measured 1 and 3 minutes after standing.
Patients diagnosed with hypertension can benefit from lifestyle modifications (Table 2). In addition to lowering BP, lifestyle changes help control other CV risk factors and medical conditions.
Recommendations on Lifestyle Changes
Giusseppe Mancia, MD, Centro di Fisiologia Clinica e Ipertensione, Milan, Italy, reviewed drug treatment recommendations from the 2013 ESH/ESC guidelines.
Based on available evidence, recommended target BP is a systolic BP <140 mm Hg and a diastolic BP <90 mm Hg, regardless of risk. Additionally, task force members decided not to rank antihypertensive drugs for the following reasons: the primary mechanism associated with the benefit of antihypertensive treatment is the lowering of BP per se; the effects on cause-specific outcomes are very similar between drugs; patient outcomes are unpredictable; and each drug class has its advantages and disadvantages. Instead, the task force has provided recommendations based on trial data in specific conditions to help clinicians select the most appropriate drug, taking into account risk factors and adverse events.
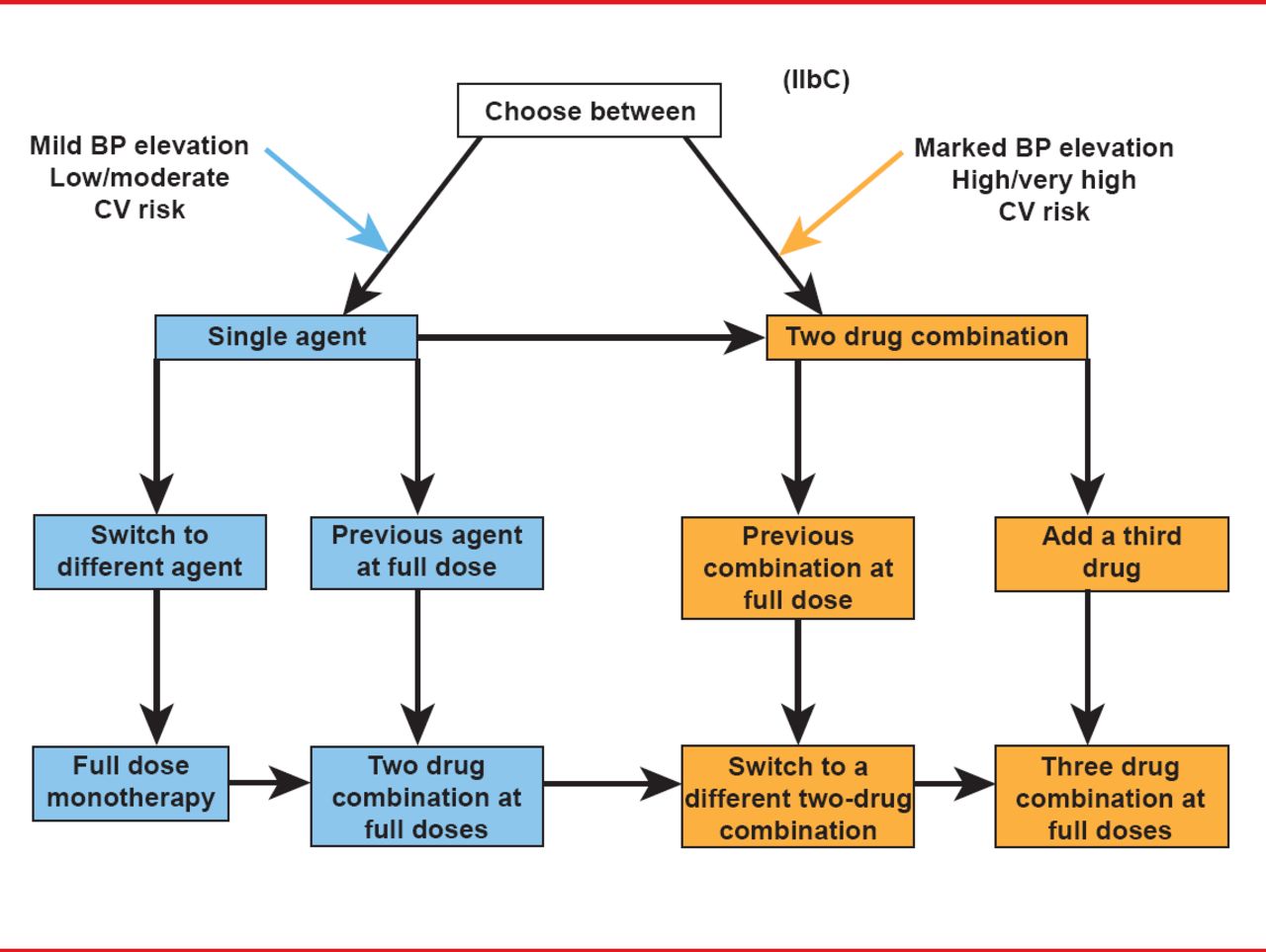
In terms of combination therapy, it remains true that most patients require ≥2 drugs to control BP. Combination therapy is best for patients with high baseline BP or with high risk, and in all cases, moving from a less intensive therapy to a more intensive strategy should be undertaken if the target BP is not met. A schematic of mono versus combination therapy strategies is illustrated in Figure 1.
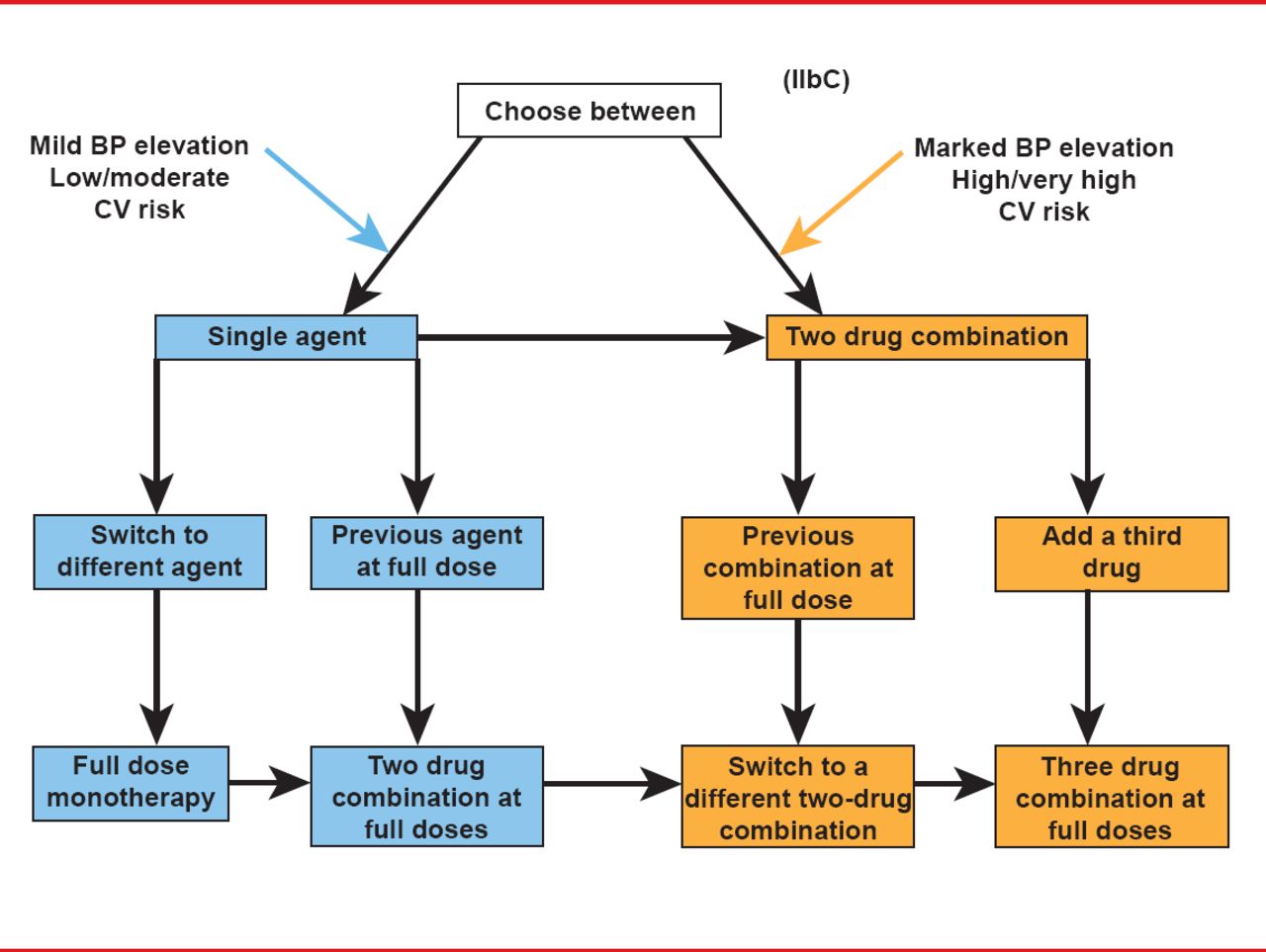
Mono Versus Combination Therapy to Achieve Target Blood Pressure
BP=blood pressure; CV=cardiovascular.
In his closing remarks, Prof. Mancia encouraged clinicians to read the section on “gaps in evidence and the need for future trials” that is listed in the guidelines and emphasized the need for more research in the area of hypertension.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.