

Summary
Hypertension is present in more than two-thirds of patients with type 2 diabetes and its development can precede and predict the development of hyperglycemia, while impaired glucose tolerance can predict the development of hypertension. This article presents an overview of the comorbidity problems associated with hypertension and diabetes.
- Hypertensive Disease
- Hyperglycemia/Hypoglycemia
- Diabetes Mellitus
Hypertension is present in more than two-thirds of patients with type 2 diabetes and its development can precede and predict the development of hyperglycemia, while impaired glucose tolerance can predict the development of hypertension. William C. Cushman, MD, Veterans Affairs Medical Center and University of Tennessee, Memphis, Tennessee, USA, presented an overview of the comorbidity problems associated with hypertension and diabetes.
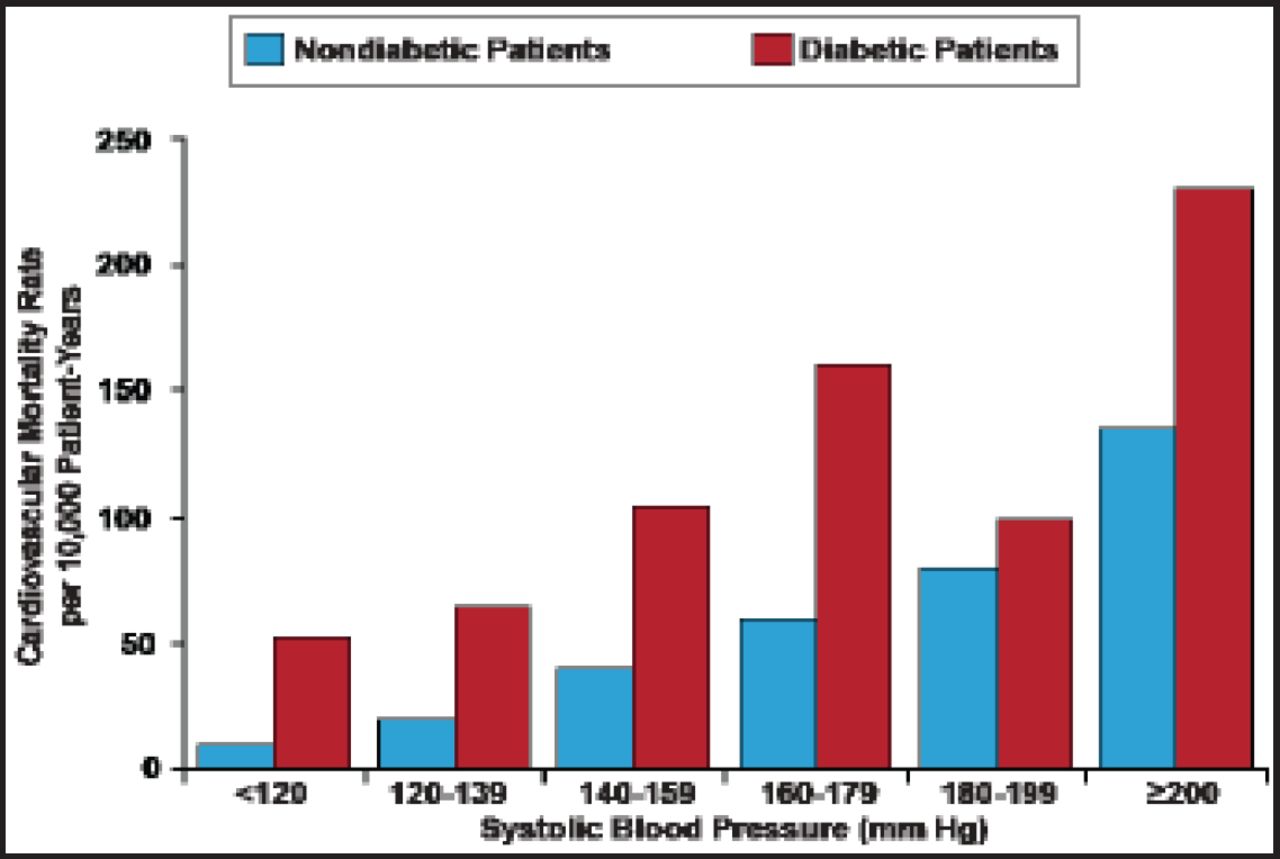
Together diabetes and hypertension increase the risk of cardiovascular (CV)-related death in men 4- to 6-fold [Stamler J et al. Diabetes Care 1993] (Figure 1). Although it is generally agreed that reducing blood pressure (BP) is desirable, the exact target goal is in question. In one large study (n=4733), diabetic patients were randomized to intensive therapy (target systolic BP <120 mm Hg) or standard therapy (target systolic BP<140 mm Hg). Patients treated to the lower systolic BP goal did not experience a reduced rate of a composite outcome of fatal and nonfatal major CV events compared with the standard therapy [Cushman WC et al. N Engl J Med 2010]. In Dr. Cushman's opinion a BP ≤140/85 mm Hg is a reasonable therapeutic goal in hypertensive patients with type 2 diabetes and can be achieved with number of BP-lowering regimens.

Elevated Systolic BP in Type 2 Diabetes Increases Cardiovascular Risk.
Stamler J et al. Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in the Multiple Risk Factor Intervention Trial. Diabetes Care. 1993;16(2):434–44.
He recommends a renin-angiotensin system blocker combined with a thiazide-type diuretic as the most reasonable initial antihypertensive regimen for most people with diabetes, although calcium channel blockers (CCB) and a CCB–angiotensin converting enzyme inhibitor (ACE) combination are also effective. Certain antihypertensive drugs can be associated with incident diabetes (the risk is lowest for angiotensin II receptor blockers and ACE inhibitors followed by CCBs and placebo, β-blockers, and highest for diuretics [Elliot WJ, Meyer PM. Lancet 2007]); however, Dr. Cushman advocated that the positive effects of antihypertensive drugs, especially thiazide-type diuretics, on CV outcomes outweigh their negative effects on glucose metabolism [Ferrannini E, Cushman WC. Lancet 2012].
Baroreflex stimulation and renal denervation are 2 new non-pharmacological treatments receiving attention for treating patients with drug-resistant hypertension (BP >140/90 mm Hg on 3+ antihypertensive drugs in full- or highest-tolerated dose, 1 drug being a diuretic) that target the sympathetic nervous system. Murray Esler, MD, Baker IDI Heart and Diabetes Institute, Melbourne, Australia, presented data regarding the use of these new treatments.
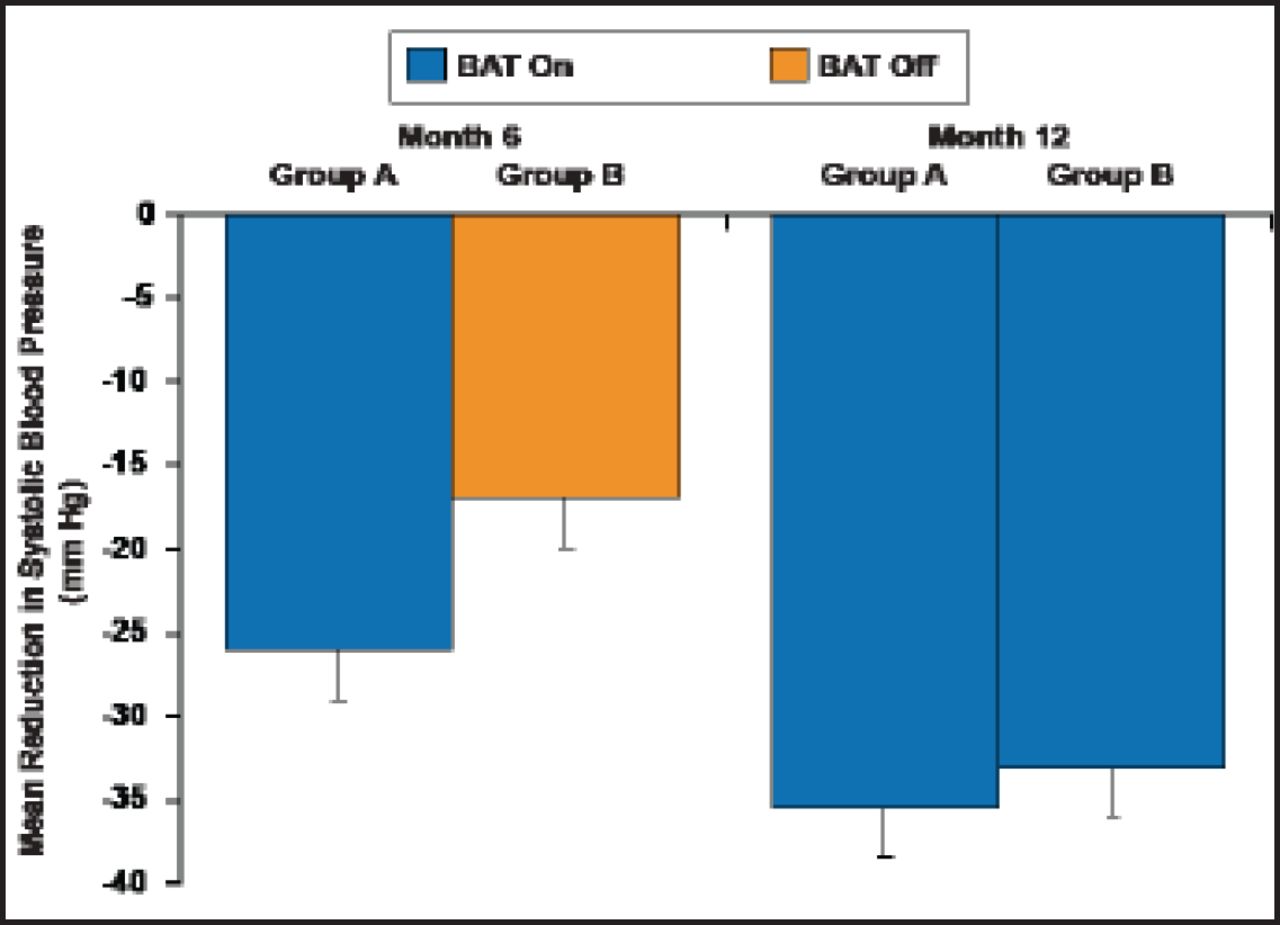
The implantable baroreceptor stimulator is a device that delivers energy pulses targeting afferent nerve inputs to the carotid baroreceptors. These pulses are interpreted by the brain as a rise in BP, which then causes the brain to signal other parts of the body to reduce BP. In the largest clinical trial to-date using this device (n=265), 42% of patients receiving baroreflex activation therapy achieved systolic BP ≤140 mm Hg at 6 months versus 24% not receiving the therapy (p=0.005; Figure 2) [Bisognano JD et al. J Am Coll Cardiol 2011].

Observed Mean Change in Systolic BP.
BAT=baroreflex activation therapy.
Bisognano JD et al. Baroreflex activation therapy lowers blood pressure in patients with resistant hypertension. J Am Coll Cardiol. 2011;58(7):765–73.
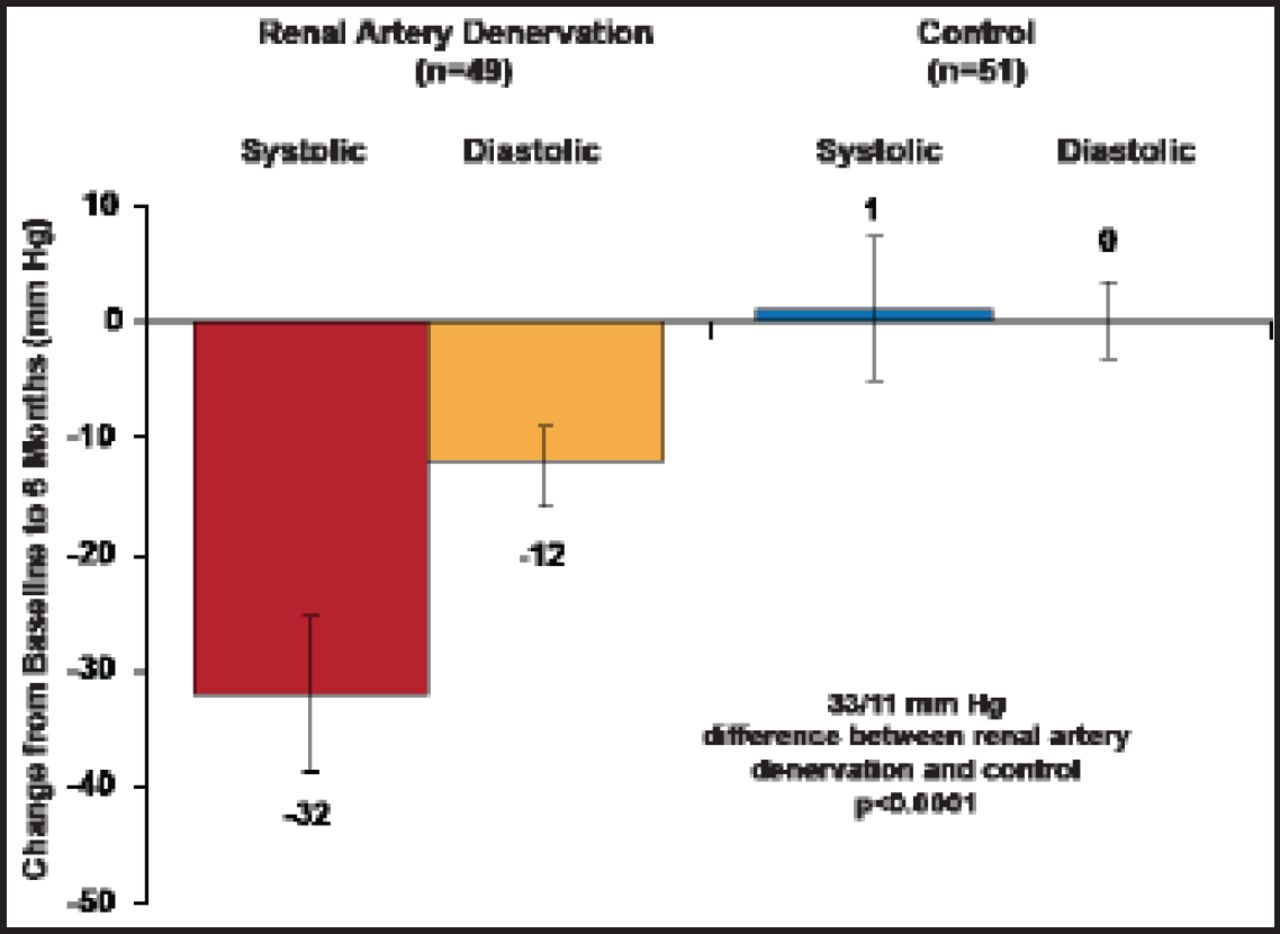
Renal denervation has been shown to delay/prevent the development of preclinical experimental forms of hypertension. The Renal Denervation in Patients With Uncontrolled Hypertension [Symplicity HTN-2] trial was a prospective, randomized trial in 106 treatment-resistant hypertensive patients with a baseline systolic BP ≥160 mm Hg (≥150 mm Hg for type diabetics) in which catheter-based renal denervation using radio frequency was shown to reduce BP by 32/12 mm Hg at 6 months [Symplicity HTN-2 Investigators et al. Lancet 2010] (Figure 3). Prof. Esler shared new data showing that the effect was still durable after 3 years, with no evidence of atherogenesis, fibrotic stenosis, renal artery aneurysm, deterioration in renal function, or orthostatic or electrolyte disturbances [Lenski M et al. Eur Heart J 2012].

Primary Endpoint: 6-Month Office BP.
Reproduced with permission from The Lancet; Symplicity HTN-2 Investigators. Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): A randomised controlled trial. 2010;376(9756):1903–9.
In addition to significantly reducing BP, a small study suggests denervation may also improve glucose metabolism and insulin sensitivity [Mahfoud F et al. Circulation 2011]. Left ventricular (LV) hypertrophy and diastolic dysfunction are associated with elevated sympathetic activity and increased morbidity and mortality [Redfield MM et al. JAMA 2003; Bombeli M et al. J Hypertens 2009]. New evidence suggests renal denervation may improve LV and diastolic function. Six months after 46 resistant hypertensive patients underwent bilateral renal denervation, the patients experienced a significant reduction in LV mass and improved diastolic function in addition to significant BP reduction [Brandt MC et al. J Am Coll Cardiol 2012].
There is also evidence that renal denervation improves cardiorespiratory response to exercise. In a small study with 37 patients, renal denervation reduced BP during exercise without compromising chronotropic competence. Resting heart rate decreased and heart rate recovery improved after the procedure [Ukena C et al. J Am Coll Cardiol 2011]. In another recent study, renal denervation safely reduced BP, renal resistive index, and the incidence of albuminuria without adversely affecting glomerular filtration rate (GFR) or renal artery structure within 6 months [Mahfoud F et al. Hypertension 2012] and may be equally effective in resistant hypertensive patients with Stage 3/4 chronic kidney disease (mean estimated GFR 31 mL/min/1.73 m2) [Hering D et al. J Am Soc Nephrol 2012].
Keys to good outcomes with renal denervation include good patient selection and a thorough preprocedural work-up. Alberto Cremonesi, MD, Villa Maria Cecilia Hospital, Cotignola, Italy, provided his insight regarding appropriate patient selection for renal denervation. It is important to establish that the patient is truly drug-resistant and is not undertreated, non-compliant, or taking other medications/therapies that interfere with BP control. Contributing lifestyle factors (eg, obesity, physical inactivity, excessive alcohol ingestion, high salt intake) should be identified and treated, substances that interfere with BP should be addressed, and patients should also be screened for secondary causes of hypertension. The best treatment modality should maximize pharmacological treatment, which may include maximizing diuretic therapy, combining agents with different mechanisms of action, and using aldosterone antagonists such as spironalactone.
Felix Mahfoud, MD, Universitätsklinikum des Saarlandes, Homburg/Saar, Germany, described his catheter-based approach to renal denervation. The renal nerves should receive ≥5 ablations (120 seconds each) separated both longitudinally and rotationally (spacing >5 mm) with ablation occurring distal to proximal. Prof. Mahfoud noted that a secondary rise in BP should not be expected after renal denervation and that the amount of BP reduction correlates to baseline systolic BP. It is best to use office BP to monitor BP changes, confirmed by ambulatory BP, he added. New treatment catheters using radiofrequency energy, new approaches using ultrasound, and chemical denervation are on the horizon. Although renal denervation shows promise as treatment for a variety of conditions, there remain unanswered questions such as its clinical durability, how to explain non-responders, whether its clinical indication can be expanded beyond hypertension, and whether new ablation systems will address anatomical limitations. These questions are likely to be answered by the Symplicity-HTN-3 trial, an ongoing randomized study in >500 hypertensive resistant patients.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.