

Summary
Contractile reserve and echocardiographic dyssynchrony predict early response to cardiac resynchronizatiuon therapy, according to findings from the Risk Stratification and Benefits with Cardiac Resynchronization Therapy trial [BENEFIT; NCT00996086], according to outcomes from the BENEFIT study.
- Interventional Techniques & Devices
- Arrhythmias Clinical Trials
Contractile reserve and echocardiographic dyssynchrony predict early response to cardiac resynchronizatiuon therapy (CRT), according to findings from the Risk Stratification and Benefits with Cardiac Resynchronization Therapy trial [BENEFIT; NCT00996086]. John Gorcsan, MD, University of Pittsburgh, Pittsburgh, Pennsylvania, USA, presented outcomes from the study.
The BENEFIT Trial was a multicenter, prospective, longitudinal study to identify clinical and echocardiographic factors that predict response to CRT. Dr. Gorcsan noted that response to CRT is multifactorial and may be influenced by clinical, procedural, and echocardiographic variables. The objective of the BENEFIT study was to test the hypothesis that contractile reserve, assessed by low-dose dobutamine echo and echo-Doppler dyssynchrony, predicts clinical response to CRT and reverse remodeling.
The study enrolled a total of 227 patients from 26 sites. Their mean age was 65±12 years (29% female), and all had New York Heart Association (NYHA) Class III-IV heart failure with QRS duration 157±24 ms (all ≥120 ms) and ejection fraction 29%±9% (all ≤35%); 52% had ischemic heart disease.
Prespecified cutoffs were used to assess contractile reserve, dyssynchrony, and speckle tracking radial strain for septal to posterior wall delay. Contractile reserve was determined by low-dose dobutamine echo wall motion score (WMS); the cutoff was an increase in WMS ≥0.2 with 10 μg/kg per min. Dyssynchrony was determined by Doppler pre-ejection delay (PED); the cutoff was ≥140 ms. The cutoff for speckle tracking radial strain for septal to posterior wall delay was ≥130 ms.
Three predefined CRT response endpoints were assessed at 6 months: improvement in NYHA class ≥ 1, increase in 6-min walk distance ≥10%, and decrease in end-systolic volume (ESV) ≥10%. Of 190 patients with 6-month follow-up available, 83% were a CRT responder by at least 1 criterion; 51% improved NYHA class; 47% improved 6-minute walk test; and 54% improved ESV.
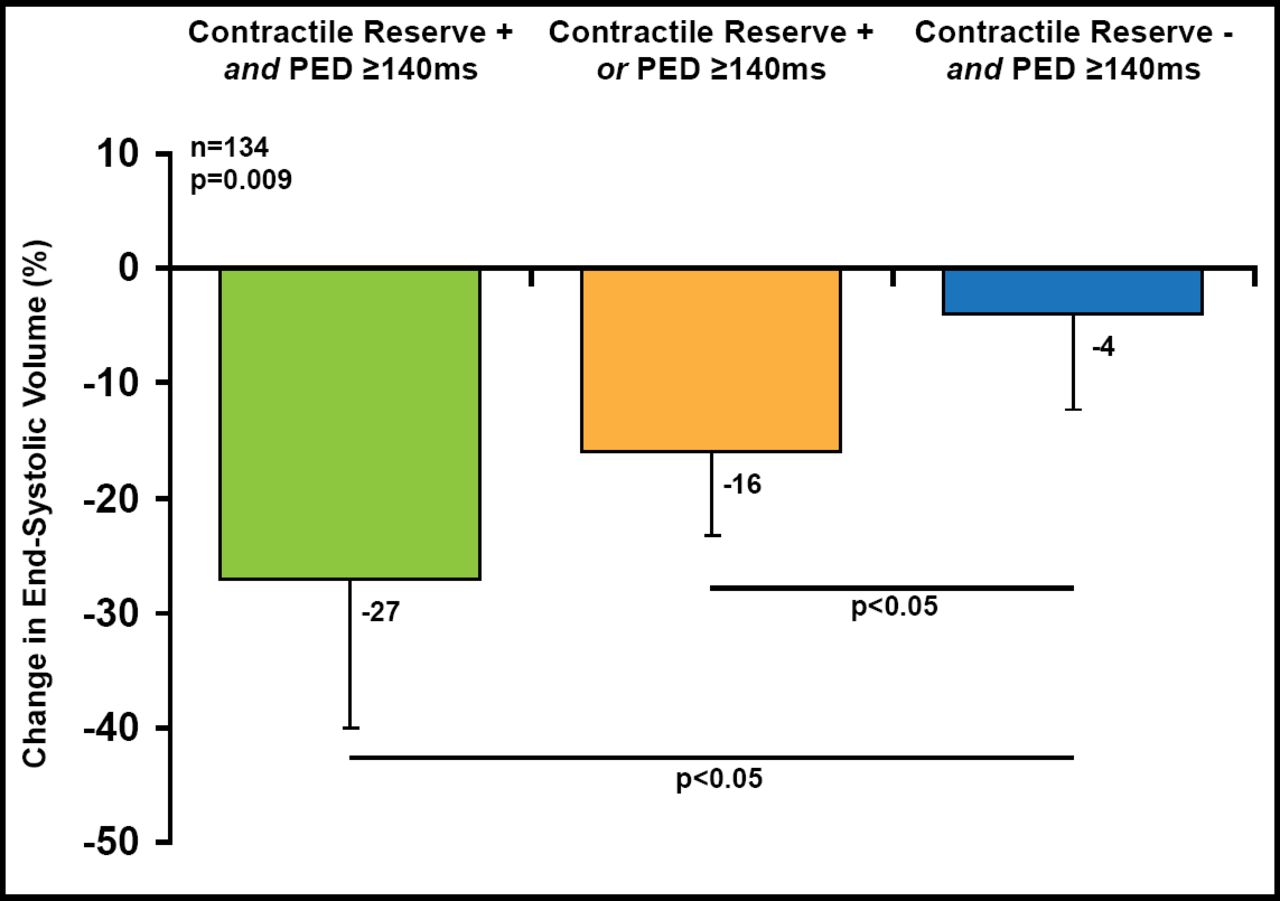
Univariate analysis of 20 clinical and echo variables, PED, septal to posterior wall delay, and creatinine predicted both clinical and ESV response (all p<0.019). Of 134 patients with paired baseline and 6-month echocardiographs, contractile reserve and PED were additive in predicting ESV response (p=0.009; Figure 1). A forward multivariate model showed that contractile reserve, dyssynchrony by PED, and creatinine remained significantly associated with both clinical and ESV CRT response.
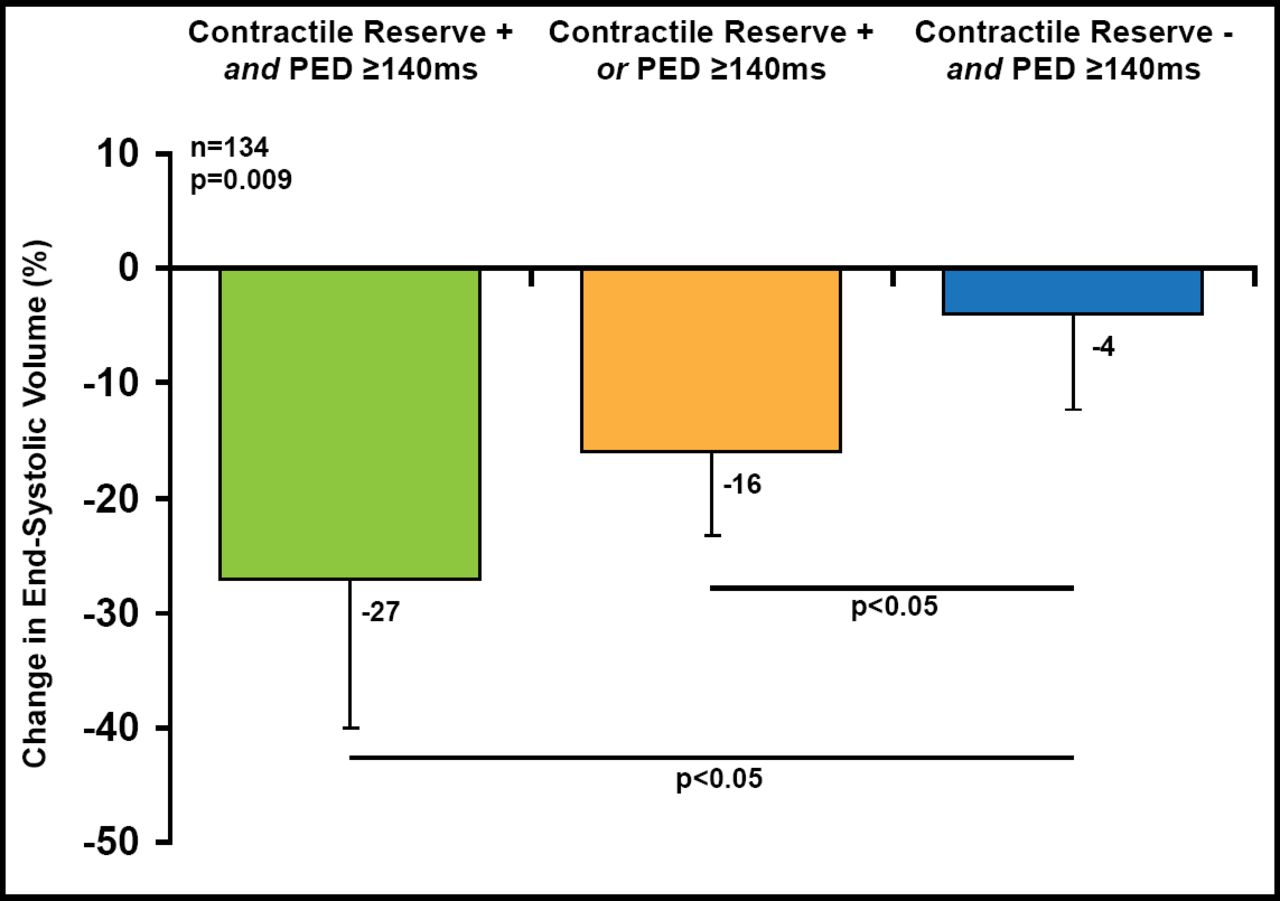
Left Ventricular Reverse Remodeling at 6 Months.
PED=pre-ejection delay.
Reproduced with permission from J. Gorcsan, MD.
Contractile reserve by low-dose dobutamine echo and dyssynchrony by routine echo-Doppler are significantly associated with early clinical and reverse remodeling CRT response. These observations have important prognostic clinical implications.
However, a study of patients who are randomized to CRT, based on echocardiographic dyssynchrony, has yet to be carried out. This makes it difficult to assign a cause-and-effect relationship with certainty. Although it is logical that echocardiographic indices of dyssynchrony can be strongly associated with outcome after CRT, most believe that it is premature to change patient selection for CRT to imaging-based echocardiographic criteria at the present time [Gorcsan J & Prinzen FW. Heart Rhythm 2012].
- © 2012 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.