

Summary
This article addresses the rising problem of hypertension and its complications, especially in black patients. Included topics are strategies for maximizing blood pressure (BP) control and the current BP goals as recommended by 2013 European Society of Hypertension (ESH)-European Society of Cardiology (ESC) and Joint National Committee (JNC) 7 guidelines.
- Hypertensive Disease
- Cardiology & Cardiovascular Medicine
- Hypertensive Disease
Arthur Liqui-Lung, MD, Stichting Teaching Hospital, Willemstad, Curaçao, Netherlands Antilles, addressed the rising problem of hypertension and its complications, especially in black patients. He discussed strategies for maximizing blood pressure (BP) control and the current BP goals as recommended by 2013 European Society of Hypertension (ESH)–European Society of Cardiology (ESC) and Joint National Committee (JNC) 7 guidelines.
Hypertension is already a major global health challenge with the prevalence only expected to increase in the coming decades. Based on a pooled analysis of regional data, an estimated 972 million adults worldwide had hypertension in 2000 with a predicted increase by 60% to 1.56 billion by 2025 [Kearney PM et al. Lancet 2005]. To maximize the reduction in the long-term risk of death owing to cardiovascular consequences, prevention and control of hypertension will be critical. Even a 2-mm Hg reduction in systolic BP can lower mortality risk from ischemic heart disease and stroke by 7% and 10%, respectively [Lewington S et al. Lancet 2002].
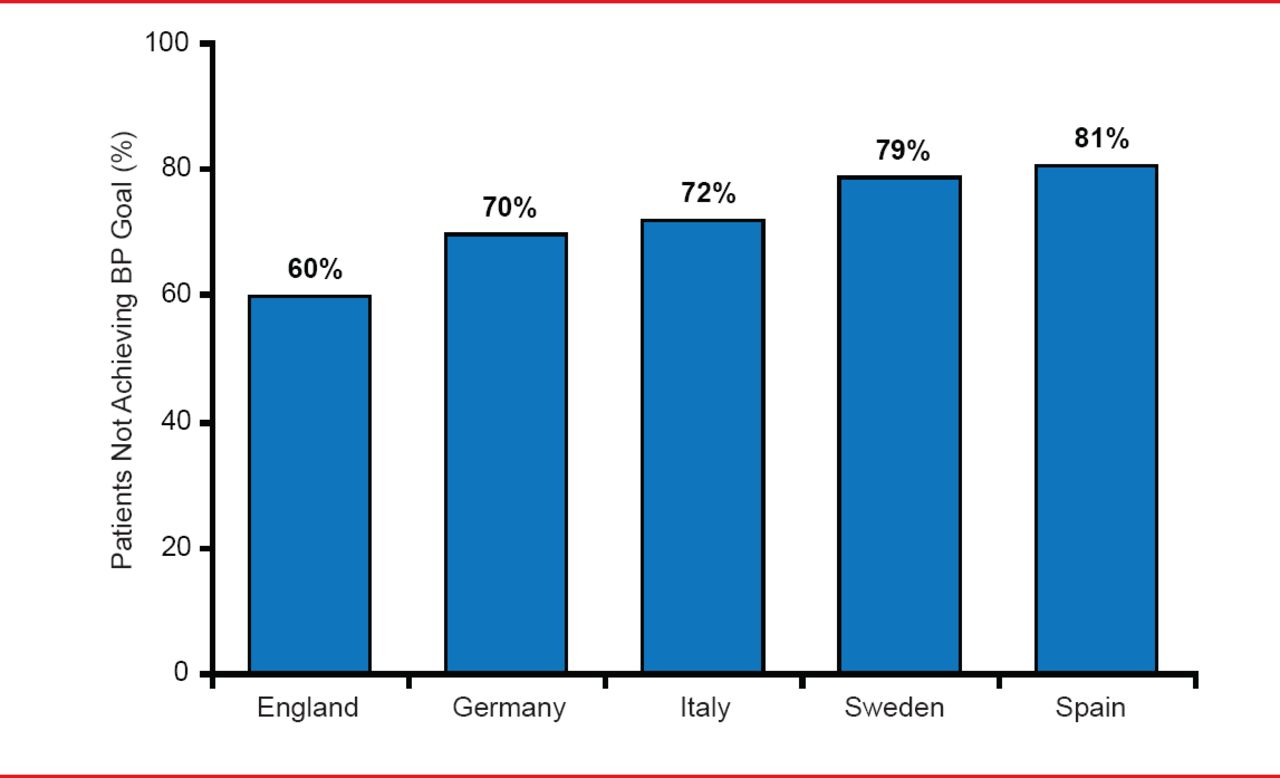
Current guidelines indicate a target BP of <140/90 mm Hg for patients without diabetes mellitus, kidney disease, or cardiovascular disease, with lower targets for those with one or more of these conditions (Table 1). Despite knowledge on lifestyle interventions and availability of effective medications, even countries with enviable healthcare systems report low attainment of current BP targets. A 2004 European study demonstrated that as many as 80% of patients receiving therapy for hypertension fail to reach target BP goals of <140/90 mm Hg (Figure 1) [Wolf-Maier K et al. Hypertension 2004].
Current BP Guidelines
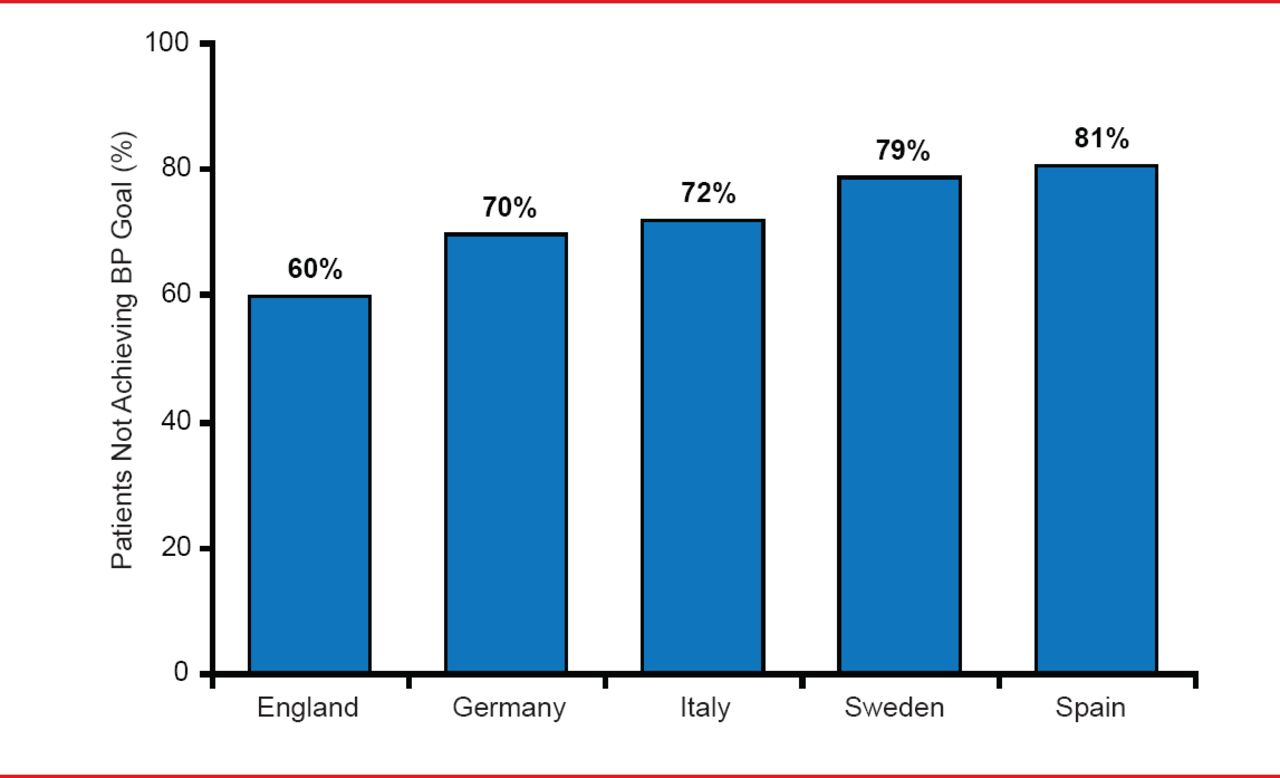
Failure to Achieve BP Goals in Europe
BP=blood pressure.
Source: Wolf-Maier K et al. Hypertension 2004.
Dr. Liqui-Lung highlighted that hypertension and its sequelae are more prevalent in black patients, providing an even greater challenge to regions like the Caribbean with a high proportion of patients with African ancestry [Flack JM et al. Hypertension 2010]. In addition, there are important differences regarding hypertension in blacks including, a greater role for hypertension in the development of heart failure, different responses to standard therapies, and greater difficulty in achieving current targets. In its 2010 consensus statement, the International Society on Hypertension in Blacks prioritized lifestyle education even in the setting of “normal” BP, slightly earlier initiation of pharmacologic therapy at 135/85 mm Hg in comorbidities, and rapidly switching from single to combination drug therapy if BP does not decrease quickly.
Medication compliance and persistence can significantly BP as well as overall medical costs significantly [Sokol MC et al. Med Care 2005]. Realizing these benefits, however, is a considerable challenge in an era of polypharmacy and with adequate hypertension therapy often requiring more than one agent [Düsing R. Vasc Health Risk Manag 2010; Mancia G et al. Blood Press 2009; Chobanian AV et al. Hypertension 2007; Milani RV. Am J Manag Care 2005; Materson BJ et al. N Engl J Med 1993; Düsing R. Vasc Health Risk Manag 2010; Mancia G et al. Blood Press. 2009]. One study also showed that when a drug from a second class of BP-lowering agents is combined with a patient's first antihypertensive drug, BP is reduced 5 times more than if the dose of the first drug was doubled [Wald DS et al. Am J Med 2009].
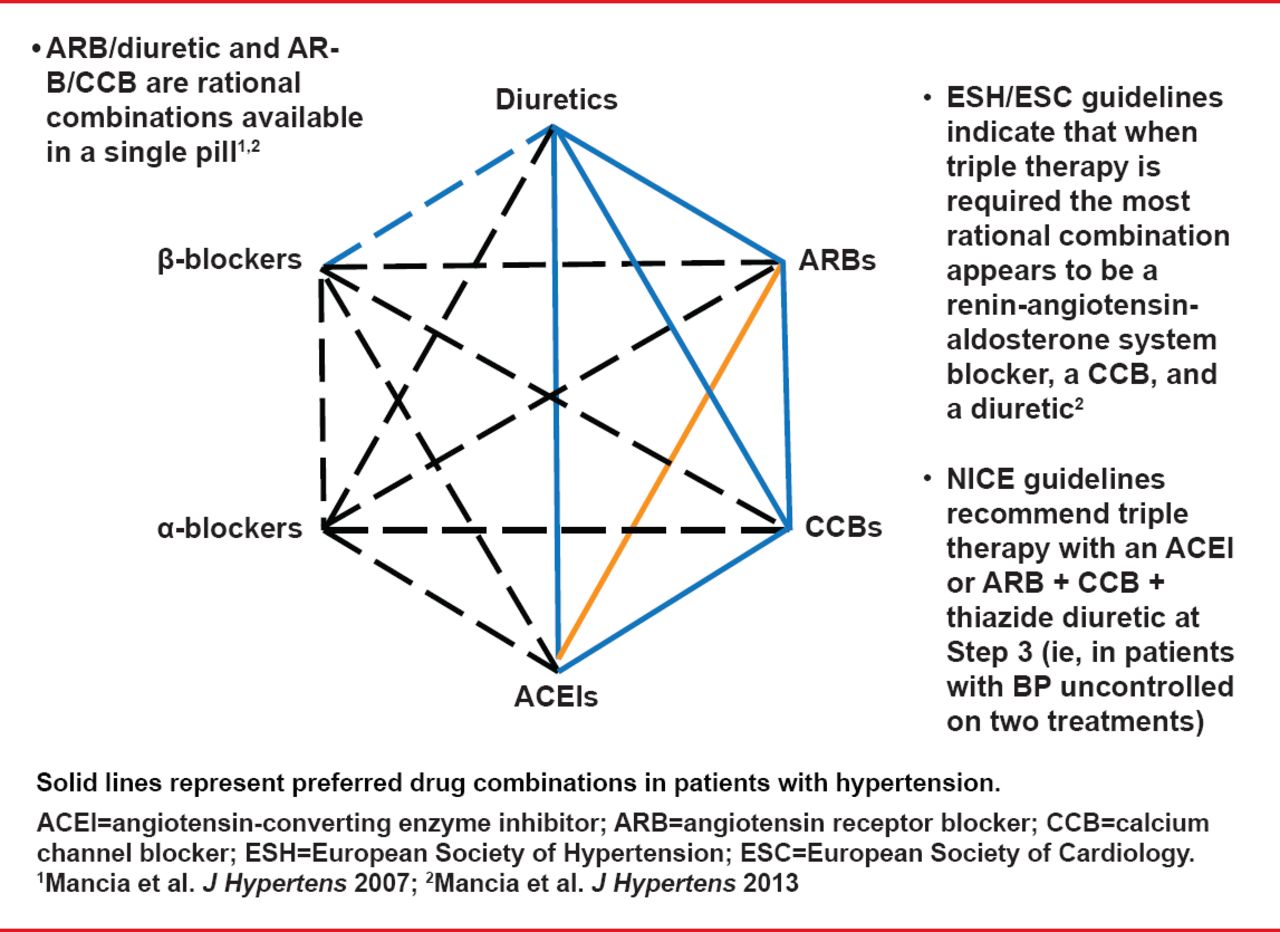
Dr. Liqui-Lung discussed evidence demonstrating that patients receiving combination drug therapy (ie, in a single pill) were significantly (p<0.0001) more likely to adhere to therapy than those receiving free-combination therapy [Gerbino PP, Shoheiber O. Am J Health Syst Pharm 2007]. The ESH–ESC and JNC 7 guidelines recommend initiation of combination drug therapy in all patients with BP >20/10 mm Hg above goal or in patients with a high risk of CVD (Figure 2) [Lenfant C et al. Hypertension 2003; Mancia G et al. Blood Press 2009].
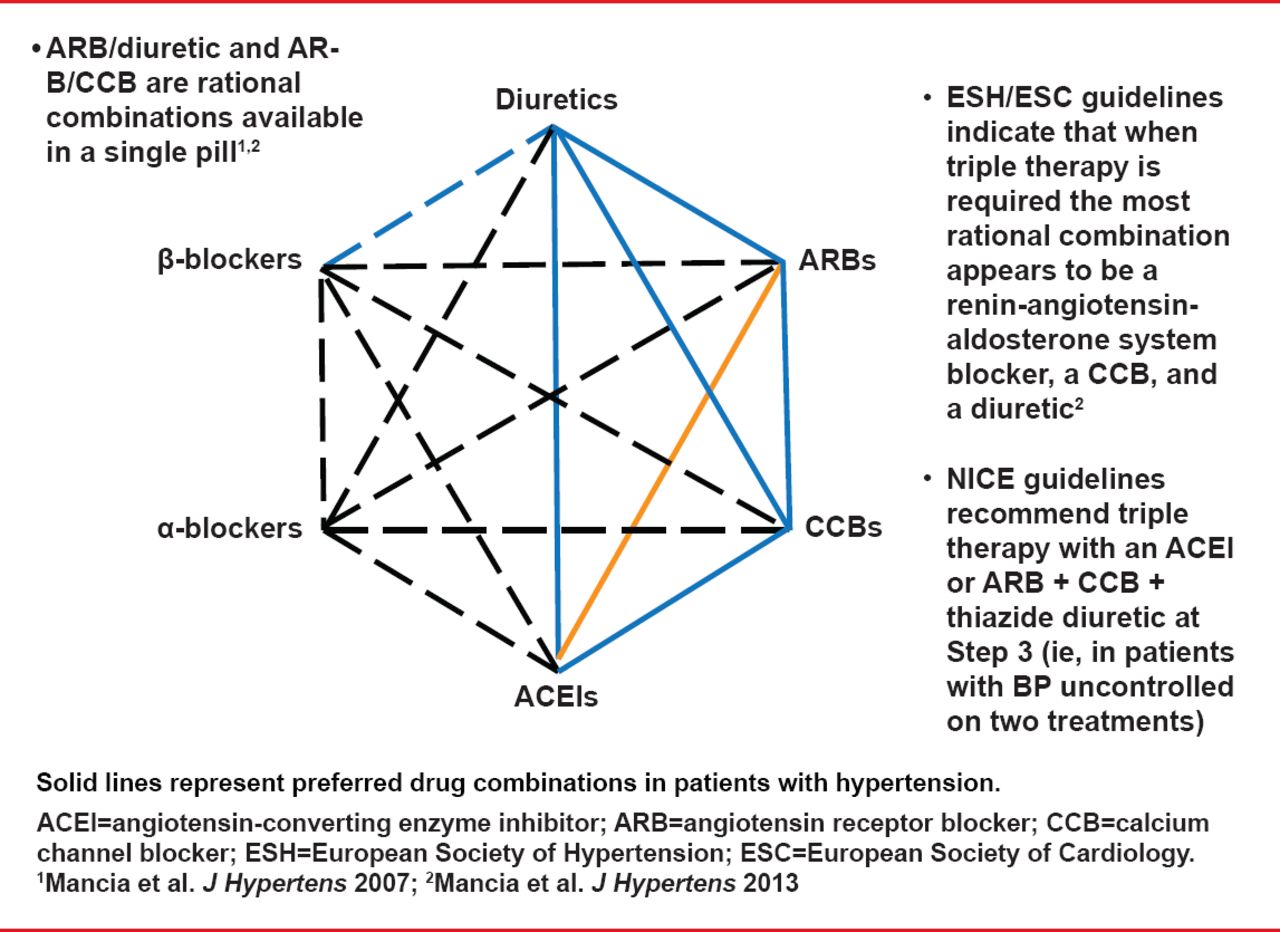
ESH-ESC Guidelines for Combining Antihypertensive Drugs]
Reproduced from Mancia G et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2013;34(28)2159–2219. With permission from Oxford University Press.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.