

Summary
Key opinion leaders covered the 2013 updated European Society of Cardiology (ESC)/European Society of Hypertension (ESH) Guidelines for the management of arterial hypertension, highlighting new aspects of diagnosis and treatment [Mancia G et al. Eur Heart J 2013]. These 2013 ESC/ESH guidelines represent an update to those last published in 2007 [Mancia G et al. J Hypertens 2007], and although they reinforce and refine many pre-existing concepts, several new recommendations are included as well.
- Cardiology Guidelines
- Hypertensive Disease
- Cardiology & Cardiovascular Medicine
- Cardiology Guidelines
- Hypertensive Disease
Key opinion leaders covered the 2013 updated European Society of Cardiology (ESC)/European Society of Hypertension (ESH) Guidelines for the management of arterial hypertension, highlighting new aspects of diagnosis and treatment [Mancia G et al. Eur Heart J 2013]. These 2013 ESC/ESH guidelines represent an update to those last published in 2007 [Mancia G et al. J Hypertens 2007], and although they reinforce and refine many pre-existing concepts, several new recommendations are included as well.
Josep Redon, MD, PhD, University of Valencia, Spain, discussed new aspects in diagnosis of hypertension in the guidelines, emphasizing the increased consideration of hypertension in association with combined cardiovascular (CV) and other risk factors, such as diabetes and organ damage. The guidelines also include an increasing role for out-of-office blood pressure (BP) monitoring, especially when there is discordance between in-clinic and ambulatory BP measurements. Specific recommendations for special patient populations such as pregnant women, young patients, and the elderly, also are provided.
According to Robert H. Fagard, MD, PhD, Katholieke Universiteit, Leuven, Belgium, the guidelines encourage physicians to initiate antihypertensive strategies considering the patient's level of CV risk. They also recommend treating all patients aged <80 years to systolic BP (SBP) <140 mm Hg. For patients aged >80 years with SBP ≥160 mm Hg, the recommended SBP target is 140 to 150 mm Hg. Lifestyle changes are still recommended for all patients to help lower BP, including reducing salt intake to 5 to 6 g per day, and reducing weight to a body mass index of 25 kg/m2.
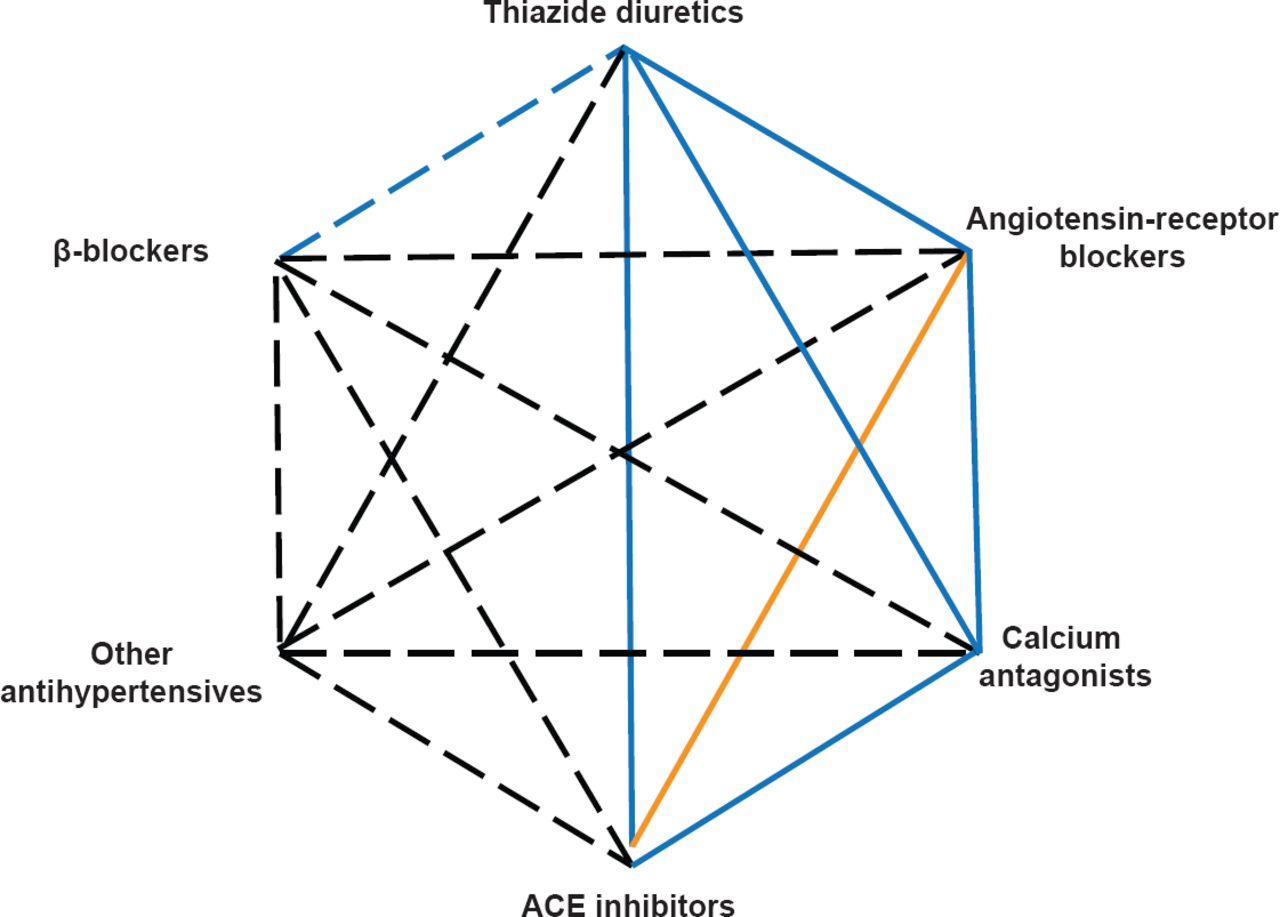
Sverre E. Kjeldsen, MD, PhD, University of Oslo, Ullevaal Hospital, Oslo, Norway summarized the recommended treatment algorithm. The updated guidelines indicate no preference for specific agents in uncomplicated hypertension, so all typical first-line drugs can be used. For patients requiring more than one drug, combinations of thiazide diuretics, calcium channel blockers, angiotensin receptor blockers, and angiotensin-converting-enzyme inhibitors is advised. Dual renin-angiotensin-aldosterone system blockade is no longer recommended, and diltiazem and verapamil should not be combined with a β-blocker. However, β-blockers remain the cornerstone of therapy for patients with heart failure, coronary disease, and tachyarrhythmias (Figure 1).
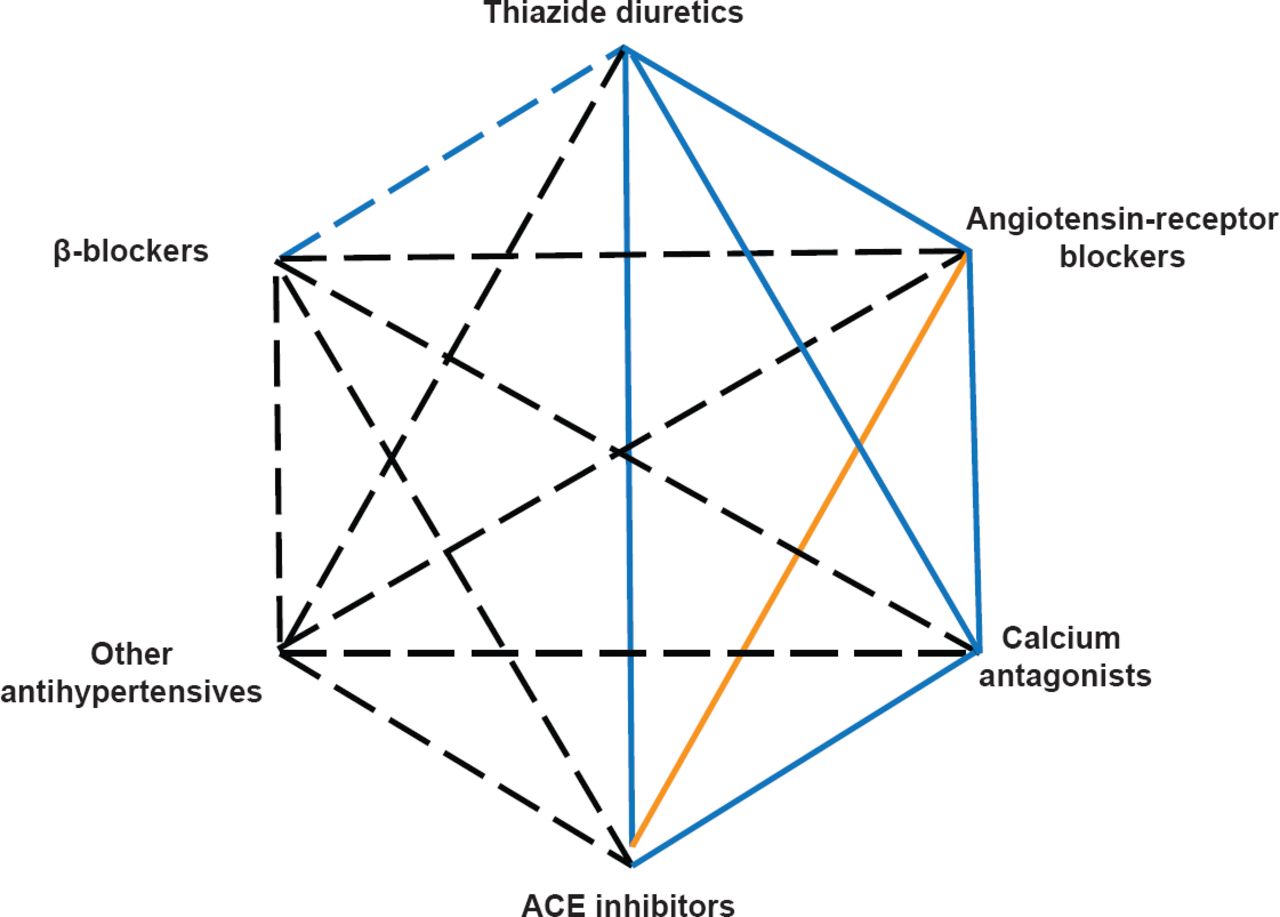
2013 Drug Combinations for the Treatment of Hypertension
ACE=angiotensin-converting enzyme.
Mancia G et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2013;34(28):2159–2219. With permission from Oxford University Press.
Giuseppe Mancia, MD, University of Milano-Bicocca, Milan, Italy, summarized clinical trials demonstrating the protective effect of reducing BP below 140/90 mm Hg. The International Verapamil SR Trandolapril Study [INVEST], for example, was designed to evaluate whether study outcomes are related to consistency of BP control below this target [Mancia G et al. Hypertension 2007]. In 22,576 patients with hypertension and coronary artery disease, as the number of visits where BP was 140/90 mm Hg increased, fewer CV events occurred. A similar association was also demonstrated by the Ongoing Telmisartan Alone and in Combination With Ramipril Global End Point Trial [ON TARGET; Mancia G et al. Circulation 2011].
Prof. Mancia concluded, however, that there is no evidence from randomized trials of an additional beneficial effect of more aggressive therapy to reduce SBP below 130 mm Hg [Barzilay JI et al. Diabetes Care 2012; Appel LJ et al. N Engl J Med 2010; Ruggenenti P et al. Lancet2005; Beri T et al. Ann Intern Med 2003].
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.