

Summary
There is often a long time interval between the onset of stroke and treatment. Current transfer systems for getting patients to hospital or catheterization laboratories in order to undergo treatment are poorly developed. Additionally, current therapies are limited. This article discusses new data which may change the management of patients with acute stroke.
- Interventional Techniques & Devices
- Cerebrovascular Disease
- Interventional Radiology
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Cerebrovascular Disease
- Interventional Radiology
Horst Sievert, MD, CardioVascular Center Frankfurt, Frankfurt, Germany, discussed new data which may change the management of patients with acute stroke. He noted that there is often a long time interval between the onset of stroke and treatment. In addition, current transfer systems for getting patients to hospital or catheterization laboratories in order to undergo treatment are poorly developed. Finally, current therapies are limited.
The amount time in which the brain is without blood flow impacts the severity of the stroke and potential for recovery. There is often a considerable delay from the time in which patients first develop symptoms to the time in which they seek treatment. Efforts must be made to educate patients about the early signs of transient ischemic attack (TIA)/stroke and the need to quickly seek medical care when these symptoms occur. The time to treatment may also be improved by using ambulances specifically designed for transporting stroke patients. It may also be possible to reduce the amount of time needed to make the diagnosis of a stroke by utilizing mobile computed tomography (CT) scanners or bypassing the Emergency Department and taking patients directly to imaging. Providers could then take a history can be taken, perform lab tests, and ready the patient for thrombolysis while the patient is preparing to undergo imaging.
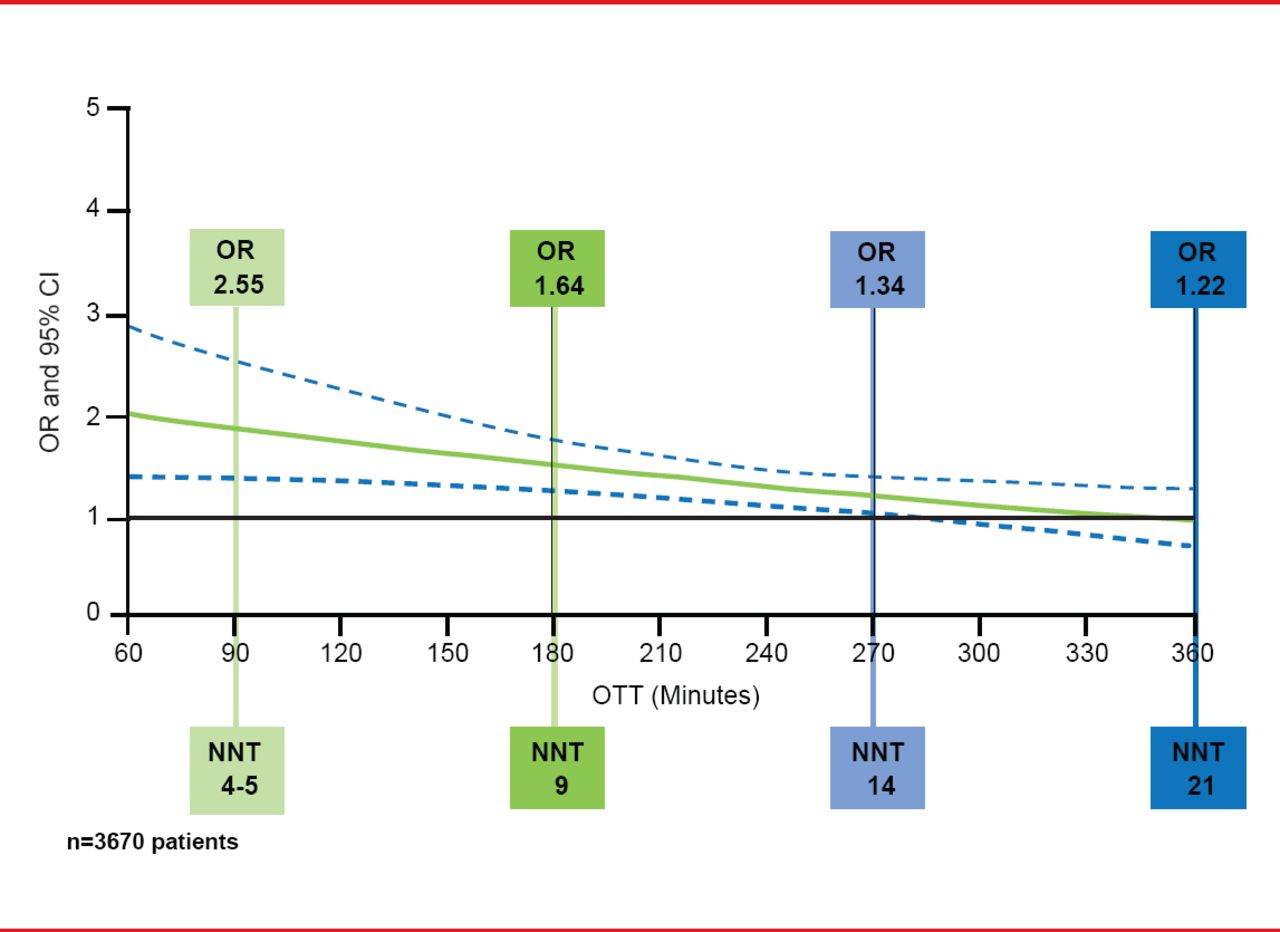
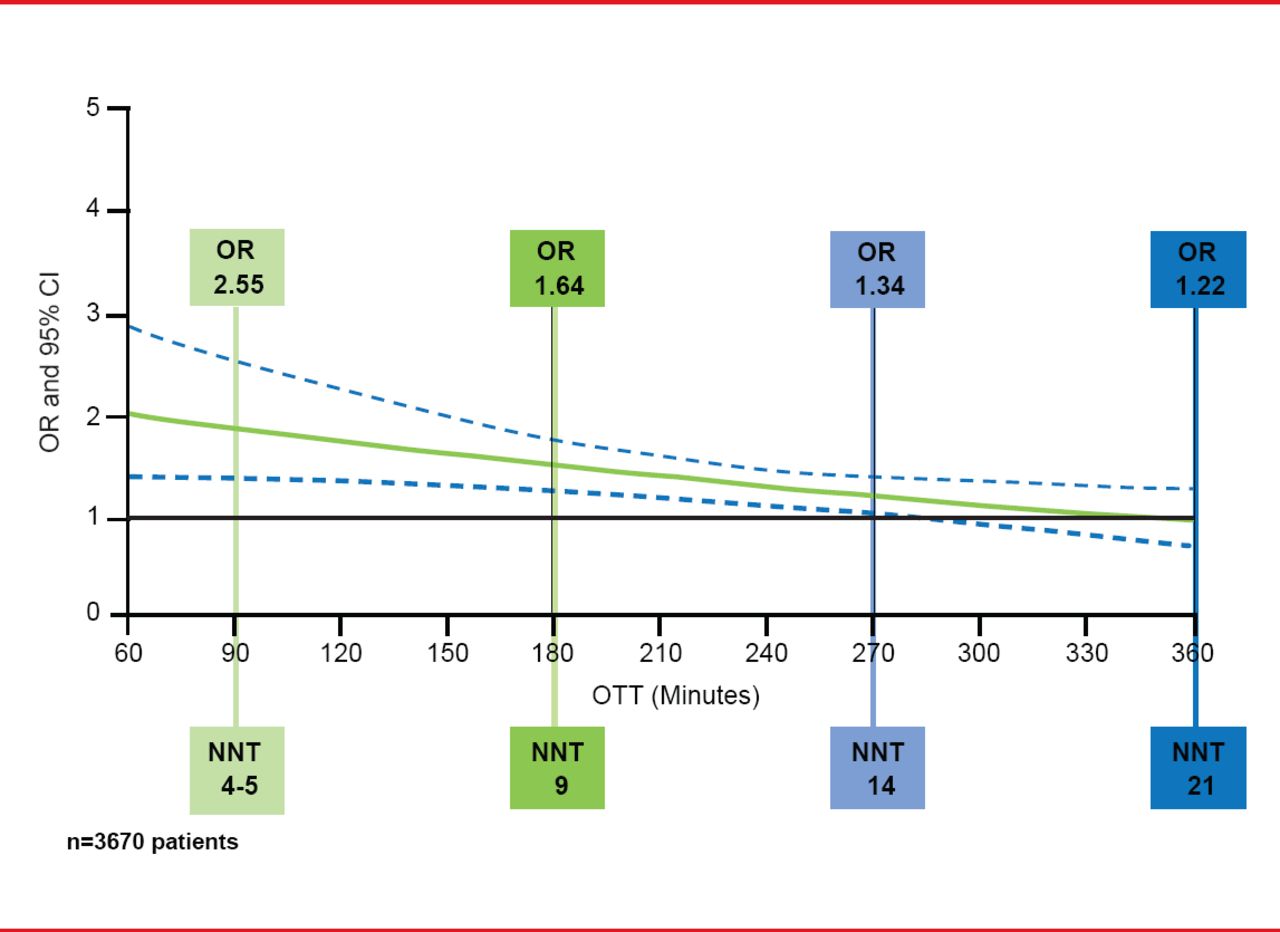
Expediting the treatment of patients with thrombolysis is important since data from a pooled analysis of early administration of recombinant tissue plasminogen activator (rtPA) after ischemic stroke showed benefit out to 4.5 hours after stroke onset. After 4.5 hours, the risk of thrombolysis may outweigh its potential benefits (Figure 1) [Lees KR et al. Lancet 2010].
Pooled Analysis rtPA for Acute Ischemic Stroke: Favorable Outcome (mRS 0–1) Versus Time
Reproduced from Lees KR et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet 2010;375(9727):1695–1703. With permission from Elsevier.
Thrombolysis improves outcomes in patients with acute ischemic stroke; however, the success of thrombolysis for the recanalization of large clots is poor (∼10% success) and reocclusion occurs in ∼20% of patients who initially have successful reperfusion. The use of angiography allows for better localization of the occlusion and allows for direct administration of thrombolytics to thrombus. In addition, mechanical thrombectomy devices can be used to obtain immediate reperfusion.
Although thrombolysis is still the gold standard therapy for acute stroke, more centers are developing clinical pathways based on severity, duration of symptoms, and the use of catheter intervention. Data from the PROACT-II study [Furlan A et al. JAMA 1999], IMS II trial [IMS Trial Investigators. Stroke 2007], and RECANLISE registry [Sen S et al. Neurocrit Care 2009], support the use of a catheter invention approach; however, recent data show no benefit from mechanical lysis compared with IV tPA (IMS III [Broderick JP et al. N Engl J Med 2013], SYNTHESIS [Ciccone A et al. N Engl J Med 2013], and MR Rescue [Kidwell CS et al. N Engl J Med 2013]). As a result, the optimal treatment for patients with ischemic stroke remains undefined.
Prof. Sievert proposed an algorithm to guide treatment selection based on time since symptom onset (Table 1).
Treatment Algorithm
Under multisociety consensus quality improvement guidelines [Sacks D et al. Catheter Cardiovasc Interv 2013], patients with the following characteristic benefit the most from mechanical recanalization:
-
▪ Patients in whom IV tPA is contraindicated or in whom IV tPA has failed or is likely to fail
-
▪ Patients with large vessel occlusion
-
▪ Very symptomatic patients
-
▪ Patients with a stroke time window out to 8 hours
-
▪ Patients with a proximal artery occlusion
“There is only one effective treatment for ischemic stroke,” said Prof. Sievert, “to get the vessel open.”
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.