

Summary
Practicing cardiologists are faced with many vascular challenges on an everyday basis. This article discusses the treatment options for asymptomatic carotid artery disease, recommendations for the screening and treatment of abdominal aortic aneurysms, a 5-step approach to the diagnosis and management of claudication, risk stratification for venous thrombosis, as well as the diagnosis and management of femoral access complications.
- Coronary Artery Disease
- Cerebrovascular Disease
- Interventional Techniques & Devices
- Coronary Artery Disease
- Cardiology & Cardiovascular Medicine
- Cerebrovascular Disease
- Interventional Techniques & Devices
Asymptomatic carotid artery disease (CAD), abdominal aortic aneurysm, intermittent claudication, venous thrombosis, and femoral access complications represent diverse vascular challenges for treating clinicians. Joshua A. Beckman, MD, Brigham and Women's Hospital, Boston, Massachusetts, USA, discussed the treatment options for asymptomatic CAD.
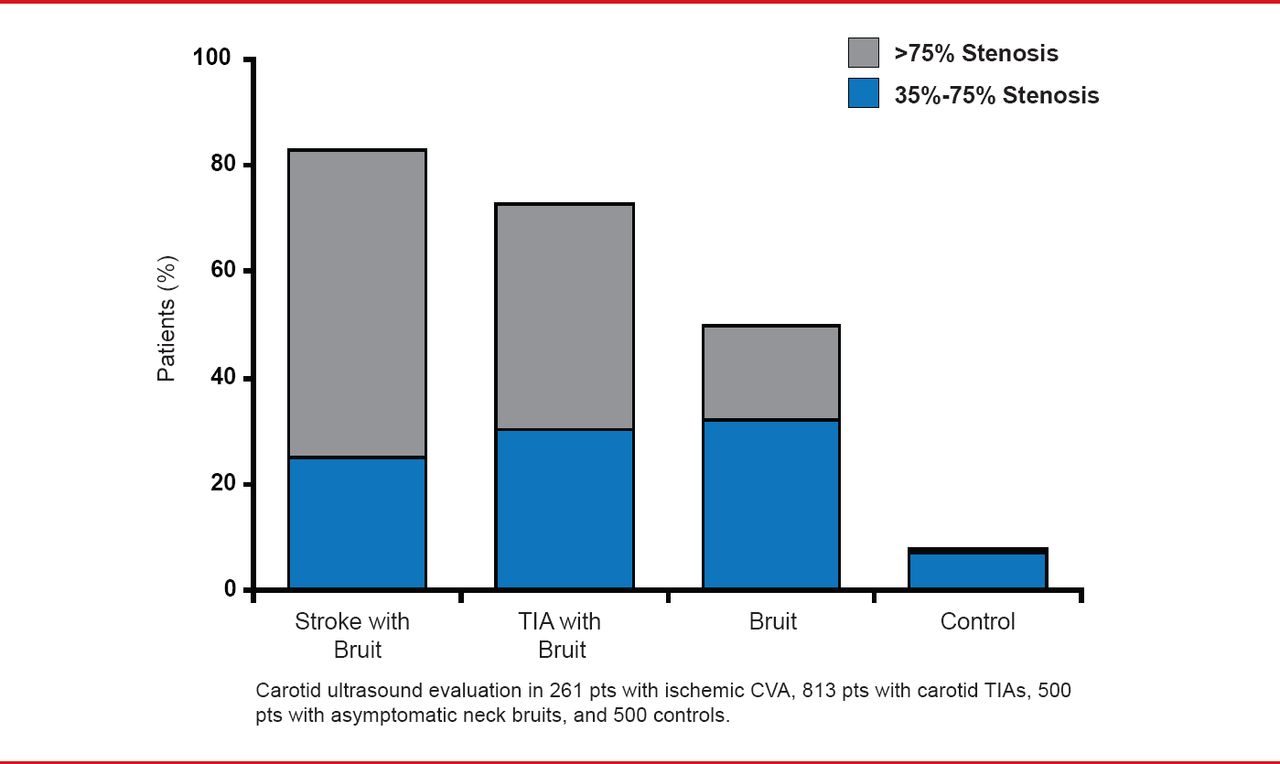
Whether or not to screen for asymptomatic carotid stenosis remains an area of intense debate with conflicting recommendations presented in guideline statements. It is clear, however, that the presence of a bruit is associated with carotid stenosis (Figure 1). In addition, the presence of a bruit is associated with adverse outcomes. Therefore, it may be reasonable to consider carotid ultrasound evaluation in patients with bruits, but it may not be necessary to screen patients without bruits.

Presence of Bruit Increases Likelihood of Carotid Disease
CVA=cardiovascular accident; TIA=transient ischemic attack.
Reproduced from Zhu C and Norris JW. Role of carotid stenosis in ischemic stroke. Stroke Aug 190;21(8):1131–1134. With permission from Lippincott Williams and Wilkins.
While guidelines clearly recommend optimal medical therapy (OMT) for patients with asymptomatic disease, there is ongoing debate regarding whether revascularization is beneficial and if so, which technique (surgical endarterectomy or percutaneous stenting) is optimal [Klein A et al. N Engl J Med 2008]. It can be challenging for clinicians to decide whether carotid revascularization is necessary for an individual patient and which revascularization method should be used.
While early trials of surgical endarterectomy showed benefit compared with OMT, data have shown consistent reductions in stroke risk with improving background therapy including the addition of statins [ACAS Investigators. JAMA 1995; Halliday A et al. Lancet 2010; Abbott AL. Stroke 2009]. This has led some to conclude that OMT alone is now the optimal approach [Abbott AL. Stroke 2009].
For those who recommend revascularization, the optimal approach remains unclear. The CREST study [Silver FL et al. Stroke 2011] compared carotid artery stenting with carotid endarterectomy in symptomatic and asymptomatic patients with high-grade carotid stenosis. No significant difference in stroke and death rates was found between carotid stenting and carotid endarterectomy in asymptomatic patients (p=0.15). Since study data indicate that neither technique is superior to the other, treatment decisions should be tailored to the individual patient.
James B. Froehlich, MD, MPH, University of Michigan, Ann Arbor, Michigan, USA, presented recommendations for the screening and treatment of abdominal aortic aneurysms (AAA). Risk factors associated with AAA include age, smoking, and family history of AAA [Lederle FA et al. Arch Intern Med 2000]. Female sex, diabetes, and black race are associated with a reduced risk of AAA. The ACC/AHA 2005 Guidelines for the Management of Patients with Peripheral Arterial Disease recommend that men aged ≥60 years who have a sibling or parent with AAA undergo a physical examination and ultrasound screening to detect aortic aneurysms [Hirsch AT et al. J Am Coll Cardiol 2006]. They also recommend that men aged 65 to 75 years who have ever smoked undergo a physical examination and 1-time ultrasound screening.
For AAA <5.5 cm, the ADAM study [Lederle FA et al. N Engl J Med 2002] and the UK Small Aneurysm trial [UK Small Aneurysm Trial Participants. N Engl J Med 2002] both found that survival is not improved by elective repair of AAA compared with surveillance.
For AAA ≥5.5 cm, surgery is generally recommended. Endovascular repair and open repair of AAA have been found to have similar rates of survival in long-term follow-up studies of the DREAM [De Bruin JL et al. N Engl J Med 2010] and EVAR trials [United Kingdom EVAR Trial Investigators. N Engl J Med 2010].
Heather L. Gornik, MD, Cleveland Clinic, Cleveland, Ohio, USA, presented a 5-step approach to the diagnosis and management of claudication. The first step is to complete a differential diagnosis, including a thorough vascular exam, to determine if the patient has claudication. If the patient has pain in either leg when walking and the pain goes away within 10 minutes of resting, there is a high likelihood of peripheral artery disease (PAD). Only 11% of patients with PAD have classic claudication [Hirsch AT et al. JAMA 2001].
The second step is to confirm the diagnosis of PAD with the Ankle-Brachial Index (ABI) as recommended by the ACC/AHA guidelines for the Management of Patients With Peripheral Artery Disease [Anderson JL et al. Circulation 2013]. If the patient has symptoms of intermittent claudication and the resting index is normal, the ABI should be measured after exercise.
Steps 3, 4, and 5 are considered the triad of PAD management: prevent myocardial infarction, stroke, and death; protect the feet to prevent amputation; and improve function and quality of life. According to Dr. Gornik, smoking cessation is the most important intervention for patients with PAD, and supervised exercise rehabilitation is highly effective for PAD.
J. Michael Bacharach, MD, MPH, North Central Heart Institute, Sioux Falls, South Dakota, USA, discussed risk stratification for venous thrombosis. Venous thromboembolic disease can range from calf vein thrombosis to hemodynamically significant pulmonary embolism. Patients with an acute iliofemoral deep vein thrombosis (DVT), a reasonable life expectancy, and no immediate threat to the affected limb, who receive care within 14 days after DVT development may be candidates for thrombolysis. In addition, patients with acute hemodynamically significant pulmonary embolism and a reasonable life expectancy or significant respiratory compromise may be candidates for thrombolysis.
A catheter directed approach for the delivery of thrombolytic therapy may be more efficient than intravenous treatment and allow for improved local delivery and lower doses. Thrombolysis has an increased risk of bleeding complications compared with heparin alone. Furthermore, some patients have absolute or relative contraindications to thrombolytic therapy.
Jeffry W. Olin, DO, Mount Sinai School of Medicine, New York, New York, USA, presented on the diagnosis and management of femoral access complications. During a postcatheterization ultrasound, there are 4 complications to look for: pseudoaneurysm, arteriovenous fistula, arterial closure device injury, and DVT. Risk factors associated with pseudoaneurysm formation include use of antiplatelet agents, anticoagulation, sheath size >8F, age >65 years, obesity, poor postprocedural compression, high or low puncture sites, simultaneous artery and vein catheterization, hypertension, PAD, hemodialysis, and complex interventions [Webber GW et al. Circulation 2007].
It is not possible to determine clinically if a patient has a pseudoaneurysm. If a patient has groin pain, new bruit, a pulsatile mass, or an expanding hematoma after catheterization, an ultrasound should be conducted to detect a possible pseudoaneurysm. The indications for surgical repair of pseudoaneurysms are [Webber GW et al. Circulation 2007]:
-
▪ Infected pseudoaneurysm
-
▪ Rapid expansion
-
▪ Failure of other therapies
-
▪ Skin necrosis
-
▪ Compressive syndromes
-
» Claudication
-
» Neuropathy
-
» Critical limb ischemia
-
Taken together, these vascular diseases provide several diagnostic and management challenges for practicing cardiologists and underscore the importance of physician education in these areas.
Mark A. Creager, MD, Brigham and Women's Hospital, Boston, Massachusetts, USA, provided the rationale for needing more physicians to undergo training in vascular medicine. Sequelae of atherosclerosis and thrombosis affect approximately 25 million people in the United States. However, not enough physicians have chosen vascular disease as an area of specialization to be available to treat these patients. Rapid advancements are being made in vascular biology, pharmacology, and technology, but vascular specialists are needed to optimize patient care.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.