

Summary
This article discusses the epidemiology of ST-segment elevation myocardial infarction (STEMI) and cardiogenic shock, and its association with the increasing use of reperfusion therapy, especially primary percutaneous coronary intervention (PCI). Specific topics include reperfusion therapy, cardiac assist devices, shock after resuscitated cardiac arrest, and the use of PCI in refractory in- or out-of-hospital cardiac arrest.
- Interventional Techniques & Devices
- Myocardial Infarction
- Cardiology & Cardiovascular Medicine
- Interventional Techniques & Devices
- Myocardial Infarction
Christian Spaulding, MD, European Hospital Georges Pompidou and INSERM U 970, Paris, France, discussed the epidemiology of ST-segment elevation myocardial infarction (STEMI) and cardiogenic shock (CS), and its association with the increasing use of reperfusion therapy, especially primary percutaneous coronary intervention (PCI).
IMPROVED USE OF REPERFUSION THERAPY
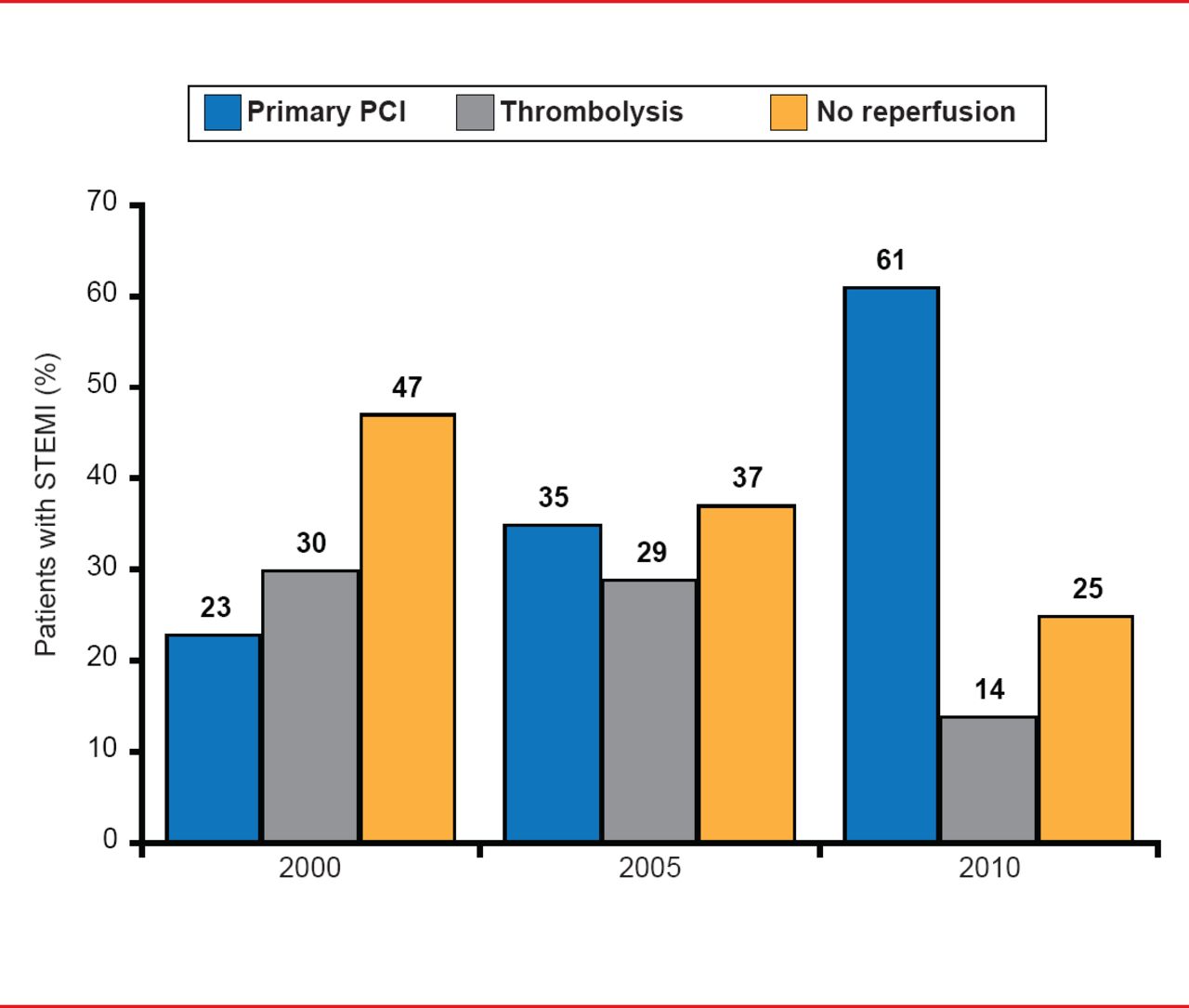
Evaluation of French survey data showed an improved use of reperfusion therapy from 1995 to 2010, associated with an increased use of primary PCI and decreased use of thrombolysis from 2000 to 2010 (Figure 1). During the decade, the mortality rate 30 days after STEMI declined by ∼9% absolute [Puymirat E et al. JAMA 2012].
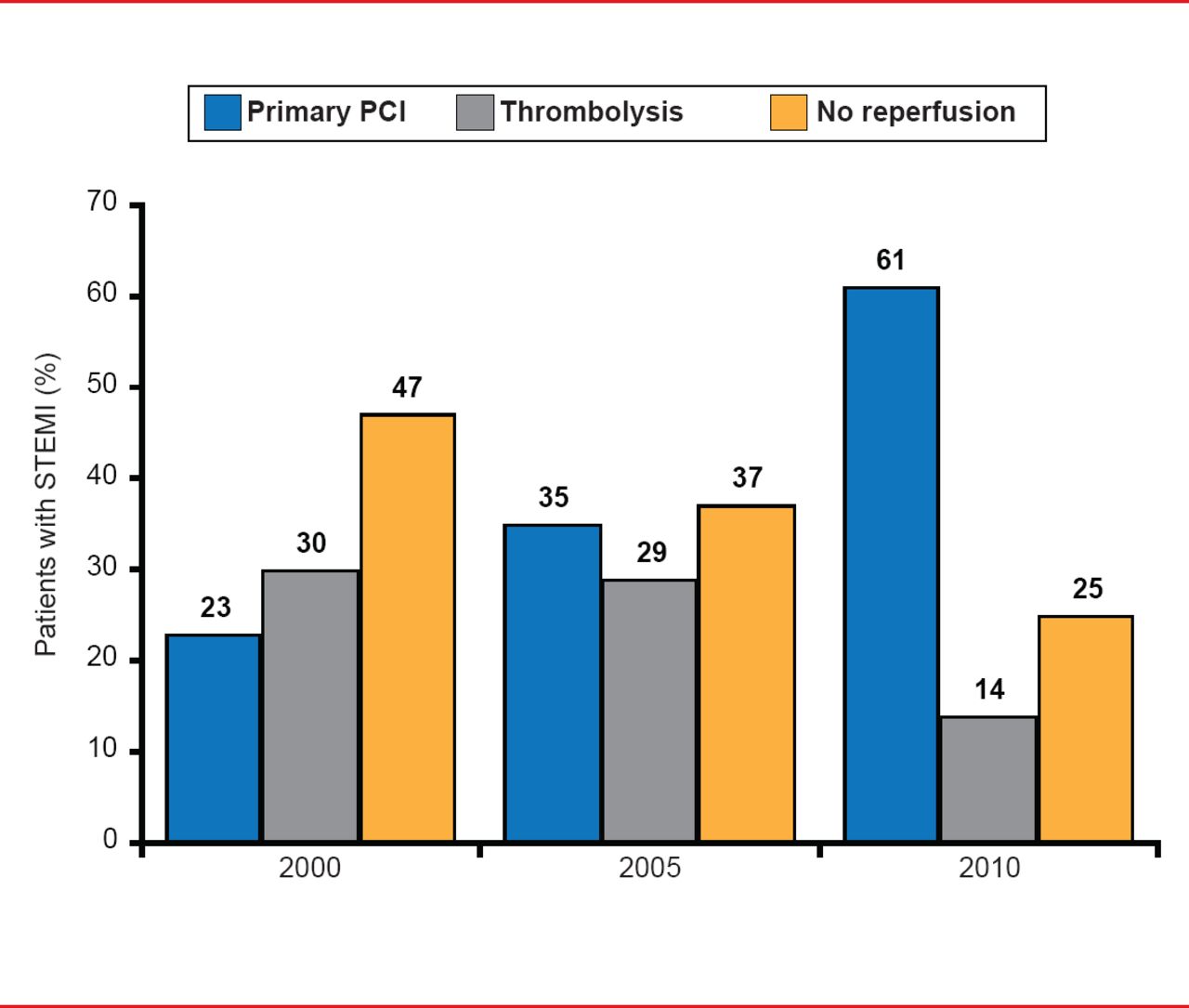
Changes in Use of Reperfusion Therapy, PCI, and Thrombolysis Over Time
Reproduced with permission from C Spaulding, MD.
Prof. Spaulding discussed key data from three French nationwide registries [Aissaoui N et al. Eur Heart J 2012] conducted between 1995 and 2005, comparing mortality in patients with acute myocardial infarction (AMI) with versus without CS. The key findings were 1) the incidence of CS decreased over time (6.9% in 1995; 5.7% in 2005; p=0.07); 2) 30-day mortality was more than 10-fold higher in CS patients (60.9% vs 5.2%); and 3) mortality decreased both among patients with (70% to 51%; p=0.003) and without CS (8.7% to 3.6%; p<0.001). Correspondingly, the use of PCI increased from 20% to 50% (p<0.001), and was associated with decreased mortality (OR, 0.38; 95% CI, 0.24 to 0.58; p<0.001).
Of patients enrolled in the Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock trial [SHOCK], 302 had AMI complicated by CS. Compared with initial medical stabilization, early revascularization resulted in a 13.2% absolute and 67% relative improvement in 6-year survival, reinforcing the need to rapidly identify patients who are candidates for early revascularization [Hochman JS et al. JAMA 2006].
CARDIAC ASSIST DEVICES
Despite the lack of clear guidelines for the timing and choice of cardiac assist devices (CADs), numerous options are available:
Intraaortic Balloon Pump (IABP): Although it was considered a Class I treatment for CS complicating AMI, clinical data are lacking to confirm this. In one recent trial, intraaortic balloon counterpulsation did not significantly reduce 30-day mortality in such patients [Thiele H et al. N Engl J Med 2012] although this lack of benefit may, in part, be explained by the use of IABP in 10% of the patients in the control arm.
Extracorporeal membrane oxygenator/extracorporeal life support (ECMO/ECLS): ECLS has shown encouraging outcomes in cardiac arrest (CA), and early ECMO-assisted primary PCI improves 30-day outcomes in STEMI complicated with CS.
Between 2002 and 2009, 1650 patients with acute STEMI underwent primary PCI. Of these, 13.3% had CS and 46 patients were treated with ECMO. The outcomes of the patients treated in an era in which ECMO was available was compared with historical controls of patients who presented between 1993 and 2002 with STEMI complicated by CS who underwent primary PCI prior to the availability of ECMO. The incidence of profound shock was similar in both groups (21.7% vs 21.0%; p>0.5); however, in patients treated in the ECMO era, the mortality of patients with profound shock and total 30-day mortality were lower (all p<0.04), and hospital survival time was increased (p=0.0005) [Sheu JJ et al. Crit Care Med 2010].
ECMO for temporary circulatory support is sometimes the only option for patients with refractory CS (RCS), but is typically only available in tertiary-care centers. However, a pilot study suggested this as a feasible option even in remote hospitals. Mortality was compared between tertiary and nontertiary care centers in the greater Paris area, and results demonstrated successful transfer of 75 of 87 RCS patients to tertiary care following local ECMO support, and 32 survived to hospital discharge (overall survival rate, 36.8%; 95% CI, 27.4 to 46.2). There was no significant difference in mortality between patients who received ECMO locally or at a tertiary care institution (OR, 1.48; 95% CI, 0.72 to 3.00, p=0.29) [Beurtheret S et al. Eur Heart J 2013].
Impella 2.5: Advantages of the Impella 2.5 system include the ease of percutaneous insertion, its user-friendly console, and trends toward improved outcomes compared with IABP-support.
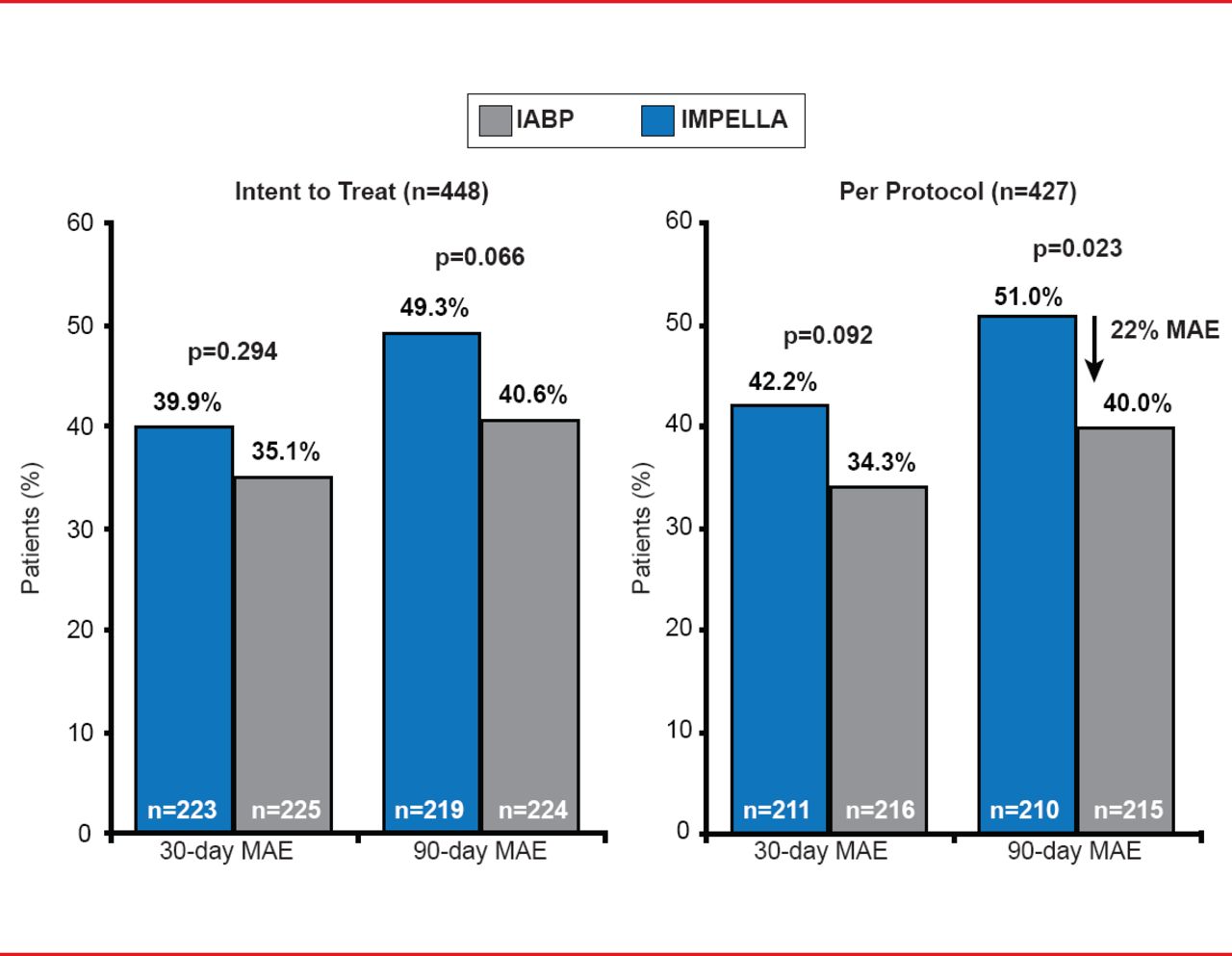
The PROTECT II trial was performed in stable patients undergoing high-risk PCI and compared the Impella system with an IABP. The with a primary endpoint of 30-day incidence of major adverse events (MAEs), which were defined as all-cause death, Q-wave or non-Q-wave MI, stroke or transient ischemic attack, any repeat revascularization procedure (PCI or coronary artery bypass graft), need for a cardiac or a vascular operation (including a vascular operation for limb ischemia), acute renal insufficiency, severe intraprocedural hypotension requiring therapy, cardiopulmonary resuscitation or ventricular tachycardia requiring cardioversion, aortic insufficiency and angiographic failure of PCI. MAEs at 30 days were not significantly different, but at 90-day follow-up there was a strong trend toward reduced MAEs in the Impella group in the intent-to-treat and per-protocol populations (Figure 2) [O'Neill WW et al. Circulation 2012]. There is limited data on the use of the Impella device in CS. Registries have shown improvement in hemodynamic parameters.
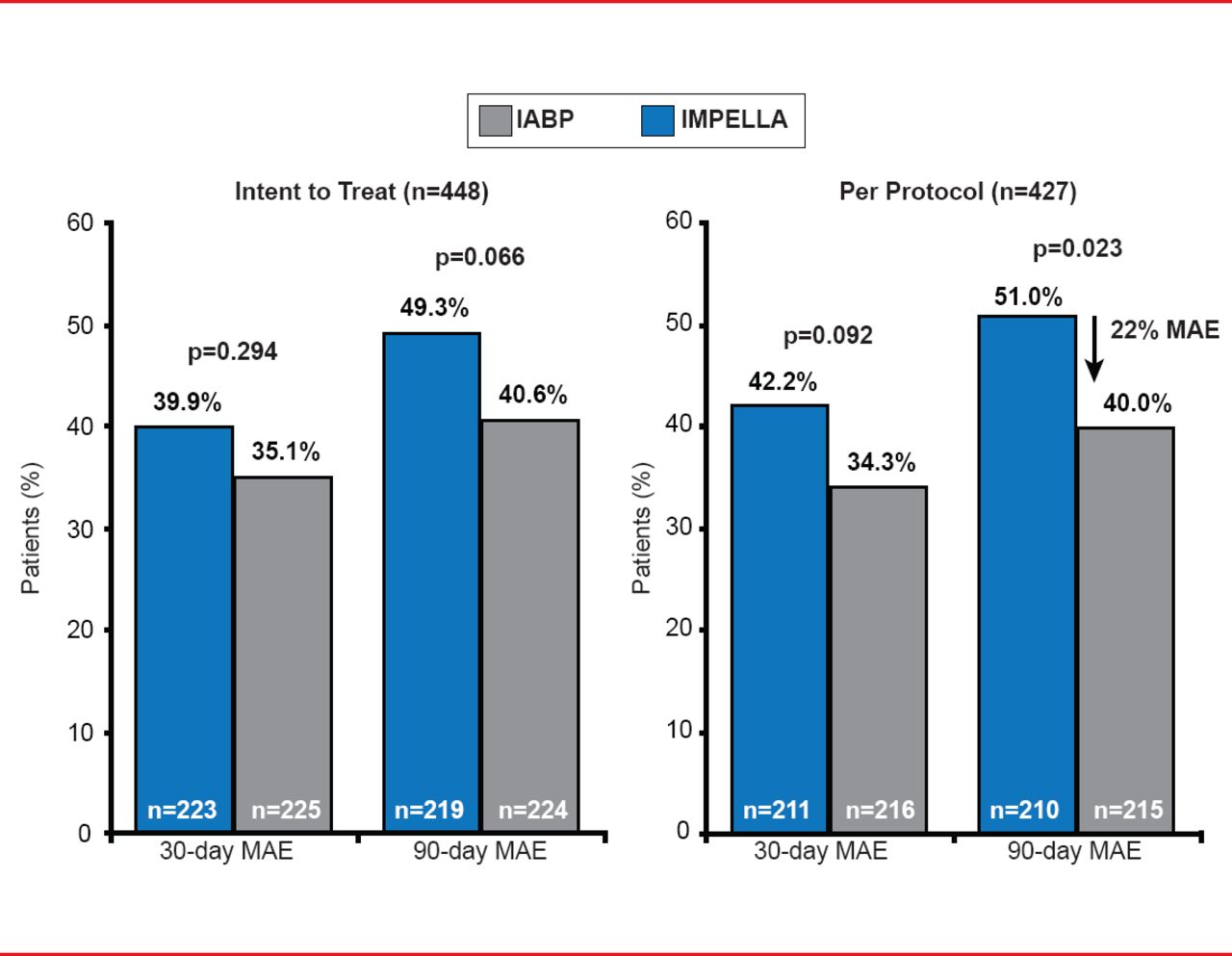
Outcomes of the PROTECT II Trial
Reproduced from O'Neill WW et al. A Prospective, Randomized Clinical Trial of Hemodynamic Support With Impella 2.5 Versus Intra-Aortic Balloon Pump in Patients Undergoing High-Risk Percutaneous Coronary Intervention: The PROTECT II Study. Circulation 2012;126(14):1717–1727. With permission from Lippincott, Williams and Wilkins.
SHOCK AFTER RESUSCITATED CARDIAC ARREST
In patients with resuscitated CA in whom electrocardiography shows ST-segment elevation, the strategy of choice is immediate angiography with a view to primary PCI.
And due to the high potential for coronary occlusions and difficulties in interpreting the electrocardiogram in patients following CA, immediate angiography should be considered when ongoing infarction is suspected.
There is also evidence that survivors of out-of-hospital CA who are comatose have improved neurological outcomes if cooling occurs soon after resuscitation. These patients should considered for prompt initiation of therapeutic hypothermia [Steg PG et al. Eur Heart J 2012].
PCI IN REFRACTORY IN- OR OUT-OF-HOSPITAL CARDIAC ARREST
Studies have shown that survival rate decreases rapidly after 10 minutes of cardiopulmonary resuscitation (CPR), and even more rapidly after 30 minutes.
A 3-year prospective study investigated the use of ECLS as compared with conventional CPR for patients with in-hospital CA of cardiac origin undergoing CPR of >10 minutes. The primary endpoint was survival to hospital discharge. Patients randomized to extracorporeal CPR had a higher survival rate to discharge (p<0.0001), 30-day survival (p=0.003), and 1-year survival as compared with the conventional CPR group (p=0.007) [Chen YS et al. Lancet 2008].
PCI IN REFRACTORY OUT-OF-HOSPITAL CARDIAC ARREST
ECLS has recently been introduced in the treatment of refractory CA. Time from CA to implementation of ECLS is a major prognostic factor for survival. Data from a pilot study has suggested that prehospital ECLS is a safe and feasible option even if the provider is not surgeon. Prehospital ECLS for refractory CA was implemented in seven patients by a team of providers that did not include surgeons. ECLS was started 22 minutes after incision and 57 minutes after onset of advanced cardiovascular life support. One patient survived without sequelae, and brain death resulted in three patients [Lamhaut L et al. Resuscitation 2013].
Prof. Spaulding highlighted that, although CS remains a concern in patients with STEMI, it is rare and usually occurs after admission. He stressed the importance of always considering shock in the management of patients with AMI, and noted that beyond PCI, other factors (such as age, diabetes, past history, coronary artery bypass graft, and AMI) also contribute to the reduced mortality of patients with STEMI.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.