

Summary
Cardiac pacing is beneficial in patients with neurally mediated syncope that have a negative tilt test, but not in those patients with a positive tilt test. This article presents data from the International Study on Syncope of Uncertain Etiology 3 registry [ISSUE-3; NCT00359203].
- Arrhythmias
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
Cardiac pacing is beneficial in patients with neurally mediated syncope (NMS) that have a negative tilt test, but not in those patients with a positive tilt test. Michele Brignole, MD, Ospedalidel Tigullio, Tigullio Lavagna, Italy, presented data from the International Study on Syncope of Uncertain Etiology 3 registry [ISSUE-3; NCT00359203].
NMS is characterized by hypotension, bradycardia, and syncope due to dysfunction of the autonomic regulation of postural tone [Zaqqa M, Massumi A. Tex Heart Inst J 2000]. Prior to the ISSUE-3 trial, the ability of pacemaker therapy to prevent syncope recurrence was controversial in patients with NMS [Brignole M et al. Circulation 2012]. The international, randomized, double-blind ISSUE-3 trial showed that cardiac pacing was able to reduce syncopal recurrence in 77 severe asystolic NMS patients randomly assigned to pacemaker ON (n=38) or to pacemaker OFF (n=39).
For the larger ISSUE-3 registry conducted in 51 centers, 504 patients with severe, recurrent reflex syncopes aged ≥40 years were initially screened for NMS and received an implantable loop recorder (ILR). Following electrocardiogram (ECG) data during a mean follow-up of 15 months, 162 out of 187 patients were determined to likely have NMS; 99 patients had asystolic NMS and 63 had hypotensive NMS. NMS was excluded in 25 patients; 21 patients had intrinsic cardiac arrhythmias and 4 had nonarrhythmic transient loss of consciousness.
Atrial tachyarrhythmia was associated with intrinsic cardiac syncope, as 38% of patients with intrinsic cardiac arrhythmias versus 5% of NMS patients had atrial tachyarrhythmias. Other multiple factors related to syncopal events and other factors, such as tilt testing, structural heart disease, hypertension, diabetes, and concomitant medications, were found not to be associated with intrinsic cardiac syncope.
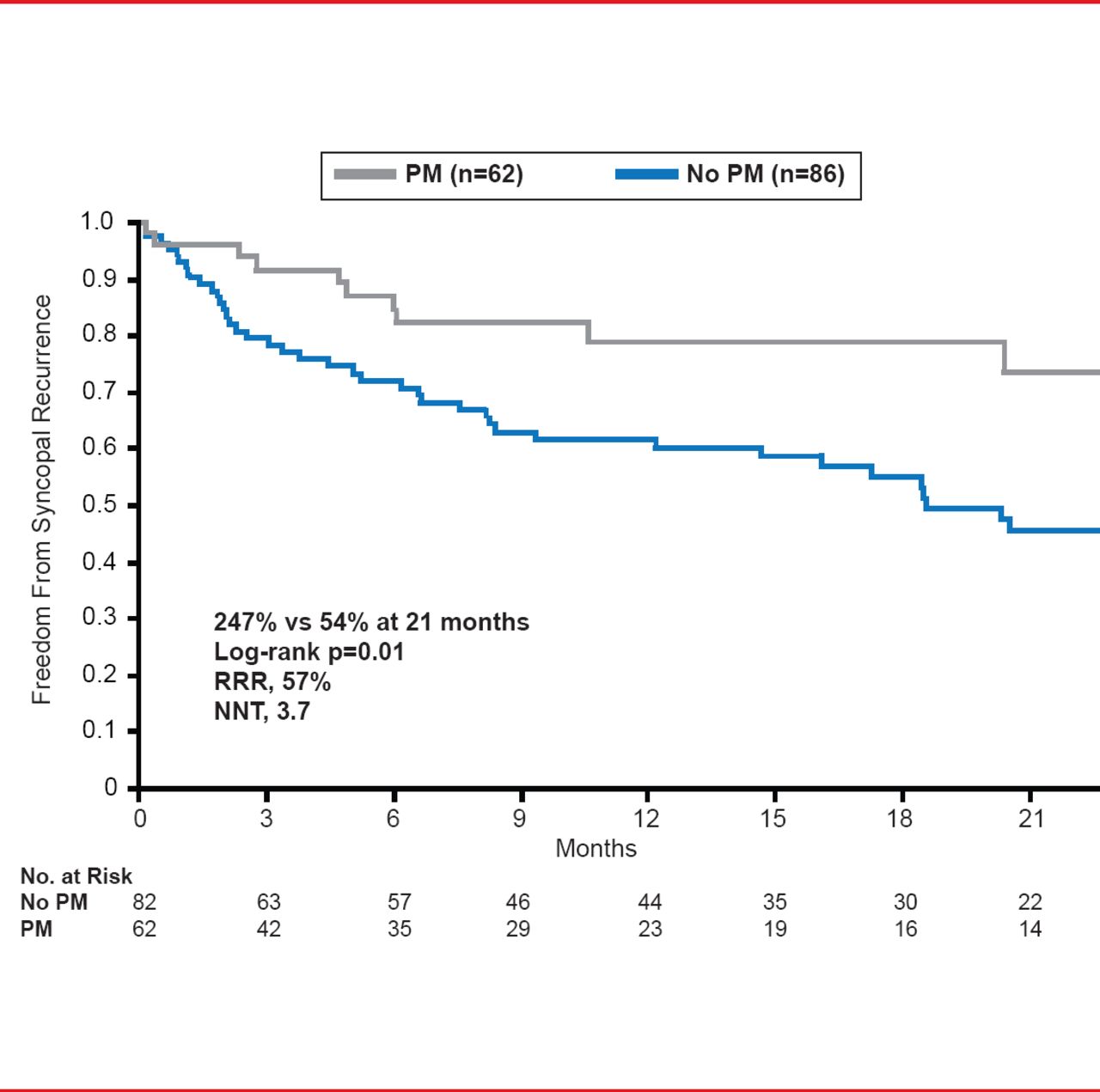
In NMS patients that received pacemaker therapy (n=62), 27% experienced recurrence of syncope, compared with 54% of NMS patients that did not receive a pacemaker at 21 months, resulting in a hazard ratio of 57% (p=0.01; Figure 1). The median total number of syncopal events was predictive of recurrence (p=0.007) and patients with ≥8 syncopal events were more likely to experience a recurrence (p=0.001).
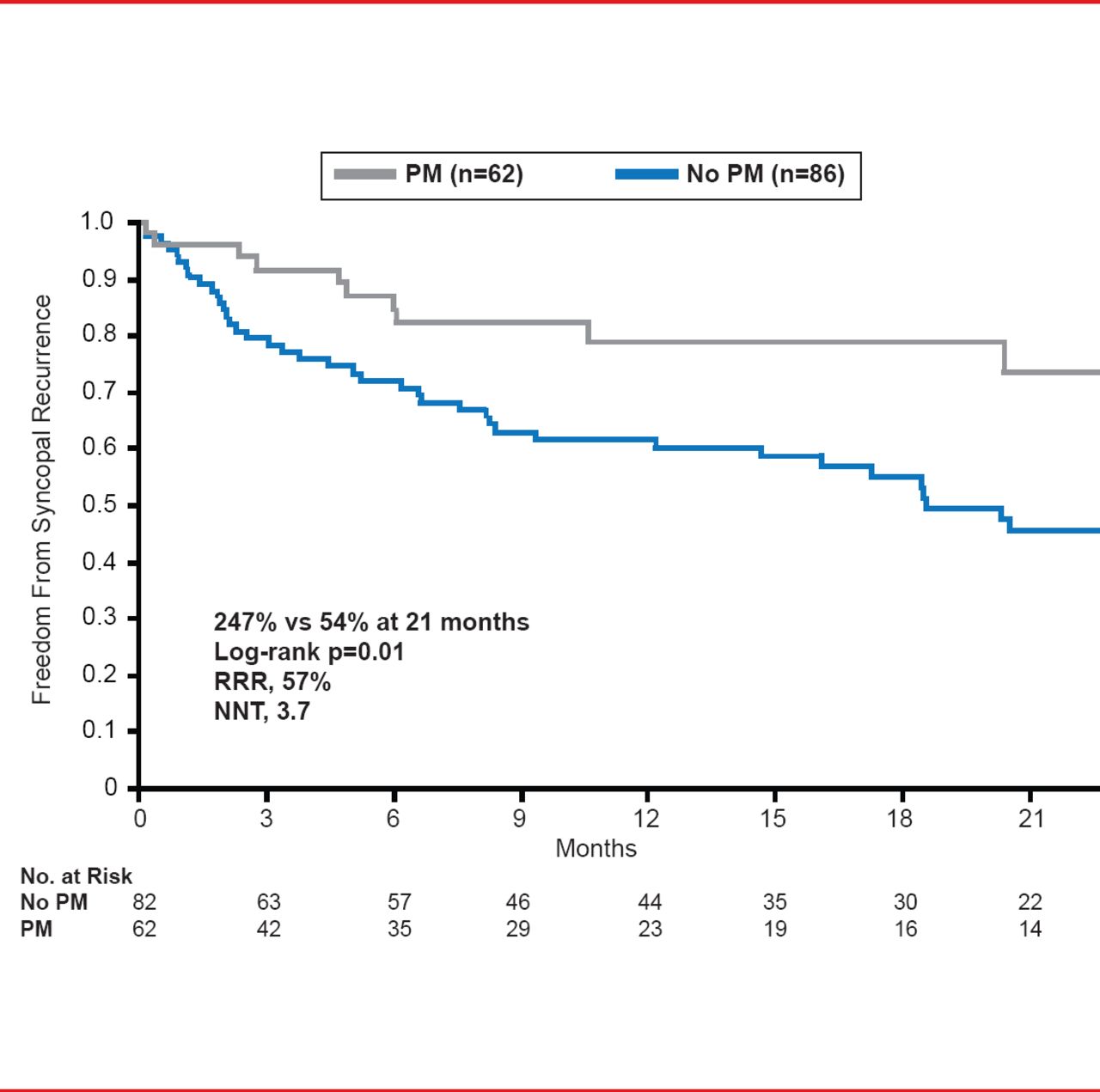
Effect of Pacemaker Therapy in Patients With NMS
Reproduced with permission from M Brignole, MD.
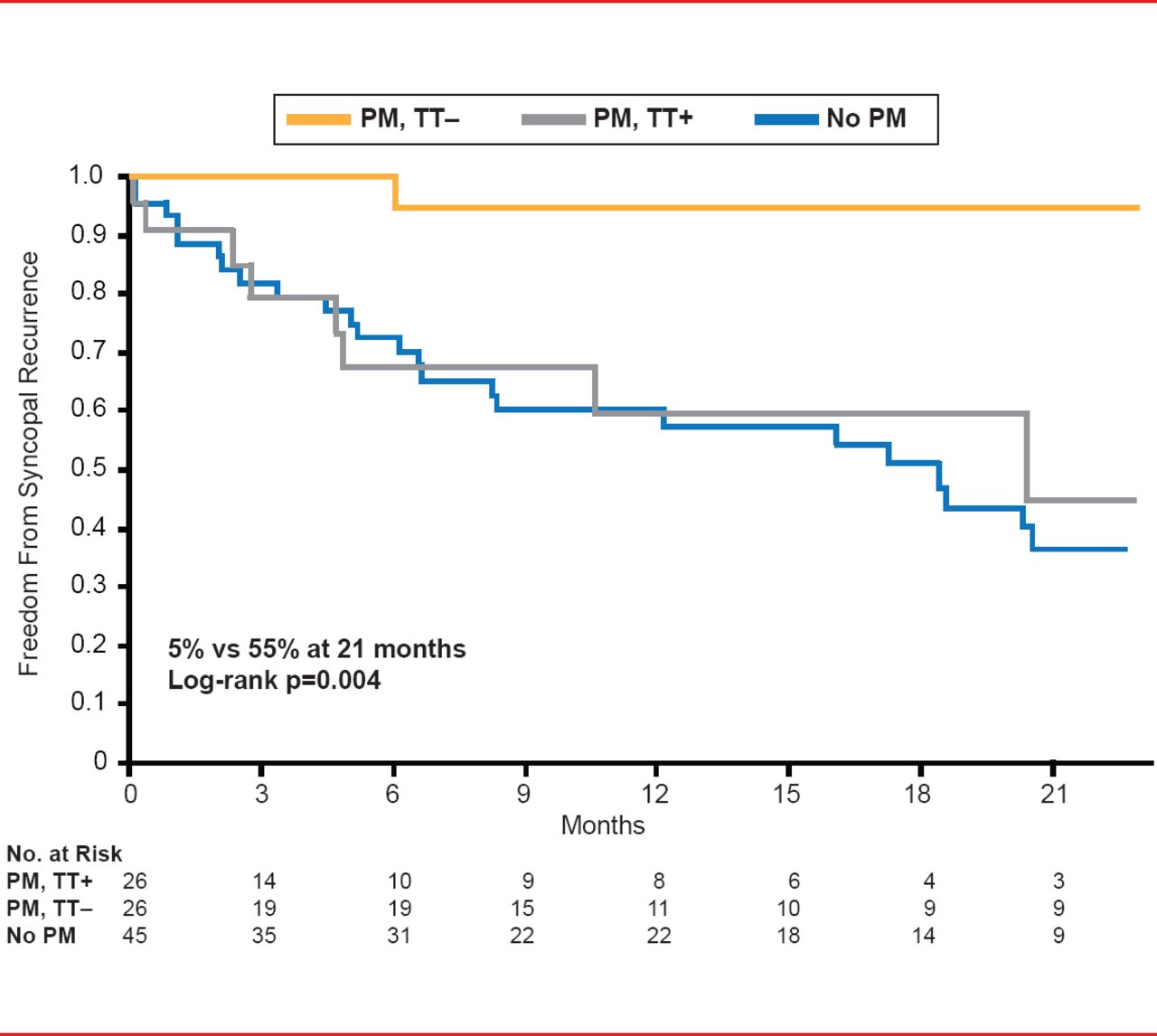
In NMS patients, a positive tilt test occurred in 89% of patients that developed recurrence compared with 42% (p=0.0004) in patients that did not develop recurrence following pacemaker therapy. In NMS patients with a pacemaker, 5% that had a negative tilt test experienced recurrence compared with 55% of patients that had a positive tilt test (p=0.004; Figure 2).
Prof. Brignole concluded that in his opinion, the data from the ISSUE-3 trial suggest that pacemaker therapy is beneficial in the subset of NMS patients that receive a negative result during the tilt test. However, cardiac pacing does not appear have efficacy in patients that have a positive tilt test.
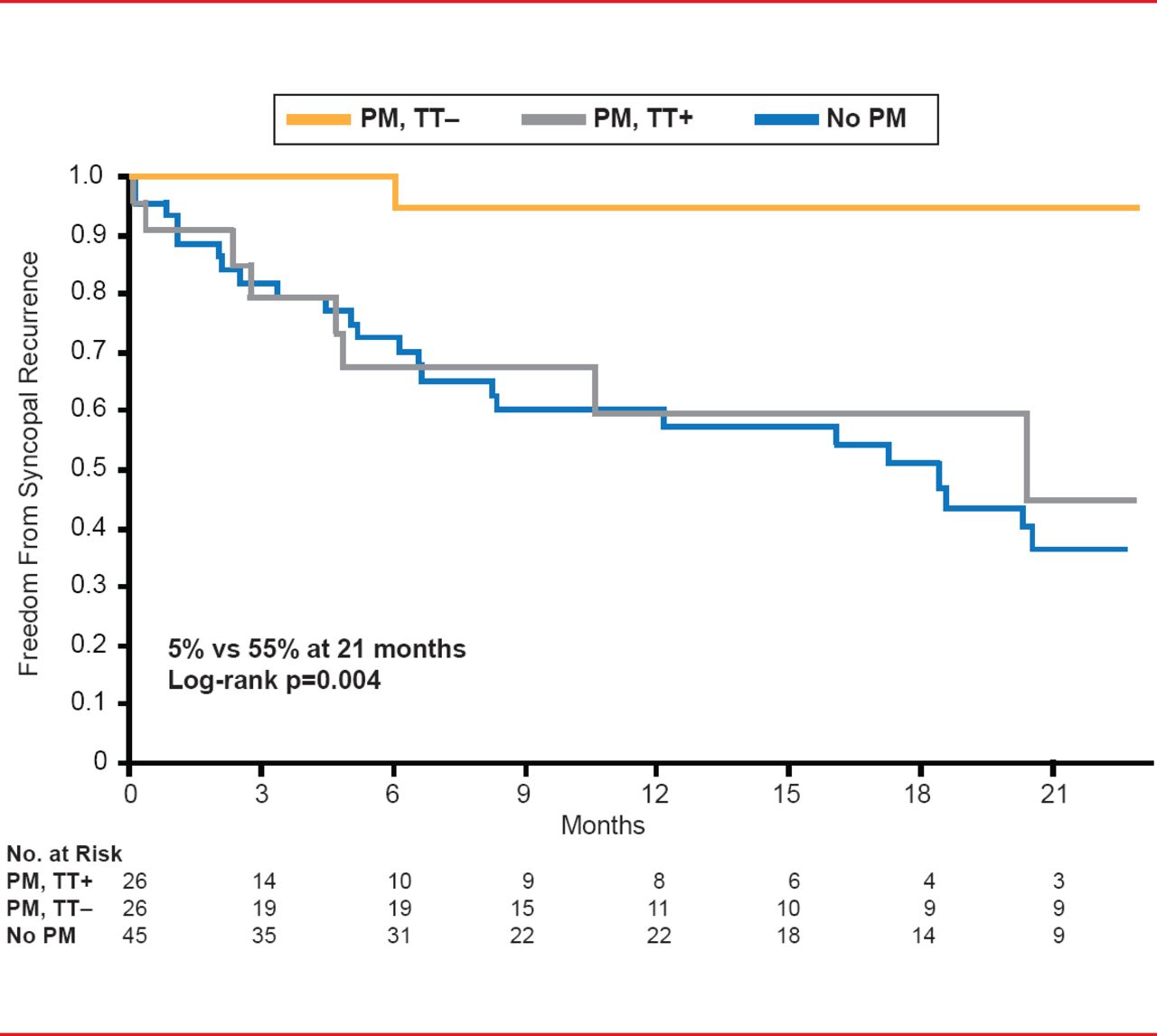
Tilt Test Results Are Predictive of Syncope Recurrence Following Pacemaker Therapy
Reproduced with permission from M Brignole, MD.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.