

Summary
Patients with rheumatoid arthritis (RA), psoriatic arthritis, and ankylosing spondylitis have a higher risk of mortality from cardiovascular disease (CVD). This article discusses the impact and pathology of CVD in people with RA.
- Coronary Artery Disease
- Hypertensive Disease
- Rheumatoid Arthritis
- Diabetes Mellitus
- Featured Meeting - Specialty page
- Valvular Disease
Patients with rheumatoid arthritis (RA), psoriatic arthritis (PsA), and ankylosing spondylitis (AS) have a higher risk of mortality from cardiovascular disease (CVD). George Kitas, MD, PhD, University of Manchester, Manchester, United Kingdom, discussed the impact and pathology of CVD in people with RA.
Most CVD-related deaths in patients with RA are caused by ischemia-related issues. Stevens et al. [Expert Rev Mol Med 2005] reviewed the evidence that atherosclerosis may be accelerated in RA. Several aspects of RA can compound CVD risk factors, such as disease activity and severity, extraarticular disease, autoantibodies such as rheumatoid factor and anticitrullinated peptide antibodies, RA susceptibility genes, and choice of RA therapy.
Patients with RA have higher rates of classic CVD risk factors, including hypertension and dyslipidemia, both of which have an inflammatory component. Inflammation may also be involved in RA cachexia, which is characterized by decreased muscle mass and increased total fat mass. In addition, studies have shown that physical inactivity is highly prevalent in people with RA, which in turn is associated with vascular dysfunction and multiple CVD risk factors. John et al. [Best Pract Res Clin Rheumatol 2009] reviewed multiple interactions between classic and novel CVD risk factors.
RA treatments also affect CVD risk factors. Nonsteroidal anti-inflammatory drugs and cyclooxygenase inhibitors can cause hypertension, and steroids can lead to hypertension, dyslipidemia, and insulin resistance. Hydroxychloroquine is associated with decreased lipid levels and may lower glucose levels, and methotrexate increases homocysteine levels.
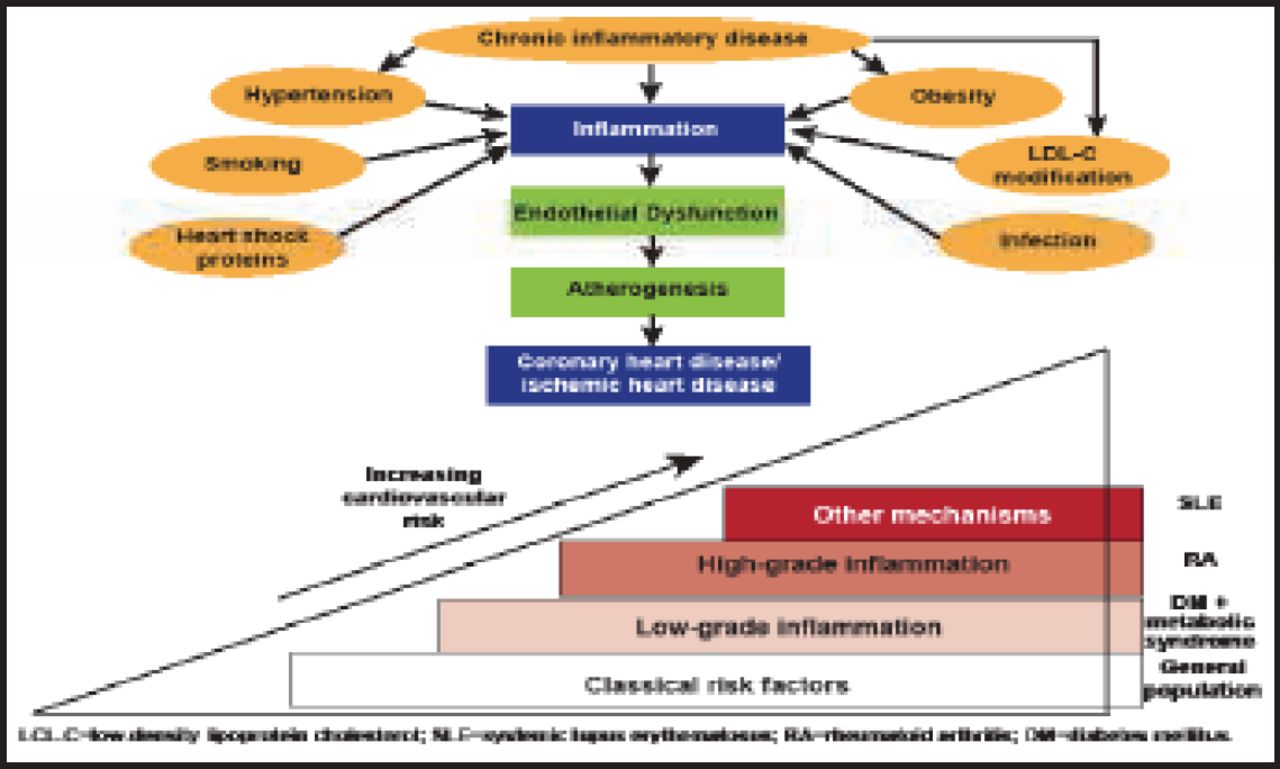
Gonzalez et al. [Ann Rheum Dis 2008] found that classic CVD risk factors imparted similar risk for the development of CVD in patients with RA compared with people without RA. Thus, disease-related risk factors may, in relative terms, play a greater role in the development of CVD than classic risk factors in patients with RA. Evidence points to inflammation as the culprit in increased CVD risk in patients with RA. Atherosclerosis and RA are chronic inflammatory disorders. Chronic inflammatory disease appears to interact with other risk factors, resulting in more inflammation that leads to endothelial dysfunction, atherogenesis, and coronary heart disease (Figure 1) [Stevens et al. Expert Rev Mol Med 2005]. Possible interventions to reduce CVD risk in patients with RA include intensive inflammation control, lifestyle interventions, and intensive management of comorbidities.
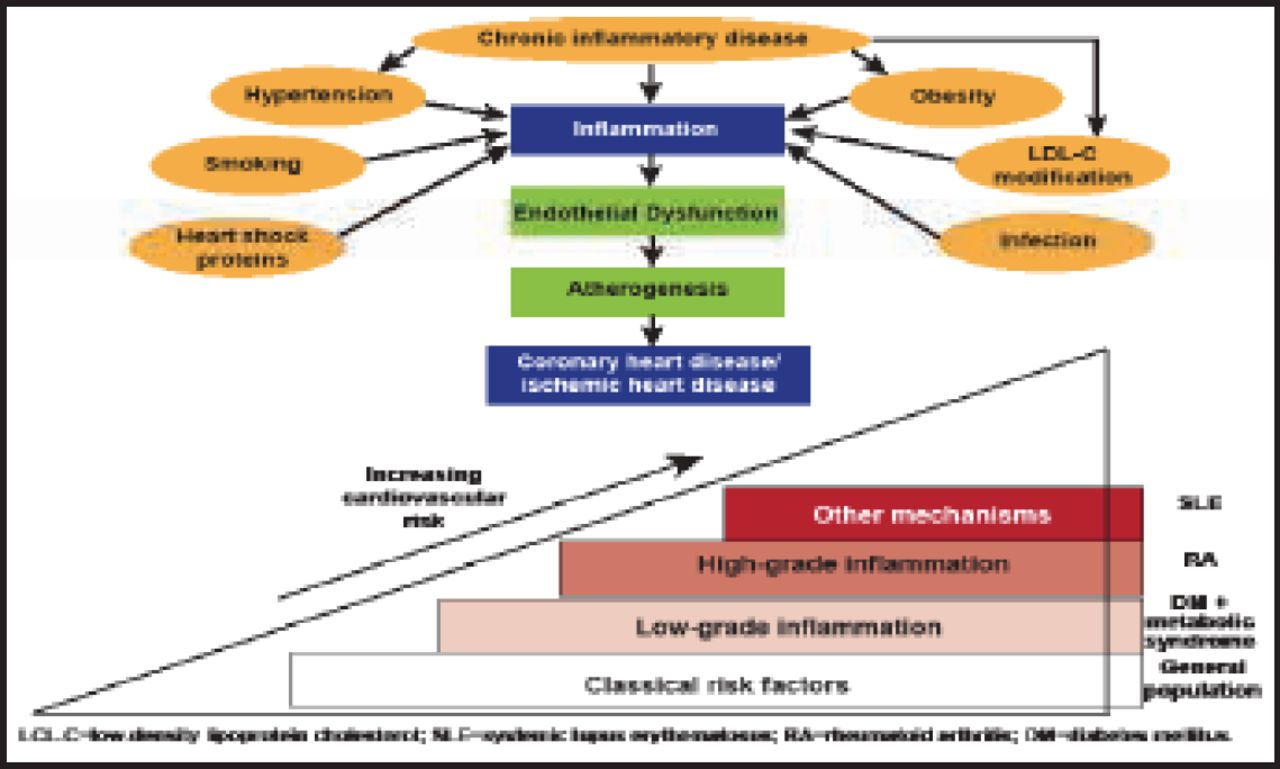
Effect of Chronic Inflammatory Disease on Risk of CVD.
Reproduced with permission from G Kitas, MD.
CVD morbidity and mortality are also increased in RA and the spondyloarthropathies because of accelerated atherosclerosis and other processes. Classic risk factors and inflammation appear to play a role in the vascular pathology of RA and the spondyloarthropathies. Multiple peculiarities of the populations and risk-factor interactions make attribution difficult. Inflammatory effects may be exerted directly, or via effects on individual classic CVD risk factors.
Cardiovascular Risk Assessment in Inflammatory Arthritis
Patients with RA have twice the risk of CVD than people without RA, and the risk may be similar in patients with AS and PsA. The inflammatory burden of RA, together with traditional CVD risk factors, imparts a CVD risk that is equal to that of patients with type 2 diabetes mellitus. Anne Meadows, MSc, Peterborough and Stamford Hospitals, United Kingdom (UK), discussed the UK national guidelines and recommendations for reducing CVD risk in patients with inflammatory arthritis. She also presented the process and results from the 2002 to 2006 nurse-led cardiovascular (CV) health screening program, conducted by the Peterborough Hospital Rheumatology Department.
The UK national guidelines recommend controlling factors that increase CVD risk in patients with inflammatory arthritis. Patients with hypertension should be treated with a goal of achieving blood pressure of <140/90 mm Hg. Ambulatory blood pressure should be monitored for 4 to 7 days, with an average of at least 14 measurements obtained. Lipid modification therapy should be initiated in patients with total cholesterol >7 mmol/L or total cholesterol-to-high-density lipoprotein ratio >6. The guidelines also recommend controlling for other risk factors, including smoking and obesity.
The Peterborough Rheumatology Department implemented a nurse-led CV screening and assessment program from 2002 to 2006 among patients with RA. The aim of the program was to obtain optimum control of inflammatory arthritis with appropriate treatment, encourage a healthy lifestyle, advise patients about their health, and treat conventional risk factors. Patients who ranged in age from 45 to 60 years were screened during a 45-minute appointment when they completed a lifestyle questionnaire about diet, smoking, alcohol consumption, and exercise. Medical tests, including blood pressure, body mass index, lipid profiles, inflammatory markers, chest x-ray, and urine glucose tests, were performed. Following the screening, patients were engaged in a lifestyle improvement discussion and provided with multidisciplinary and smoking cessation referrals. Letters with screening results were sent to the patients and to their general practitioners (GPs) with advice for further investigation. The patients were seen again at 6 months and 12 months.
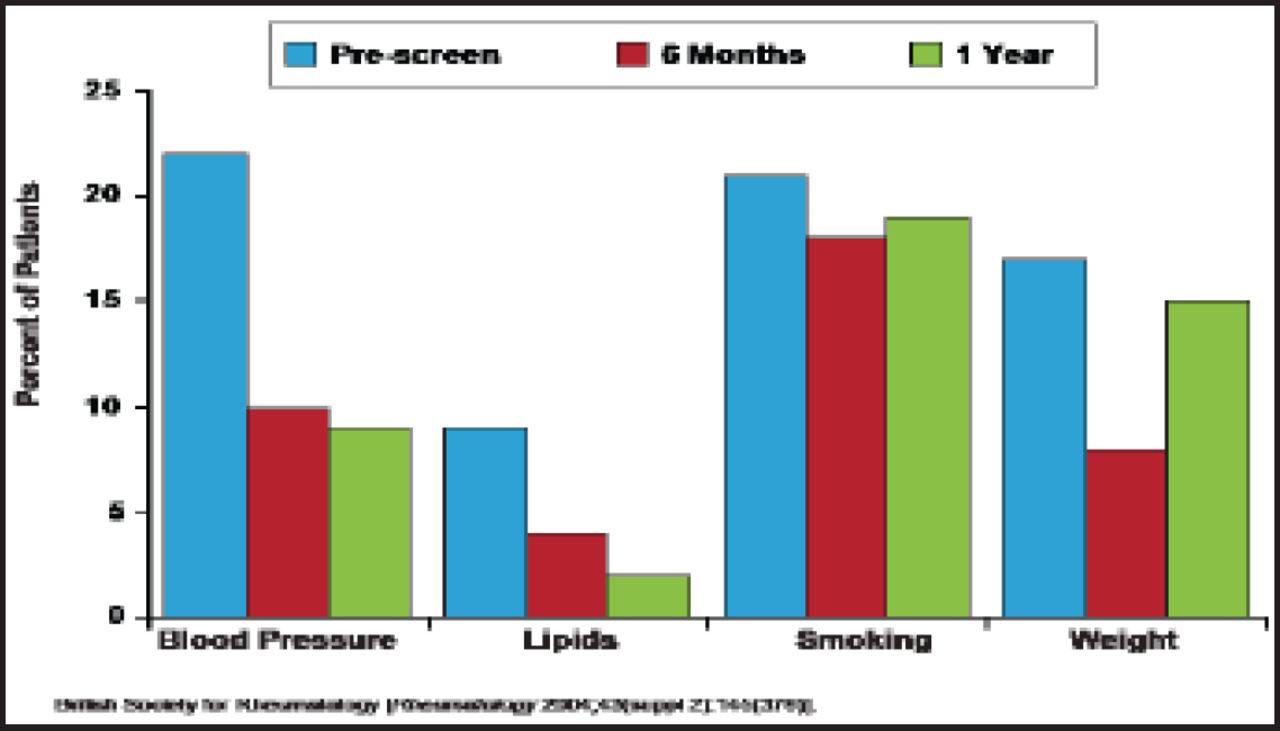
Of the 130 patients who were seen, 45 had CVD risk factors. At the 6- and 12-month follow-up visits, blood pressure and lipid levels were reduced (Figure 2). Although smoking and weight decreased initially, the patients returned to prescreening levels at 12 months. No change in exercise levels was observed. Based on these results, the authors concluded that lifestyle modification changes (smoking, weight control) could not be sustained over the observation period but that pharmacologically treatable risk factors (hypertension, hyperlipidemia) were more easily addressed.
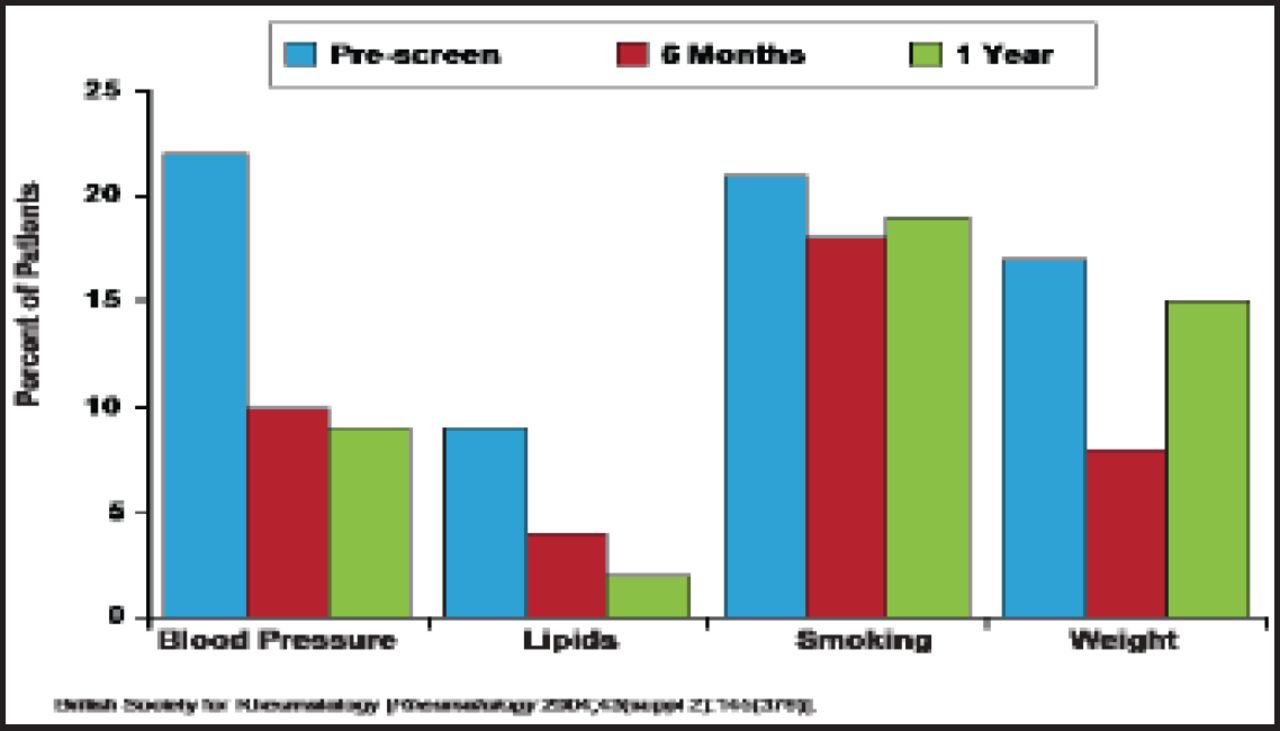
Nurse-Led CV Health Screening Audit Results.
Reproduced with permission from A. Meadows, MSc.
Challenges to the screening program included the availability of only 1 nurse specialist, time constraints, lack of a dedicated physiotherapist and occupational therapist, GPs' lack of information on risks and treatment, and lack of funding initiatives for GPs. Currently, CVD screening in Peterborough follows the National Institute for Health and Clinical Excellence 2009 RA management guidelines and is performed within the clinic by the rheumatology team, with an annual review. GPs are informed of any required follow-up, and patients are educated at each visit. Patients are referred for specific aerobic exercise and conditioning advice, with involvement of a dedicated physiotherapist and occupational therapist.
Ms. Meadows concluded that applying this process in routine practice is not easy but can be done. Screening and assessment for CVD risk in people with RA are evolving processes and require health care team compliance. Annual reviews of the process should be ongoing. The service is to be audited and, if successful, will be rolled out to include all types of inflammatory arthritis, rather than just RA.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.