

Summary
The fastest growing area of interventional cardiology is structural interventions, especially for aortic valve stenosis (transcatheter aortic valve replacement) and mitral regurgitation (mitral clipping) [Meier P, Timmis A. Heart 2012]. In total, the number of valve procedures has increased over 30% from a total of 149,407 in 2006 to 194,254 in 2010 [Stuge O, Liddicoat J. J Thorac Cardiovasc Surg 2006]. This article discusses the present status and future direction of interventional mitral valve therapies.
- Arrhythmias
- Interventional Techniques & Devices
- Valvular Disease
The Complex Landscape of Interventional Mitral Valve Therapies
The fastest growing area of interventional cardiology is structural interventions, especially for aortic valve stenosis (transcatheter aortic valve replacement [TAVR]) and mitral regurgitation (mitral clipping) [Meier P, Timmis A. Heart 2012]. In total, the number of valve procedures has increased over 30% from a total of 149,407 in 2006 to 194,254 in 2010 [Stuge O, Liddicoat J. J Thorac Cardiovasc Surg 2006]. Ted E. Feldman, MD, Evanston Hospital, Evanston, Illinois, USA, discussed the present status and future direction of interventional mitral valve therapies.
The Pivotal Study of a Percutaneous Mitral Valve Repair System [EVEREST II; NCT00209274], a multicenter, randomized, controlled trial has shown different results. Feldman et al. [N Engl J Med 2011] reported that at 12 months, the rates for the primary end point for efficacy were 55% in the percutaneous-repair group and 73% in the surgery group (p=0.007). The respective rates of the components of the primary end point were as follows: death, 6% in each group; surgery for mitral-valve dysfunction, 20% versus 2%; and grade 3+ or 4+ mitral regurgitation, 21% versus 20%. Major adverse events occurred in 15% of patients in the percutaneous-repair group and 48% of patients in the surgery group at 30 days (p<0.001). At 12 months, both groups had improved left ventricular size, NYHA functional class, and quality of life measures as compared with baseline.
Recently the EVEREST investigators have undertaken a further observational study in 78 older patients at high risk for conventional surgery. The MitraClip device reduced mitral regurgitation and led to significant left ventricular reverse remodeling in the majority of patients over 12 months. This was associated with ∼54% reduction of the annual rate of rehospitalization for heart failure (p=0.034) [Whitlow PL et al. J Am Coll Cardiol 2012].
According to Dr. Feldman, a number of percutaneous mitral repair devices are still under development, including leaflet repair, coronary sinus annuloplasty, direct annuloplasty, cerclage, mitral spacer, chordal replacement, and valve replacement.
Will Transcatheter Left Atrial Appendage Closure Transform Management of Atrial Fibrillation?
Vivek Y. Reddy, MD, Mount Sinai School of Medicine, New York, New York, USA, discussed the effect of transcatheter left atrial appendage (LAA) closure on the management of atrial fibrillation (AF). He started by reviewing the difficulties with warfarin use, including a narrow therapeutic profile, drug/diet interactions, physician reluctance to prescribe to elderly patients, and difficulties with compliance.
Kirley et al. [Circ Cardiovasc Qual Outcomes 2012] found that between 2007 and 2011, warfarin treatment visits declined from ∼2.1 million to ∼1.6 million quarterly visits. Dabigatran use increased from 0.062 million quarterly visits (2010 Q4) to 0.363 visits (2011 Q4), reflecting its increasing share of oral anticoagulant visits from 3.1% to 18.9%.
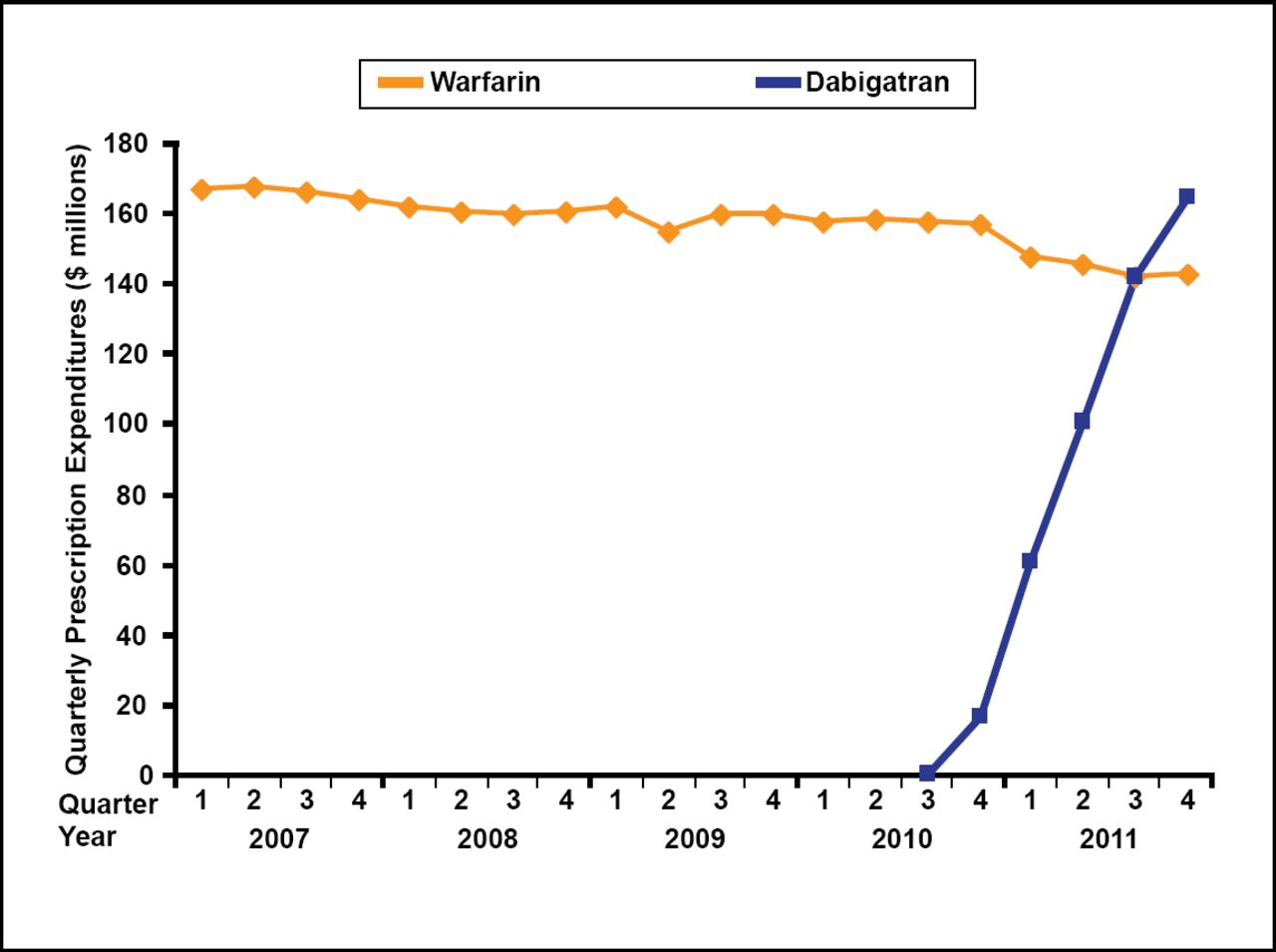
The majority of dabigatran visits were for AF, though this proportion decreased from 92% (2010 Q4) to 63% (2011 Q4), with concomitant growth in dabigatran's off-label use. Among AF visits, warfarin use decreased from 55.8% visits (2010 Q4) to 44.4% (2011 Q4), whereas dabigatran use climbed from 4.0% to 16.9%. Expenditures related to dabigatran increased from $16 million in 2010 Q4 to $166 million in 2011 Q4, exceeding those for warfarin ($144 million) in 2011 Q4 (Figure 1).
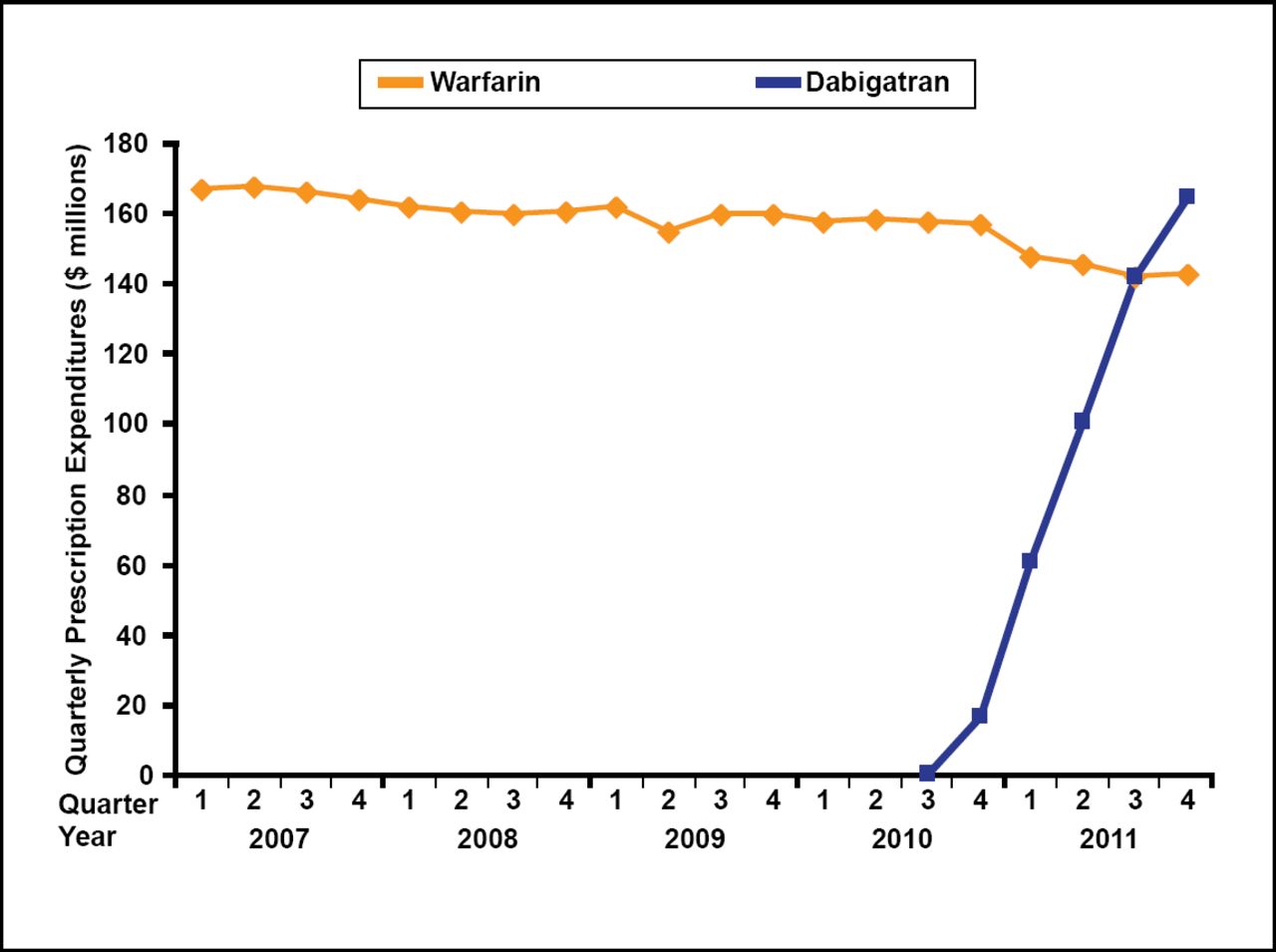
Quarterly Prescription Expenditures (2007 to 2011).
Kirley K et al. National trends in oral anticoagulant use in the United States, 2007 to 2011. Circ Cardiovasc Qual Outcomes 2012;5(5):615–621.
Kirley et al. [Circ Cardiovasc Qual Outcomes 2012] concluded that ambulatory practice in the United States has rapidly adopted dabigatran, primarily for the treatment of AF and increasingly for off-label indications. The researchers found no evidence of increased overall AF treatment.
Dr. Reddy also reviewed findings from the WATCHMAN Left Atrial Appendage System for Embolic Protection in Patients with Atrial Fibrillation [PROTECT-AF] trial, a randomized, multicenter, noninferiority trial of the efficacy and safety of percutaneous closure of the LAA for prevention of stroke compared with warfarin treatment in patients with AF.
With 1065 patient-years of follow-up, the primary efficacy event rate occurred in 3.0 per 100 patient-years (95% CI, 1.9 to 4.5) in the intervention group and 4.9 per 100 patient-years (2.8 to 7.1) in the control group (RR, 0.62; 95% CI, 0.35 to 1.25). The probability of noninferiority of the intervention was more than 99.9% [Holmes DR et al. Lancet 2009]. For the primary safety endpoint (combining major bleeding, pericardial effusion, and device embolization), event rates were significantly higher in the intervention group than in the control group (7.4% vs 4.4% per 100 patient-years, respectively; RR, 1.69; 95% CI, 1.01 to 3.19).
Based on the data, Dr. Reddy concluded that PROTECT-AF demonstrated that AF is not simply a risk marker for stroke but, rather, a risk factor, and local therapy with the LAA closure is as effective as systemic therapy with warfarin and its optimal role in the management of AF remains to be further defined.

The editors would like to thank the many members of the Transcatheter Cardiovascular Therapeutics presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.