

Summary
Atrial fibrillation (AF) is a leading reason for physicians to prescribe warfarin treatment in the elderly. The prevalence of AF increases with age [Chen LY, Shen WK. Heart Rhythm 2007]. By 2050, the projected number of persons with AF in the United States will exceed 10 million [Miyasaka Y et al. Circulation 2006], and 12%, or 1 in 8 Americans, will be aged =75 years. This article discusses the need to optimize anticoagulant treatment in the elderly.
- Arrhythmias
- Thrombotic Disorders
- Hematology
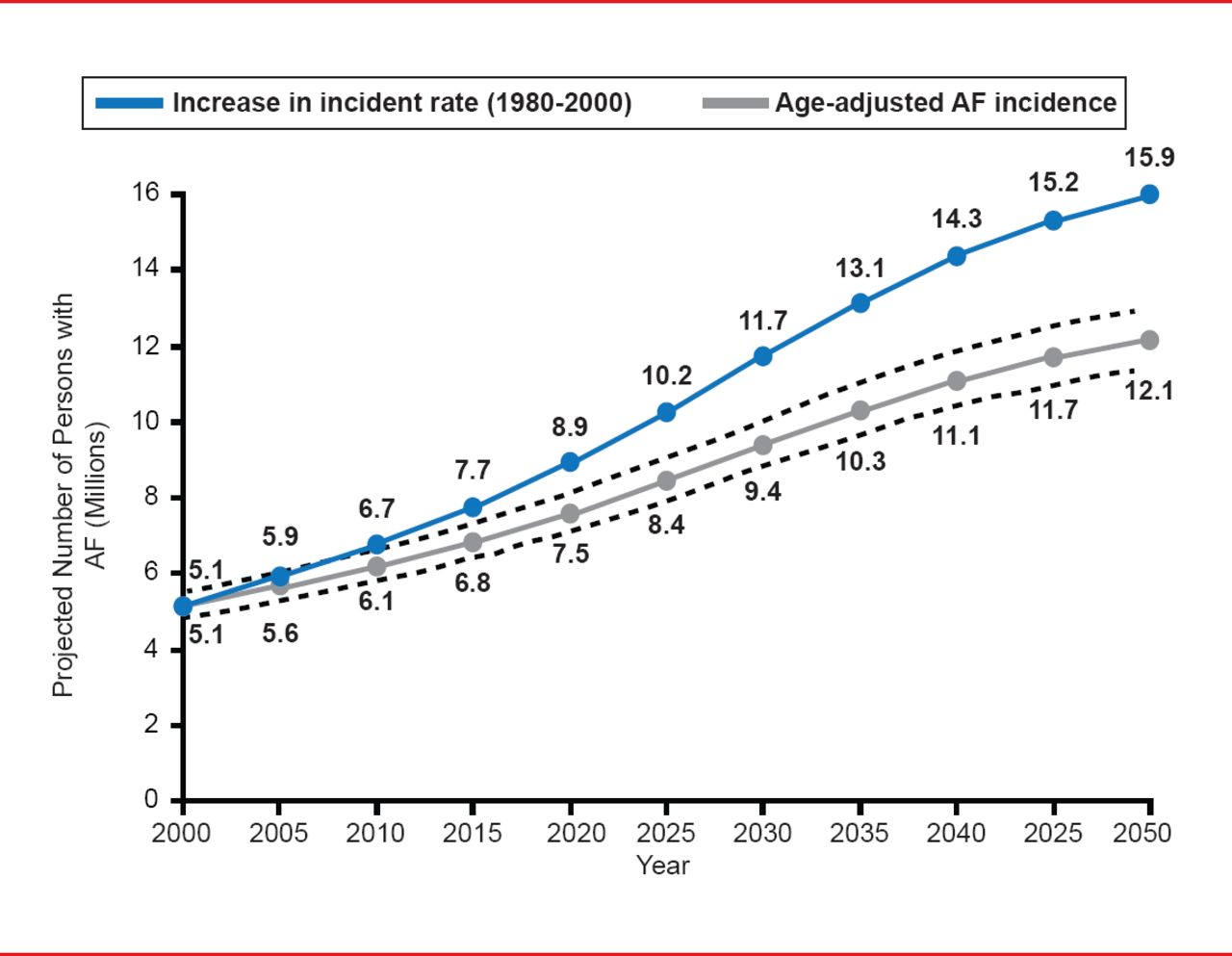
Atrial fibrillation (AF) is a leading reason for physicians to prescribe warfarin treatment in the elderly. The prevalence of AF increases with age [Chen LY, Shen WK. Heart Rhythm 2007]. By 2050, the projected number of persons with AF in the United States will exceed 10 million (Figure 1) [Miyasaka Y et al. Circulation 2006], and 12%, or 1 in 8 Americans, will be aged ≥75 years, said Elaine M. Hylek, MD, MPH, Boston University Medical Center, Boston, Massachusetts, USA, who presented on the need to optimize anticoagulant treatment in the elderly.
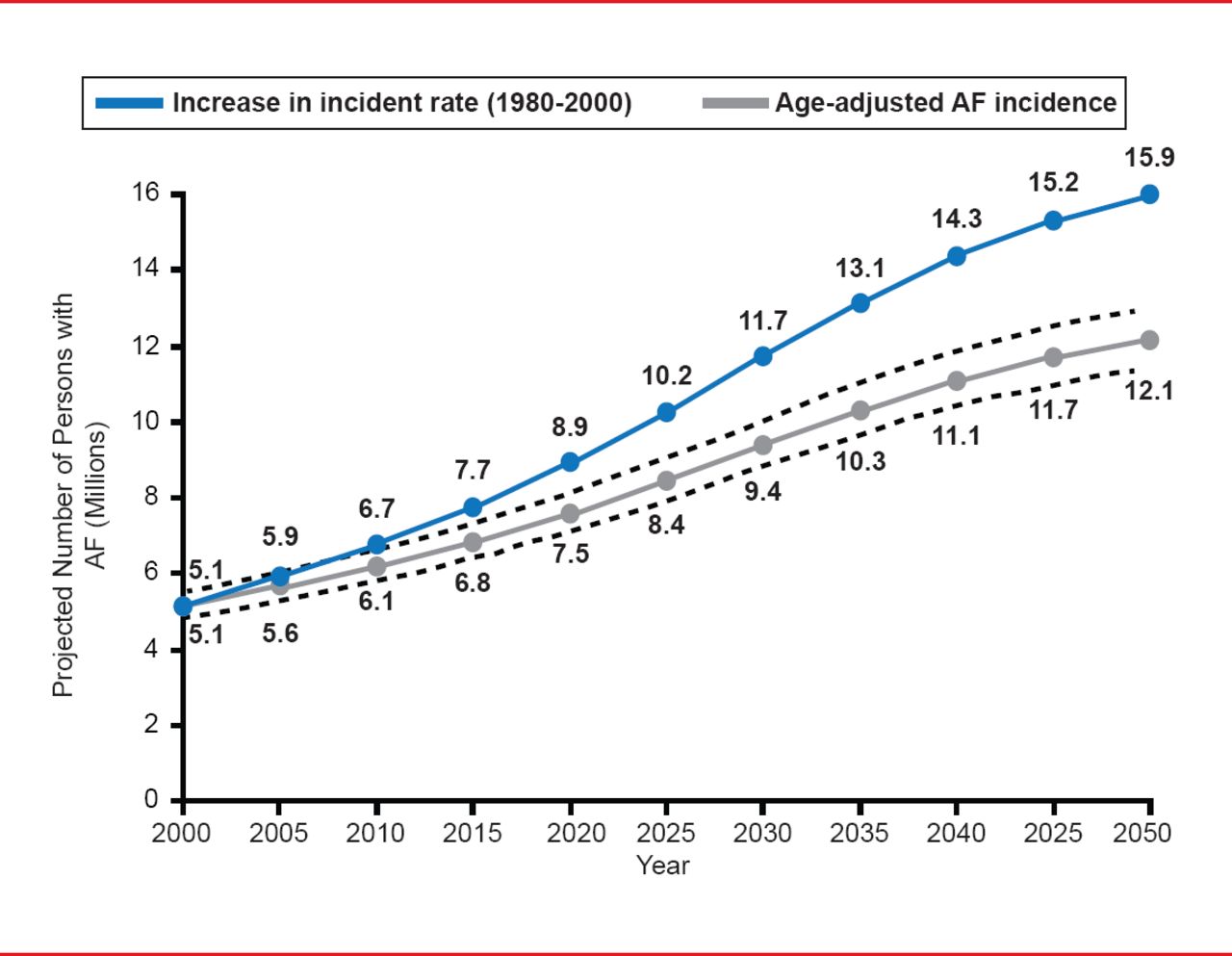
Projected Number of Persons With Atrial Fibrillation in the United States Between 2000 and 2050
Reproduced from Miyasaka Y et al. Secular Trends in Incidence of Atrial Fibrillation in Olmsted County, Minnesota, 1980 to 2000, and Implications on the Projections for Future Prevalence, Circulation 2006;114(2):119–125. With permission from the American Heart Association.
Warfarin is effective in the prevention of stroke in AF, but is underused in clinical care [Hylek EM et al. Circulation 2007]. They found that of 472 patients, 32% were aged ≥80 years, and 91% had ≥1 stroke risk factor. The cumulative incidence of major hemorrhage for patients aged ≥80 years was 13.1 per 100 person-years versus 4.7 for those aged ≤80 years (p=0.009). Within the first year, 26% of patients aged ≥80 years stopped taking warfarin, with 81% due to perceived safety issues. Rates of major hemorrhage and warfarin termination were highest among patients with CHADS2 scores of ≥3.
A review of emergency hospitalizations for adverse drug events in older Americans relating to hematological agents is shown in Table 1 [Budnitz DS et al. N Engl J Med 2011].
Hazards of Warfarin
Nonetheless, the decision to not resume warfarin therapy in the 90 days following gastrointestinal tract bleeding (GIB) is associated with increased risk for thrombosis and death [Witt DM et al. Arch Intern Med 2012]. In their analysis of 442 patients with warfarin-associated index GIB, 260 patients (58.8%) resumed warfarin therapy. This strategy was associated with a lower adjusted risk for thrombosis (HR, 0.05; 95% CI, 0.01 to 0.58) and death (HR, 0.31; 95% CI, 0.15 to 0.62), without significantly increasing the risk for recurrent GIB (HR, 1.32; 95% CI, 0.50 to 3.57).
Dr. Hylek reports that AF stroke is associated with a 30-day mortality rate of 24% among individuals not taking antithrombotic therapy. Given the morbidity and mortality related to AF stroke, it is important to remain attentive to the factors that increase the risk of hemorrhage. Blood pressure control reduces the risk of both ischemic stroke and intracranial hemorrhage. Concomitant use of aspirin should be avoided. The risk of falls in the older adult is multifactorial and a major source of serious injury. Interventions to reduce this risk should be sought.
Multiple strategies can be used to improve the quality of anticoagulant therapy in the elderly. These call on physicians to stay current with physiological changes in their patients that occur with increasing age, identify hazards amenable to intervention, improve management of antithrombotic drugs, and implement strategies to optimize the use of anticoagulants in the elderly.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.