

Summary
The new 2013 European Society of Cardiology (ESC) Guidelines on cardiac pacing and cardiac resynchronization therapy (CRT) were recently published in the European Heart Journal and Europace [Brignole M et al. Eur Heart J 2013; Europace 2013]. Michele The structural goals of the new guidelines were to provide short and simple indications with a description of both benefits and potential complications related to each treatment. In addition, acknowledgement was made of any differing opinions by any of the contributors from the final recommendations.
- Cardiology Guidelines
- Arrhythmias
- Cardiology & Cardiovascular Medicine
- Cardiology Guidelines
- Arrhythmias
The new 2013 European Society of Cardiology (ESC) Guidelines on cardiac pacing and cardiac resynchronization therapy (CRT) were recently published in the European Heart Journal and Europace [Brignole M et al. Eur Heart J 2013; Europace 2013]. Michele Brignole, MD, Ospedali del Tigullio, Tigullio Lavagna, Italy, introduced the structure of the manuscript, the contributors, and the concepts behind the level of evidence. The structural goals of the new guidelines were to provide short and simple indications with a description of both benefits and potential complications related to each treatment. In addition, acknowledgement was made of any differing opinions by any of the contributors from the final recommendations. The quality of evidence that was used to make a recommendation is also noted in the guidelines, including whether or not additional data is likely or not likely to change a recommendation.
Richard Sutton, MD, St. Mary's Hospital, London, United Kingdom, presented the new ESC recommendations for cardiac pacing for bradycardia. The ESC guidelines recommend pacing in patients with sinus node disease when the symptoms are clearly attributed or most likely due to bradycardia [Brignole M et al. Eur Heart J 2013; Europace 2013]. However, if sinus node disease is asymptomatic or reversible, pacing is not indicated. Pacing is also recommended in patients with third- or second-degree type 2 atrioventricular (AV) block, and in patients with second-degree type 1 AV block with symptoms due or located at intra-His or infra-His levels.
The new guidelines state that pacing is indicated in carotid sinus syncope (CSS) if patients have dominant cardioinhibitory carotid sinus syndrome and recurrent unpredictable syncope, or tilt-induced cardioinhibitory syncope with recurrent and frequent unpredictable syncope, if they are aged >40 years. However, Prof. Sutton pointed out that CSS is a relatively benign condition, as it does not appear to reduce survival. Therefore, pacing may help relieve syncope burden, as pacing results in a 75% decrease in recurrence compared with the natural history of the condition. Syncopal recurrence occurs in ∼20% of patients within 5 years.
Victoria Delgado, MD, Leiden University Medical Center, Leiden, The Netherlands, discussed the guideline updates on CRT in patients in sinus rhythm. Patients with and without left bundle branch block, a QRS duration of 120 ms or more, a left ventricular ejection fraction (LVEF) of ≤35%, and who remain in NYHA Functional Class II, III, or ambulatory IV are candidates for CRT [Brignole M et al. Eur Heart J 2013; Europace 2013]. Patients with a QRS duration of <120 ms are not recommended to receive CRT. A meta-analysis of the effect of QRS duration on outcomes following CRT demonstrated a combined risk ratio (RR) of 0.60 (95% CI, 0.53 to 0.67; p<0.001) in patients with a QRS duration of 150 ms or greater and an RR of 0.95 (95% CI, 0.82 to 1.10; p=0.49) in patients with a QRS duration of 120 to 149 ms [Sipahi I et al. Ann Intern Med 2011].
Interestingly, there were differences of opinion among the contributors of the 2013 ESC Guidelines in regards to the recommendations for CRT in patients in sinus rhythm [Brignole M et al. Eur Heart J 2013; Europace 2013]. Dissent was primarily due to the data on which the recommendations were based; some recommendations are based on subanalyses of randomized controlled trials and their interpretation may be problematic. Therefore, the ESC Guidelines acknowledge that additional data may change the recommendations in the future.
Pacing mode is mostly recommended to be biventricular (BiV), as a survival benefit and decreased hospitalization is associated with BiV pacing compared with LV pacing [Brignole M et al. Eur Heart J 2013; Europace 2013]. However, Prof. Delgado pointed out that LV pacing lowers the cost and complexity of the procedure, while potentially increasing the lifespan of the device. Therefore, LV pacing may be considered in children and young adults.
Christophe Leclercq, MD, PhD, Rennes University Hospital, Rennes, France, discussed CRT in patients with atrial fibrillation (AF). Prof. Leclercq highlighted that there is a lack of CRT randomized controlled trials that are dedicated to or include patients with AF, yet ∼25% of patients that receive CRT have AF. Patients are candidates for CRT only if they have permanent or long-standing, persistent AF.
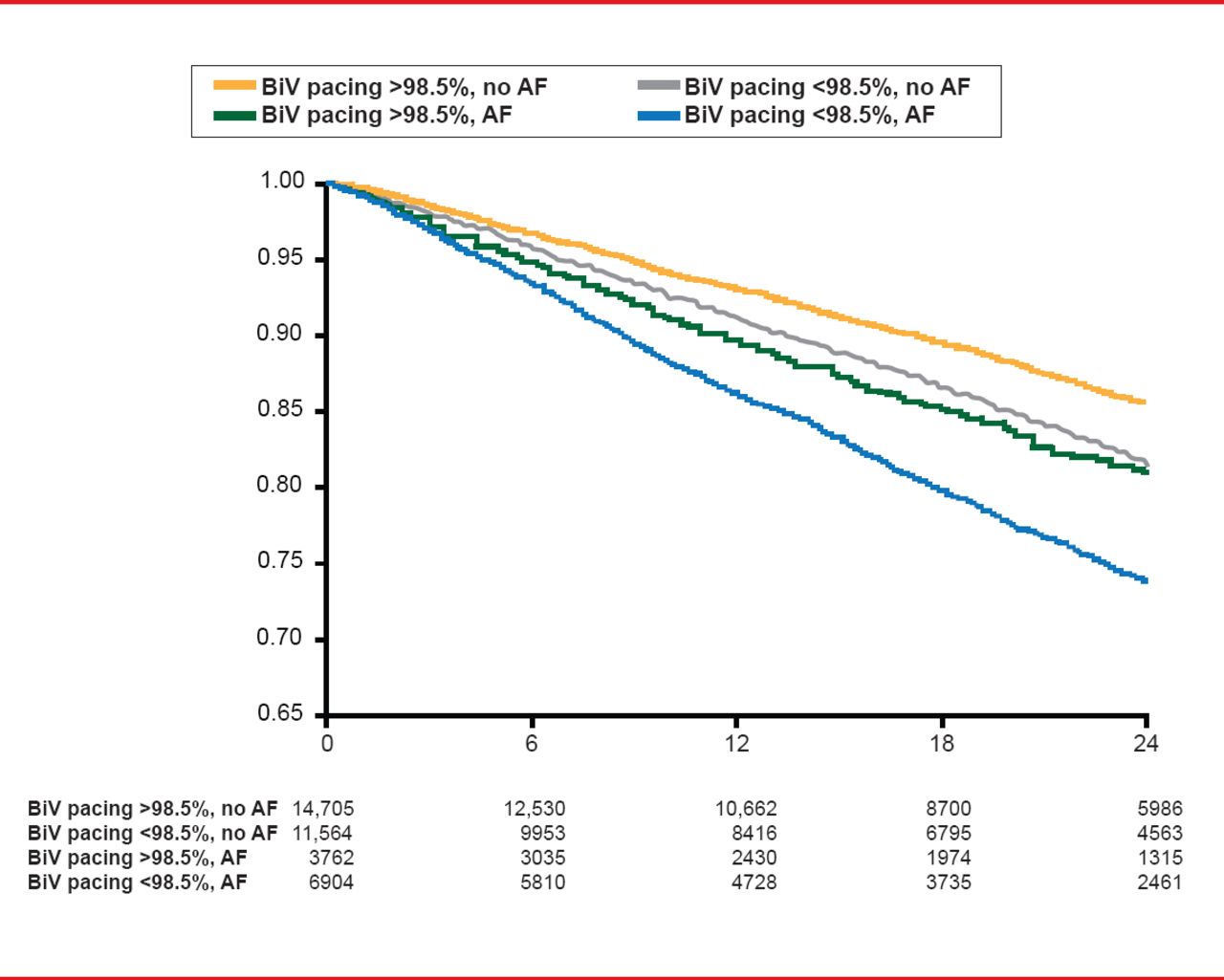
Prof. Leclercq presented data that demonstrated that AF patients that received BiV pacing >98.5% of the time experienced a greater survival rate, compared with AF patients that had BiV pacing <98.5% (Figure 1) [Hayes D et al. Heart Rhythm 2011].
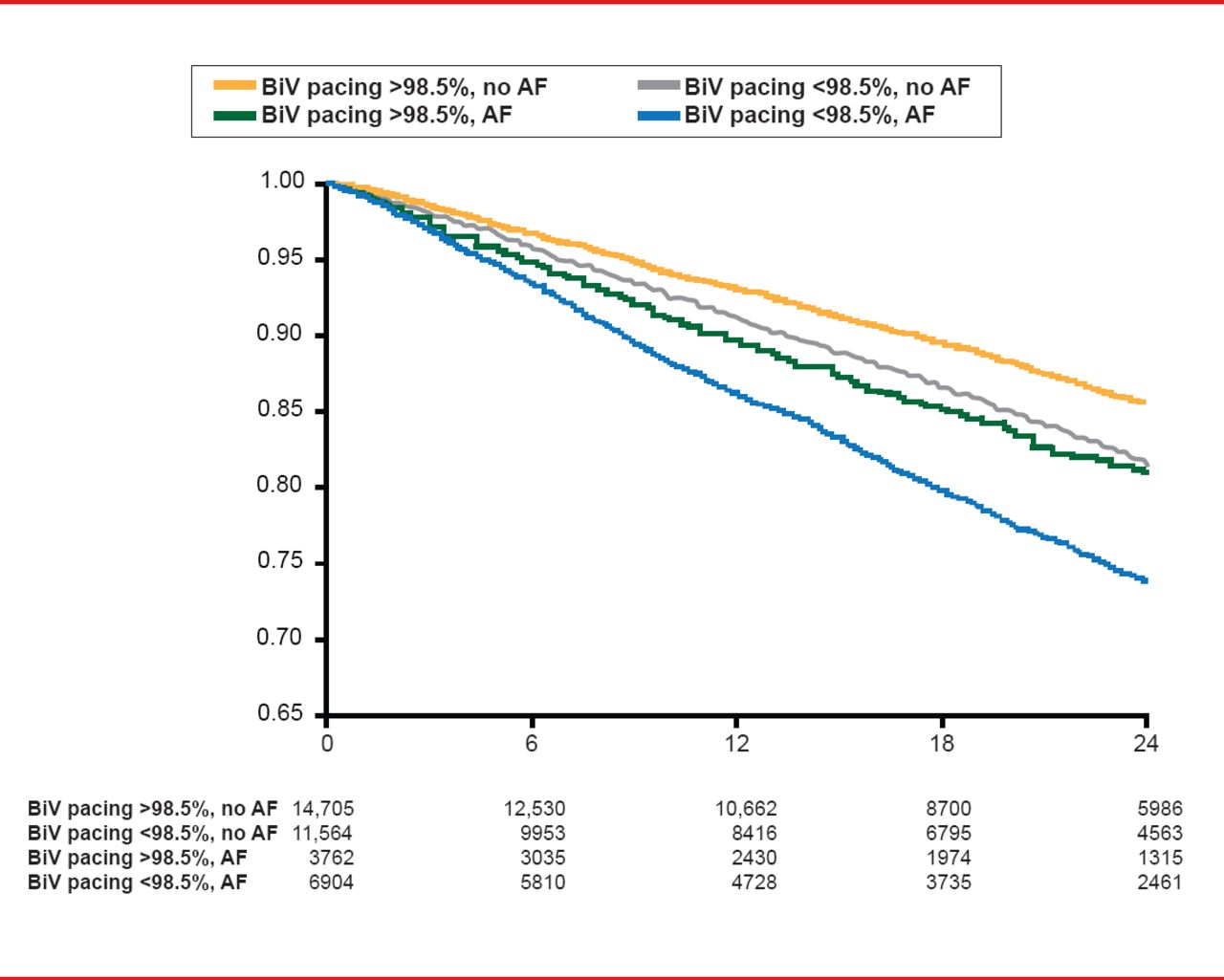
Effect of Biventricular Pacing in Patients With AF
AF=atrial fibrillation; BiV=biventricular.
Reproduced from Hayes DL et al. Cardiac resynchronization therapy and the relationship of percent biventricular pacing to symptoms and survival. Heart Rhythm 2011;8(9):1469–1475. With permission from Elsevier.
AV node ablation appears to be important in patients with AF, with benefits to survival and remodeling [Gasparini M et al. J Am Coll Cardiol 2006; Ganesan AN et al. J Am Coll Cardiol 2012]. In addition, the 2013 ESC Guidelines recommend that patients with uncontrolled heart rate with AF that are candidates for AV ablation should also be considered for pacing [Brignole M et al. Eur Heart J 2013; Europace 2013]. Prof. Leclercq noted that although the evidence is fairly weak for CRT in patients with persistent AF, the prevailing expert opinion is that CRT should be considered and AV ablation should be added in patients that have a BiV capture of <99%.
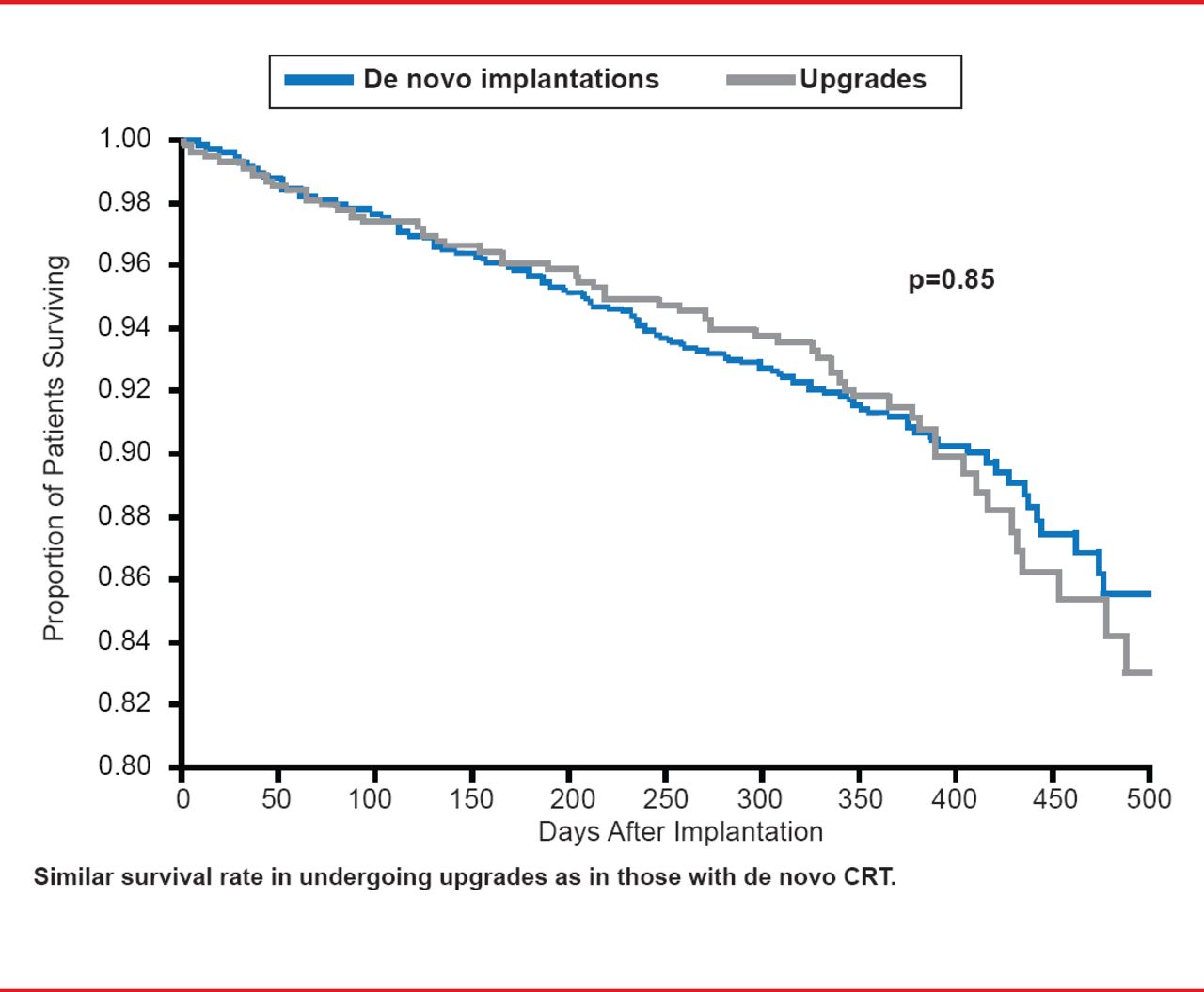
Cecilia Linde, MD, Karolinska University Hospital, Solna, Sweden, presented on CRT in patients with conventional pacemakers. The 2013 ESC Guidelines state that upgrading from a conventional pacemaker or implantable cardioverter-defibrillator (ICD) to CRT is recommended in patients with NYHA II-III HF or ambulatory NYHA IV, LVEF <35% despite optimal medical therapy and who have a high percentage of ventricular pacing; with the goal of decreasing the risk of worsening HF [Brignole M et al. Eur Heart J 2013; Europace 2013]. In several small randomized crossover studies, patients with HF NYHA III to IV and LVEF of <40% that were upgraded to CRT experienced symptomatic improvements and decreased hospitalizations, as compared with right ventricular (RV) pacing. In a survey study, patients that had de novo and upgraded CRT experienced similar rates of survival (Figure 2) [Bogale N et al. Eur J Heart Fail 2011].
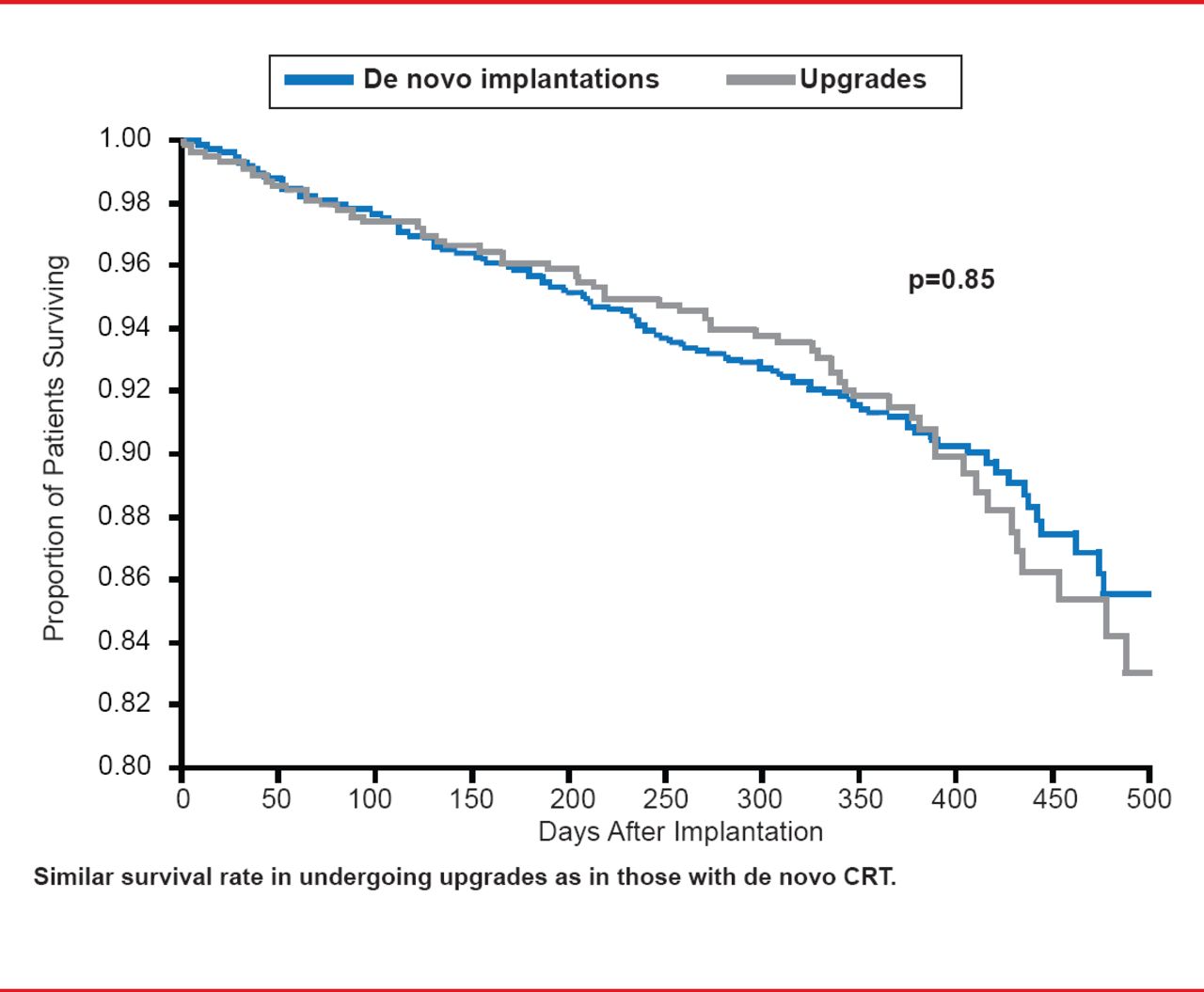
Survival Rate Following de Novo Implantation or Upgrade to CRT
Reproduced from Bogale N et al. The European Cardiac Resynchronization Therapy Survey: comparison of outcomes between de novo cardiac resynchronization therapy implantations and upgrades. Eur J Heart Fail 2011;13(9):973–983. With permission from Oxford University Press.
Prof. Linde highlighted the recommendation that patients with bradycardia should be considered for de novo CRT because a high extent of right ventricular (RV) pacing has been shown to be associated with an increased risk for hospitalizations and deterioration of LV function in prior studies of patients paced due to sinus node disease or those receiving an ICD.
De novo CRT compared with RV pacing was studied in the BLOCK HF trial [Curtis AB et al. N Engl J Med 2013] in patients in need of ventricular pacing because of high degree AV block with reduced LVEF defined as LVEF <50%. CRT (BiV pacing) resulted in a relative risk reduction of 23% of HF hospitalizations and death compared with RV pacing over a 2-year follow-up.
The 2013 ESC Guidelines include updates from the 2010 Guidelines. The document provides new and updated recommendations in a novel structure that aims to enhance the reader's ability to quickly and easily identify a topic of interest.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.