

Summary
All three stroke stratification scores are associated with risk of thromboembolic (TE) events in anticoagulated patients after radiofrequency catheter ablation of atrial fibrillation (AF). This article presents the information from the Incidence and Risk Factors for Thromboembolic Events After Catheter Ablation of Atrial Fibrillation: The Leipzig Heart Center AF Ablation Registry.
- Cardiology Clinical Trials
- Cerebrovascular Disease
- Thrombotic Disorders
- Arrhythmias
- Cardiology Clinical Trials
- Cerebrovascular Disease
- Thrombotic Disorders
- Cardiology & Cardiovascular Medicine
- Arrhythmias
All three stroke stratification scores are associated with risk of thromboembolic events (TE) in anticoagulated patients after radiofrequency catheter ablation of atrial fibrillation (AF). Jelena Kornej, MD, Heart Center Leipzig, Germany, presented the information from the Incidence and Risk Factors for Thromboembolic Events After Catheter Ablation of Atrial Fibrillation: The Leipzig Heart Center AF Ablation Registry.
The objective of the analysis was to report TE incidence in a large, contemporary AF ablation cohort in patients taking oral anticoagulation (OAC) therapy, and to investigate the value of renal dysfunction and of stroke risk stratification scores in predicting TE after ablation. The scores are CHADS2, CHA2DS2-VASc, and R2CHADS2. For the latter, renal dysfunction was defined as estimated glomerular filtration rate <60 mL/min.
The study population of the registry included 2069 patients between 2007 and 2011. Mean age was 60 years, 66% were males, 63% had paroxysmal AF, 71% had hypertension, but only 15% had diabetes and 14% had coronary artery disease. Mean scores were CHADS2 at 1.2, R2CHADS2 at 1.3, and CHA2DS2-VASc at 2.1.
After catheter ablation (CA) patients had outpatient visits at 3, 6, and 12 months. They also had serial 7-day Holter electrocardiogram recordings and were to present immediately if AF symptoms occurred. According to guidelines, recommended OAC treatment was based on CHADS2 scores.
A total of 15 TEs occurred during follow-up, including 5 strokes, 9 transitory ischemic attacks, and 1 system embolism. TE occurred after an average of 11 months (range, 5 to 17 months) following CA, and the international normalized ratio at time of events was 2.51 (Table 1).
In univariate analysis, peripheral artery disease, renal dysfunction, previous thromboembolic events and AF recurrences were associated with TE after catheter ablation. However, in multivariate analysis only three stroke risk stratification scores remained statistical significant predictors for TE during follow up (CHADS2 OR, 2.0; 95% CI, 1.4 to 3.0; p<0.001; R2CHADS2 OR, 1.8; 95% CI, 1.3 to 2.5; p<0.001, and CHA2DS2-VASc OR, 1.7; 95% CI, 1.2 to 2.3; p=0.001).
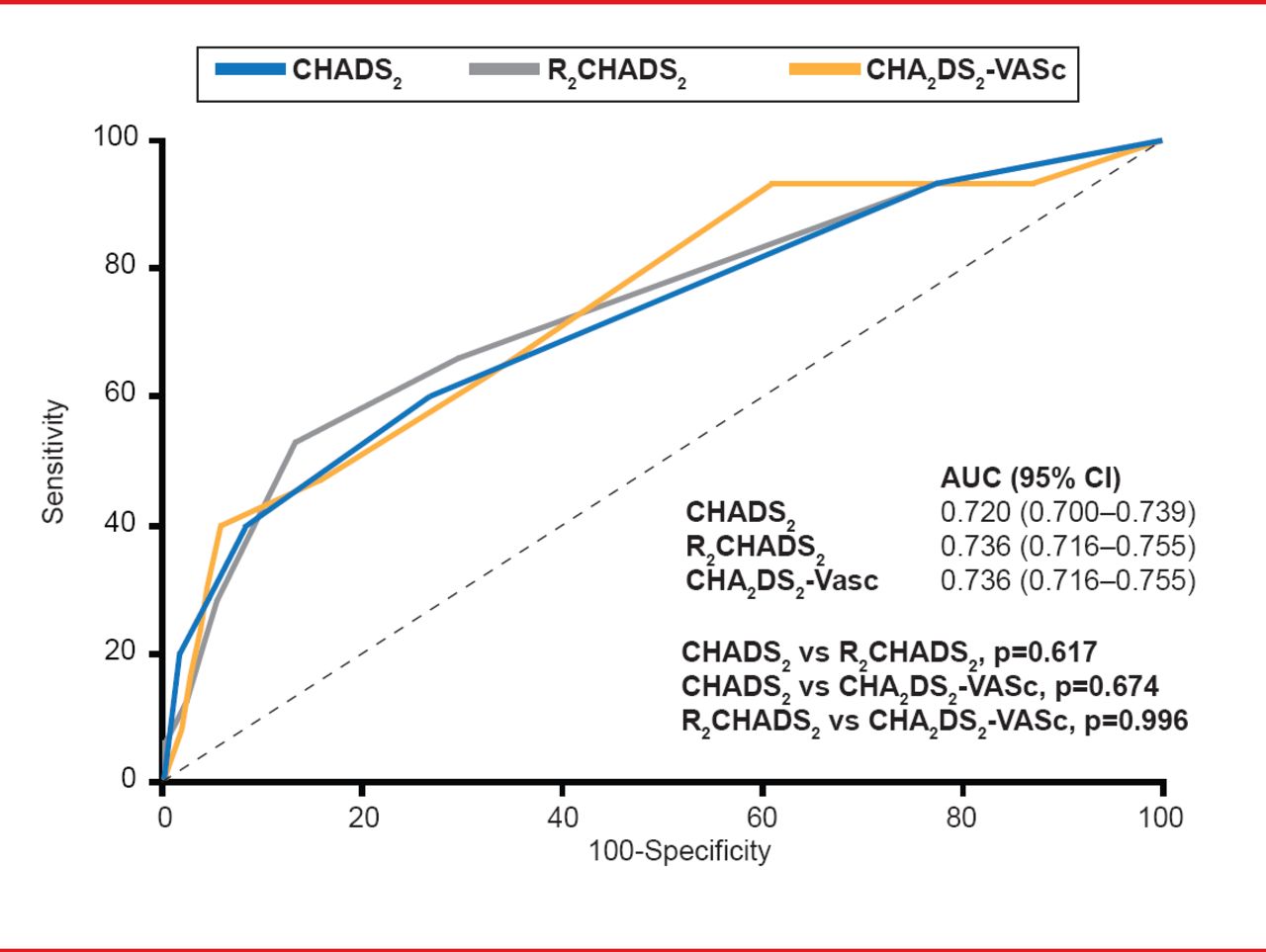
Although in the ROC curve analyses 3 stroke risk stratification scores showed modest predictive value (c-index between 0.720 and 0.736), CHA2DS2-VASc score differentiated further patients in truly low and high risk strata according to CHADS2 and R2CHADS2 of 0 to 1.
An important finding of this study was that AF recurrences conferred a nonsignificant trend for increased TE risk (p=0.056 to 0.077). In this subgroup CHA2DS2-VASc had the best predictive value compared with other scores (c-index 0.894, p=0.022 vs CHADS2, p=0.031 vs R2CHADS2; Figure 1).
Comparison of Patients With and Without Thromboembolic Events During Follow-Up

Comparison of Scores as Predictors for Thromboembolism in Patients With AF recurrences
Reproduced with permission from J Kornej, MD.
A low event rate of 0.7%, and the retrospective nature of the study and registry design were considered the most important limitations. Additionally, complete rhythm follow-up was available in 75% of the patients, whereas time of therapeutic range for patients on anticoagulation with vitamin K antagonists was not available at all.
Prof. Kornej concluded that even in anticoagulated patients all three stroke risk stratification scores are useful in predicting thromboembolic events after catheter ablation and stressed the importance to control the AF recurrences during follow up because of their association with thromboembolic complications.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.