

Summary
Valvular heart disease is not usually regarded as a major public health problem. However, the prevalence of both mitral and aortic valve disease is increasing and is particularly troublesome for individuals aged =75 years [Nkomo VT et al. Lancet 2006]. European Society of Cardiology/European Association for Cardio-Thoracic Surgery Guidelines on the management of valvular heart disease were updated in 2012 [Vahanian A et al. Eur Heart J 2012; Eur J Cardiothorac Surg 2012]. This article discusses some of the major changes that resulted from new evidence regarding risk stratification, diagnostic methods, and therapeutic options.
- Interventional Techniques & Devices Guidelines
- Valvular Disease
- Interventional Techniques & Devices
- Cardiology Guidelines
- Cardiology & Cardiovascular Medicine
- Valvular Disease
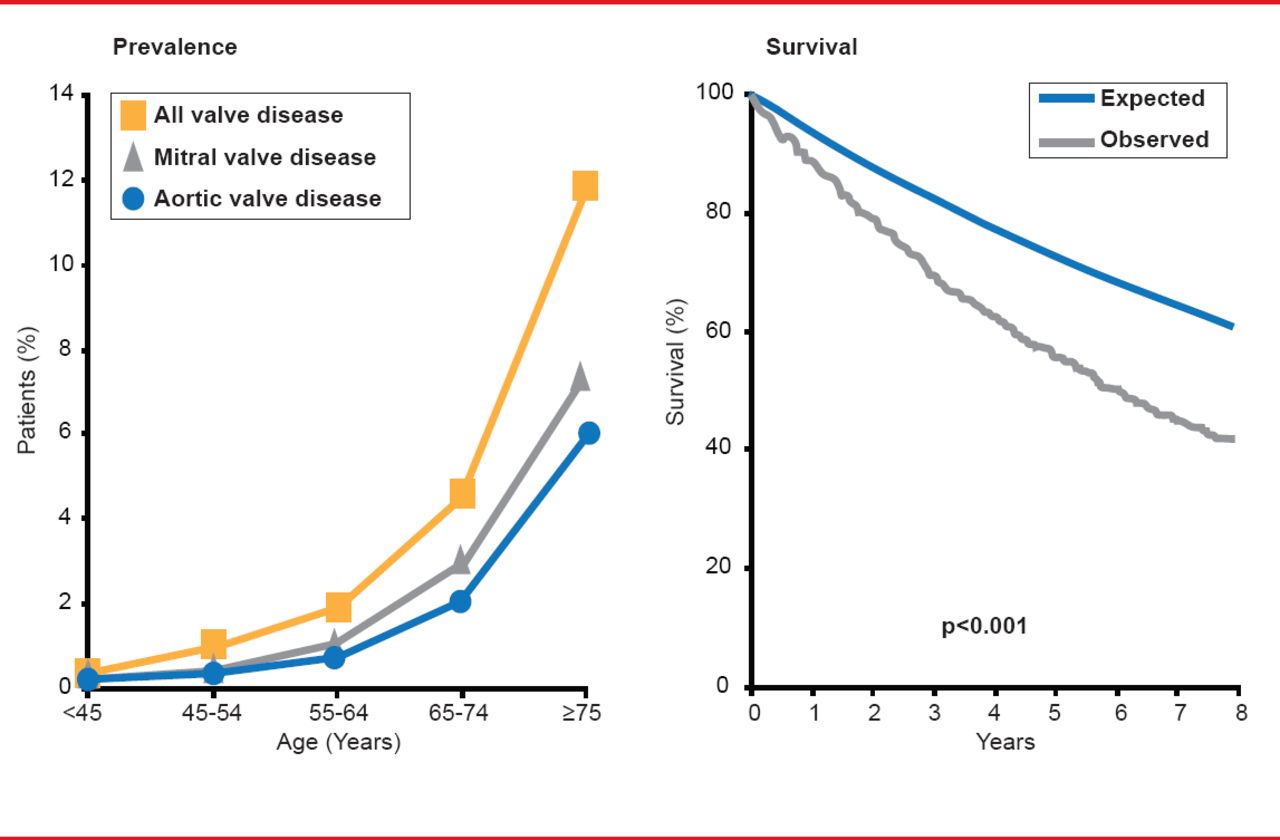
Valvular heart disease is not usually regarded as a major public health problem. However, the prevalence of both mitral and aortic valve disease is increasing and is particularly troublesome for individuals aged ≥75 years (Figure 1) [Nkomo VT et al. Lancet 2006].
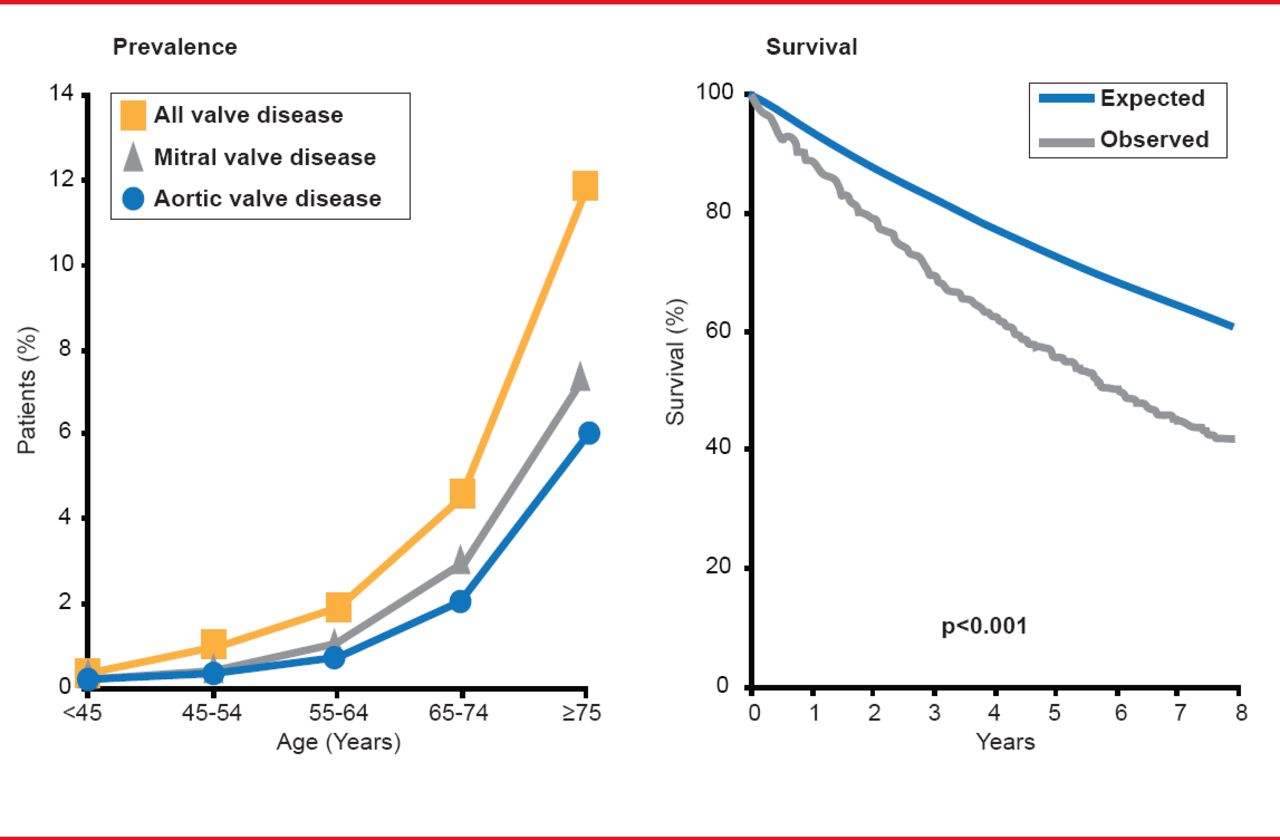
Burden of Valve Disease
Reproduced from Nkomo VE et al. Burden of valvular heart diseases: a population-based study. Lancet 2006;368(9540):1005–1011. With permission from Elsevier.
European Society of Cardiology (ESC)/European Association for Cardio-Thoracic Surgery (EACTS) Guidelines on the management of valvular heart disease were updated in 2012 [Vahanian A et al. Eur Heart J 2012; Eur J Cardiothorac Surg 2012]. Fausto J. Pinto, MD, PhD, University of Lison, Lisbon, Portugal, discussed some of the major changes that resulted from new evidence regarding risk stratification, diagnostic methods, and therapeutic options.
The 2012 guidelines recommend that treatment decisions for patients with valvular heart disease be made by a “heart team” comprised of cardiologists, cardiac surgeons, imaging specialists, anesthesiologists, and others, as appropriate. The decision process should focus on disease severity, patient symptoms, the relationship of the symptoms to valvular disease, life expectancy and quality of life, whether the expected benefits of intervention outweigh the risk, the patient's wishes, and whether local resources are optimal for the planned intervention.
All patients should receive a clinical assessment and echocardiography to confirm diagnosis and to assess severity and prognosis. Exercise testing, stress echocardiography, magnetic resonance imaging, and multislice computed tomography may provide additional useful information. Cardiac catherization to evaluate valve function are necessary only if noninvasive findings are inconsistent with the clinical assessment.
Aortic Regurgitation (Class and Level of Evidence)
Aortic Valve Replacement (Class and Level of Evidence)
Severe Primary MR (Class and Level of Evidence)
PMC in Mitral Stenosis with Valve Area ≤1.5 cm2 (Class and Level of Evidence)
TAVI (Class and Level of Evidence)
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.