

Summary
Recent studies suggest that pulmonary vein isolation with radiofrequency ablation may significantly reduce the time to first recurrence and the burden of atrial fibrillation (AF) compared with antiarrhythmic drug (AAD) therapy in patients with paroxysmal AF. The primary objective of the Radiofrequency Ablation versus Antiarrhythmic Drugs for Atrial Fibrillation Treatment-2 study [RAAFT-2; NCT00392054] was to assess if catheter-based PVI isolation is superior to AADs as first-line therapy in patients with symptomatic paroxysmal recurrent AF who were not previously treated with therapeutic doses of AADs.
- Interventional Radiology Clinical Trials
- Arrhythmias
- Interventional Techniques & Devices
Recent studies suggest that pulmonary vein isolation (PVI) with radiofrequency (RF) ablation may significantly reduce the time to first recurrence and the burden of atrial fibrillation (AF) compared with antiarrhythmic drug (AAD) therapy in patients with paroxysmal AF. The primary objective of the Radiofrequency Ablation versus Antiarrhythmic Drugs for Atrial Fibrillation Treatment-2 study [RAAFT-2; NCT00392054] was to assess if catheter-based PVI isolation is superior to AADs as first-line therapy in patients with symptomatic paroxysmal recurrent AF who were not previously treated with therapeutic doses of AADs. Carlos A. Morillo, MD, McMaster University and Hamilton Health Sciences, Hamilton, Ontario, Canada, presented recent findings.
A total of 127 patients were randomly assigned to ablation (n=66) or AAD therapy (n=61) and monitored for 21 months. The primary efficacy outcome was time to first recurrence of symptomatic or asymptomatic AF, atrial flutter (AFL), or atrial tachyarrhythmia (AT). The primary safety outcome was time to first occurrence of any event in a cluster of serious complications that occur in patients in the ablation arm.
Ablation was performed in 65 (98.5%) patients, and AADs were started in 60 (98.4%) patients. Ablation was performed in 3 (4.9%) patients in the AAD arm during the treatment period. In the ablation arm, 7 (10.6%) patients started an AAD during the follow-up period.
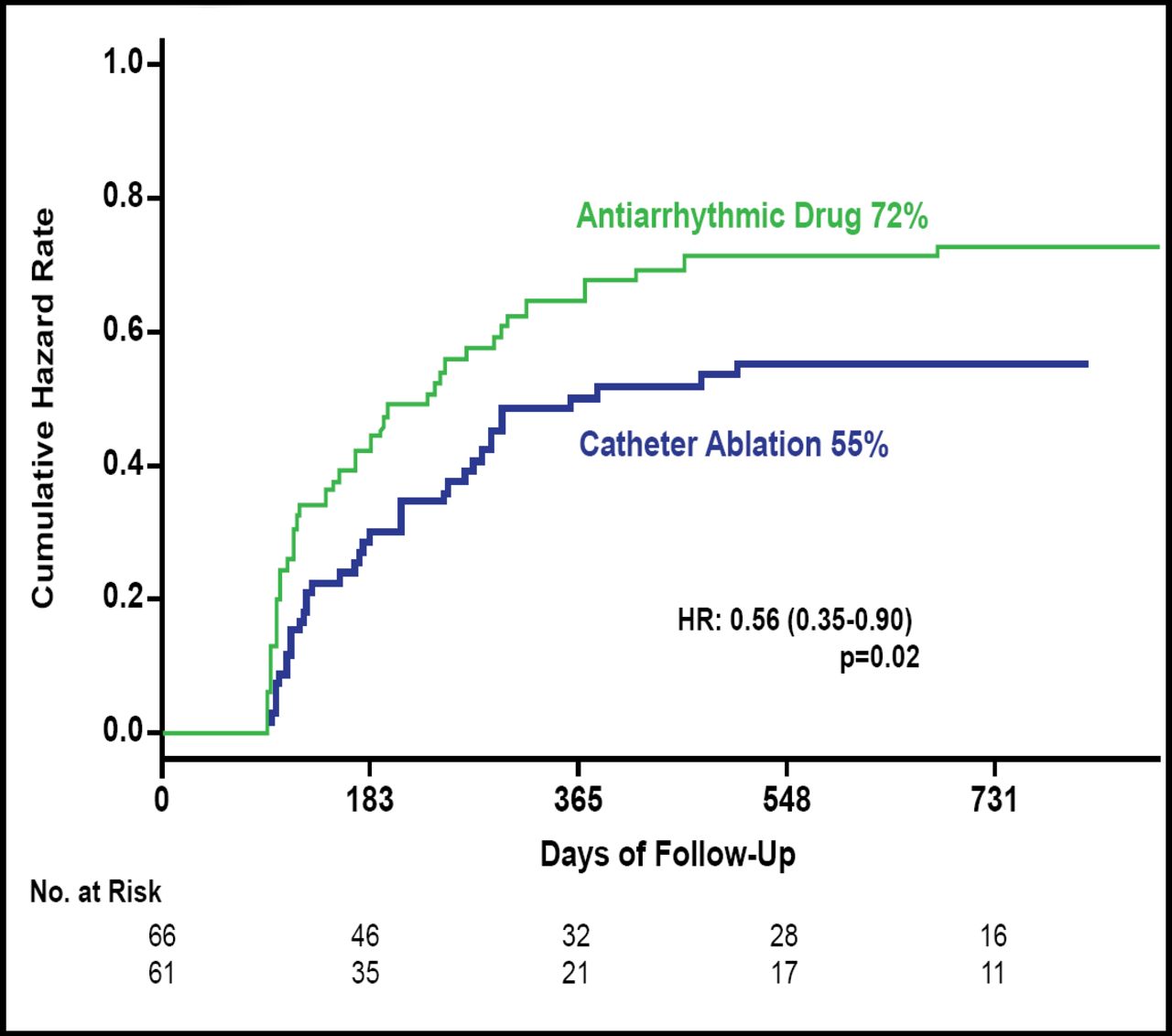
The primary efficacy outcome was reached in 72% of patients in the AAD arm versus 55% of patients in the ablation arm (HR, 0.56; 95% CI, 0.35 to 0.90; p=0.02; Figure 1). Recurrence of symptomatic AF, AT, or AFL occurred in 59% of patients in the AAD arm versus 47% in the ablation arm (HR, 0.56; 95% CI, 0.33 to 0.95; p=0.03), while symptomatic AF occurred in 58% of patients in the AAD arm versus 41% in the ablation arm (HR, 0.52; 95% CI, 0.30 to 0.89; p=0.01). Recurrence of multiple primary outcome events using a recurrence event model was reached by 14.7% of patients in the AAD arm versus 6.6% in the ablation arm (HR, 0.33; 95% CI, 0.28 to 0.40; p=0.0001).
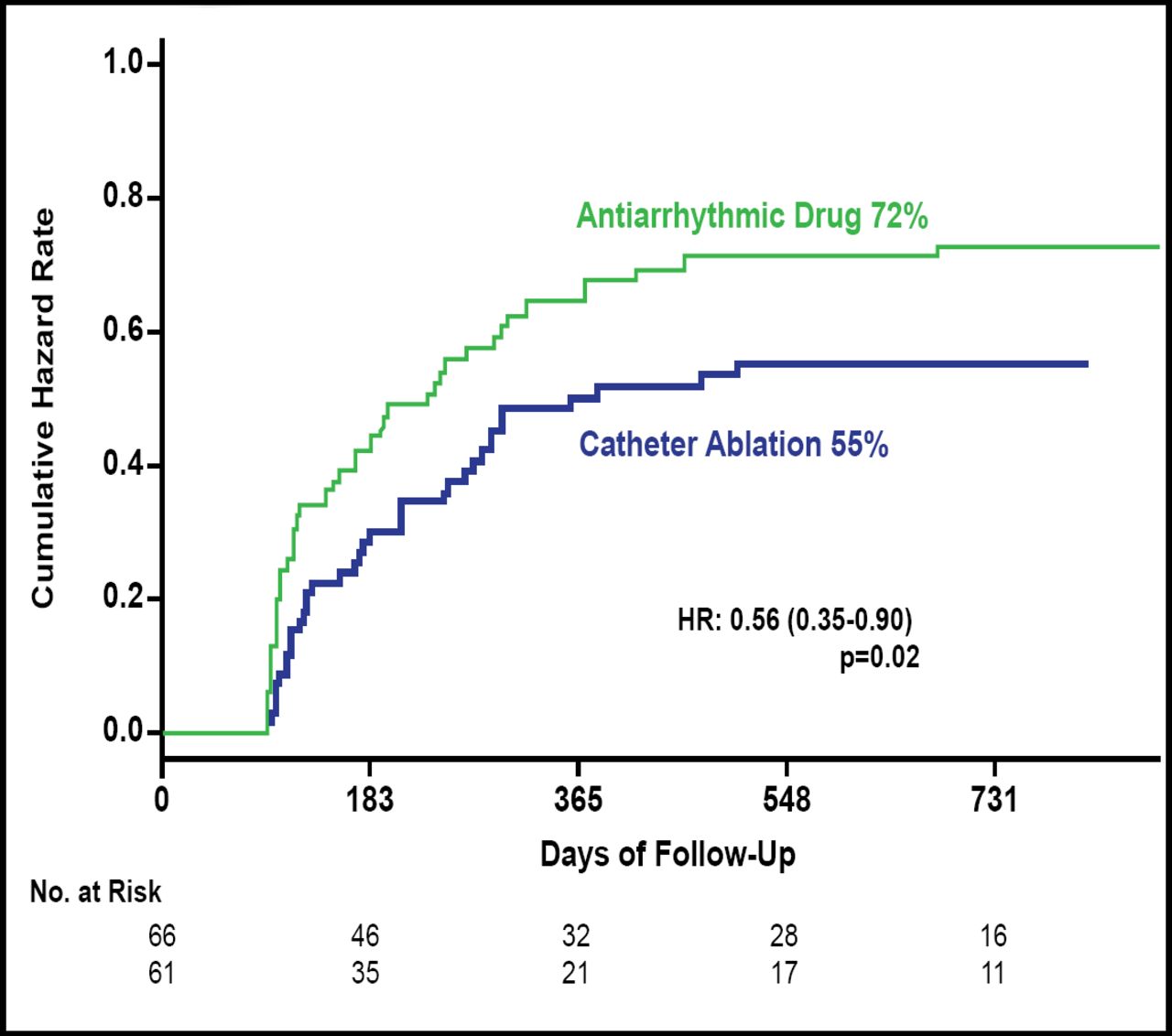
Primary Efficacy Outcome.
Reproduced with permission from C. Morillo, MD.
The primary safety endpoint was reached by 19.7% of patients in the AAD arm compared with 7.7% of patients in the ablation arm (Table 1).
Primary Safety Endpoint.
Dr. Morillo concluded that RF catheter PVI ablation is safe and significantly superior to AAD therapy in preventing the recurrence of symptomatic or asymptomatic AF, AFL, or AT in patients with paroxysmal AF, with a relative risk reduction of 44%. These results support the indication of RF PVI as first-line therapy for patients with paroxysmal AF.

The editors would like to thank the many members of the Heart Rhythm Society presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2012 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.