

Summary
Around the world, the average 1-year mortality rate is 10% for patients with a diagnosis of atrial fibrillation (AF) who present to an emergency department for any reason. AF is a major global disease, most of what is known about the disorder is based on studies conducted in Europe and North America. The baseline results from the Randomized Evaluation of Long-Term Anticoagulation Therapy [RE-LY AF] registry demonstrated important regional variations in risk factors and treatment of AF across 47 countries.
- Arrhythmias
- Cardiology Clinical Trials
- Prevention & Screening
Around the world, the average 1-year mortality rate is 10% for patients with a diagnosis of atrial fibrillation (AF) who present to an emergency department (ED) for any reason. The rate is highly variable among different countries, noted Jeffrey S. Healey, MD, McMaster University, Hamilton, Ontario, Canada, who reported on the study.
Prof. Healey said that, although AF is a major global disease, most of what is known about the disorder is based on studies conducted in Europe and North America. The baseline results from the Randomized Evaluation of Long-Term Anticoagulation Therapy [RE-LY AF] registry, which were presented at the European Society of Cardiology Congress 2012, demonstrated important regional variations in risk factors and treatment of AF across 47 countries. Dr. Healey and colleagues followed patients for 1 year to document cause-specific mortality and clinical outcomes—most notably, stroke.
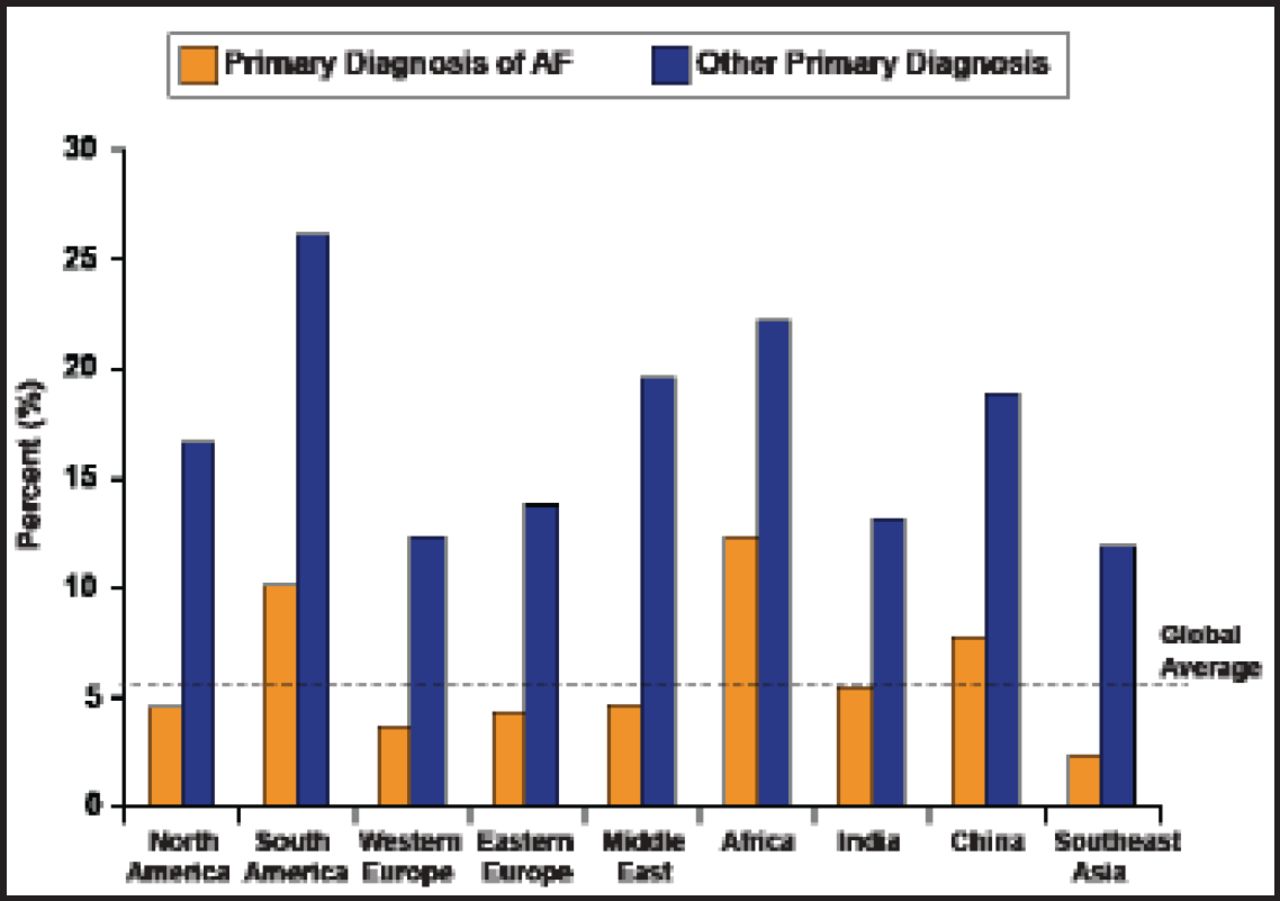
Of the 18,113 patients enrolled in the RE-LY AF trial, 15,408 (85%) were entered in the registry. The vast majority (98%) had AF (while 2% had atrial flutter), and most (79%) had a prior history of AF. For patients presenting to an ED, AF was the primary diagnosis for 44% of patients and the secondary diagnosis for 56%; for those with a secondary diagnosis of AF, the primary diagnosis varied widely between regions, but heart failure (HF) was the most common.
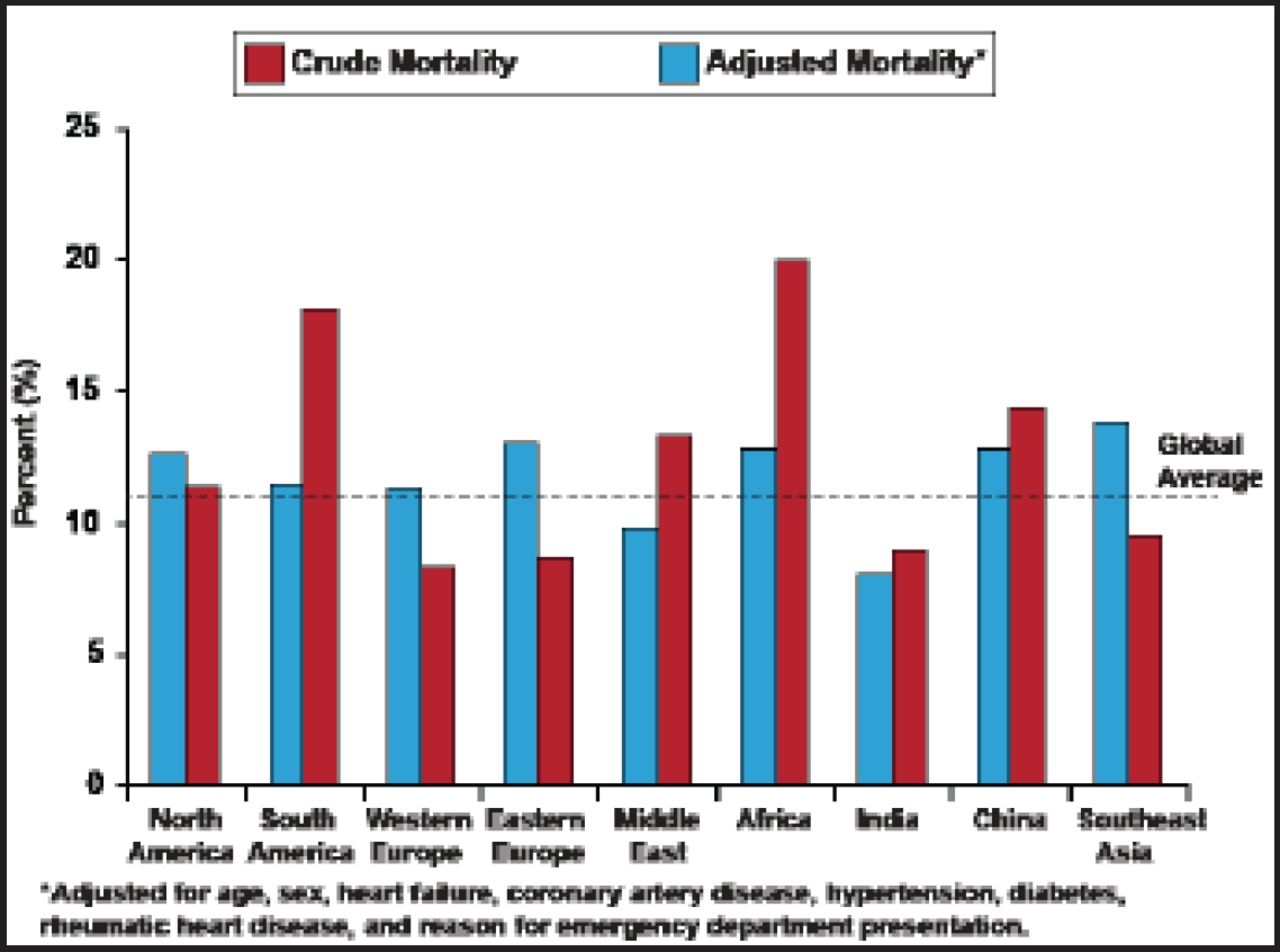
The global average crude mortality rate was 10%, with the highest rates in Africa, South America, and China. When adjustments were made for several variables, the differences were somewhat attenuated, and the rates were highest in Southeast Asia, China, and Eastern Europe (Figure 1). The rates were substantially higher (2–3 fold overall) in all regions when AF was a secondary diagnosis (Figure 2). HF was the primary cause of death overall (34%), followed by infection (12%), and stroke (9.5%). Other causes of death were respiratory failure, cancer, sudden death, and myocardial infarction (all less than 9%).
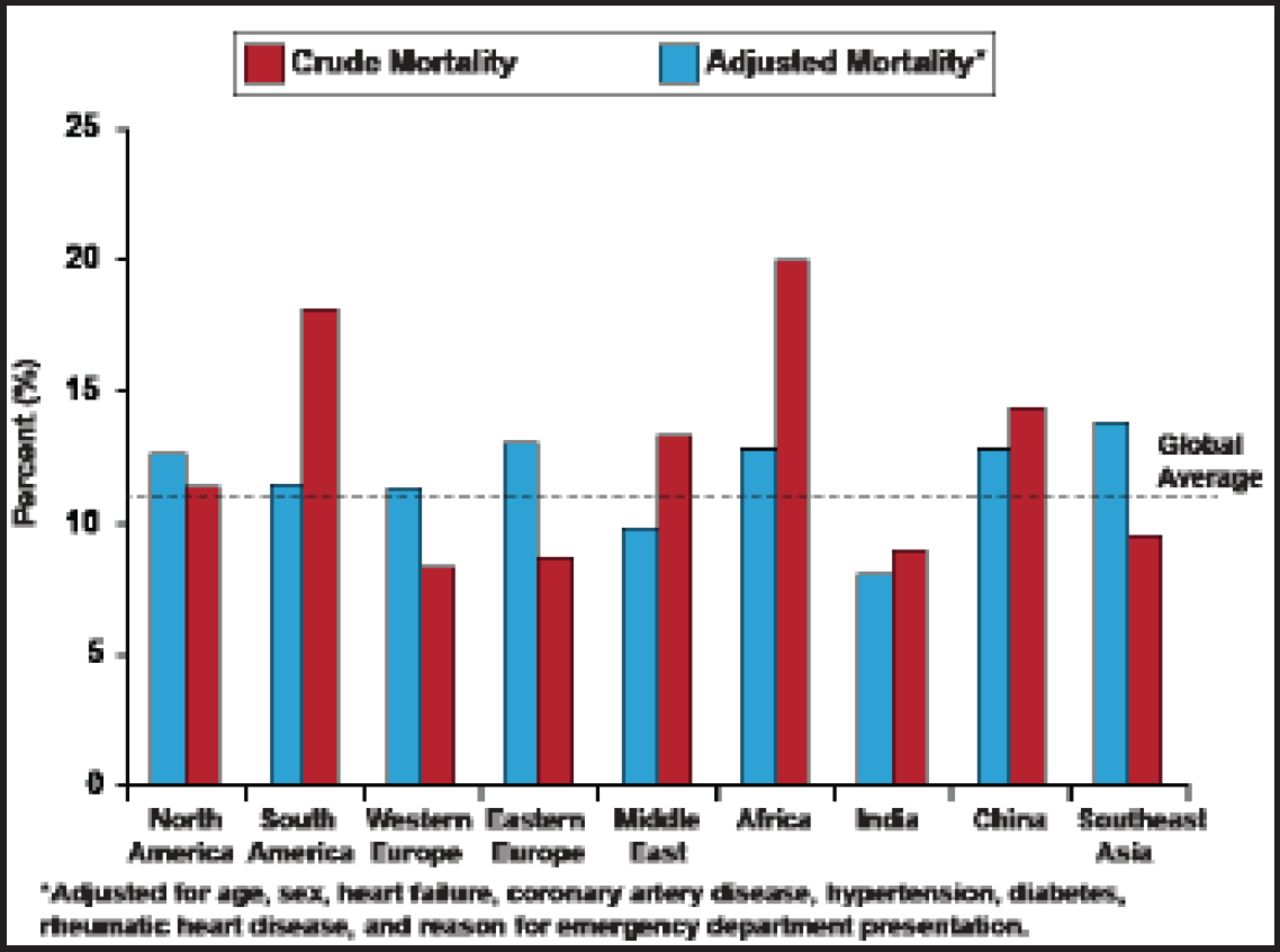
1-Year Mortality for Patients with AF by Region.
Reproduced with permission from J. Healey, MD.
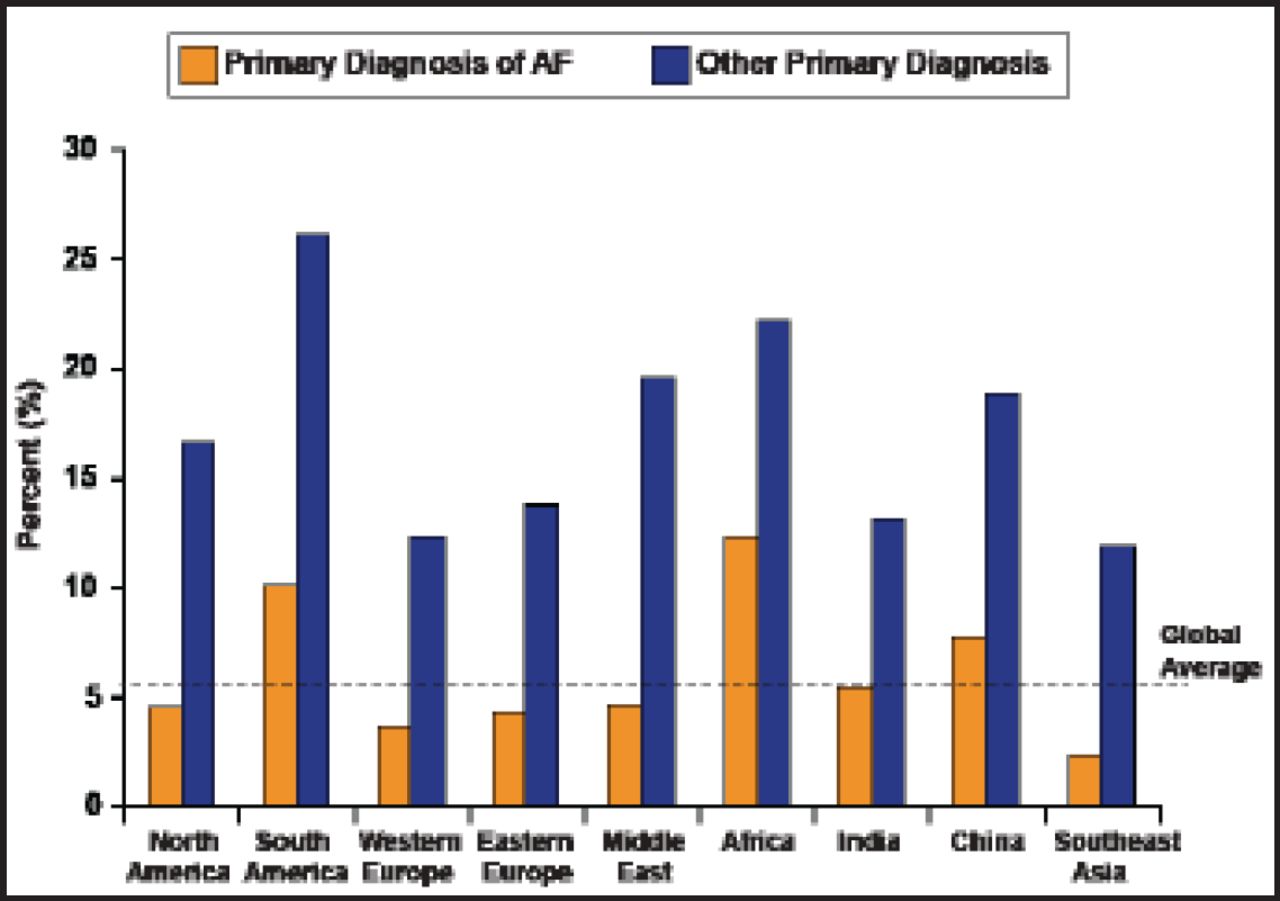
Regional Variation in 1-Year Mortality According to AF as a Primary or Secondary Diagnosis.
Reproduced with permission from J. Healey, MD.
The rate of stroke within 1 year varied among regions, from approximately 8% in Africa to less than 1% in India; the global average was 4%. When adjusted for confounders (age, stroke/transient ischemic attack, HF, hypertension, diabetes, and use of vitamin K antagonists [VKAs]), there was substantially less variation in the stroke rate, ranging from approximately 5% in China and Southeast Asia to 3% in India. Most of the difference in stroke rates could be explained by differences in VKA use.
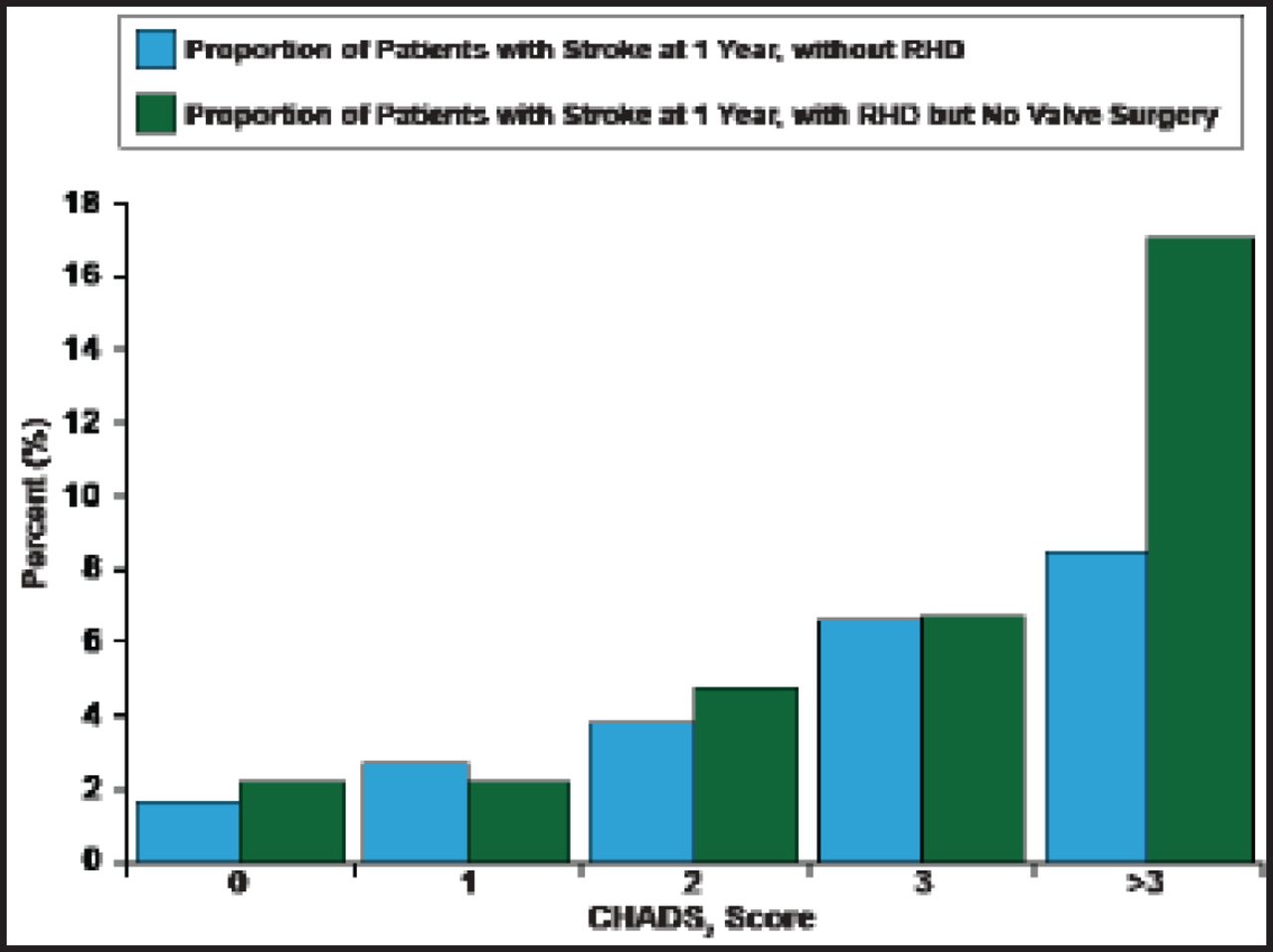
About one third of the patients from India in the registry had documented rheumatic heart disease (RHD). Overall, 1788 patients had RHD, and when the data for this population were analyzed, the risk of stroke was higher for patients with a history of RHD (adjusted rates, 4.3% vs 2.5%). Globally, the CHADS2 score had a greater influence on risk of stroke than the presence of RHD (Figure 3).
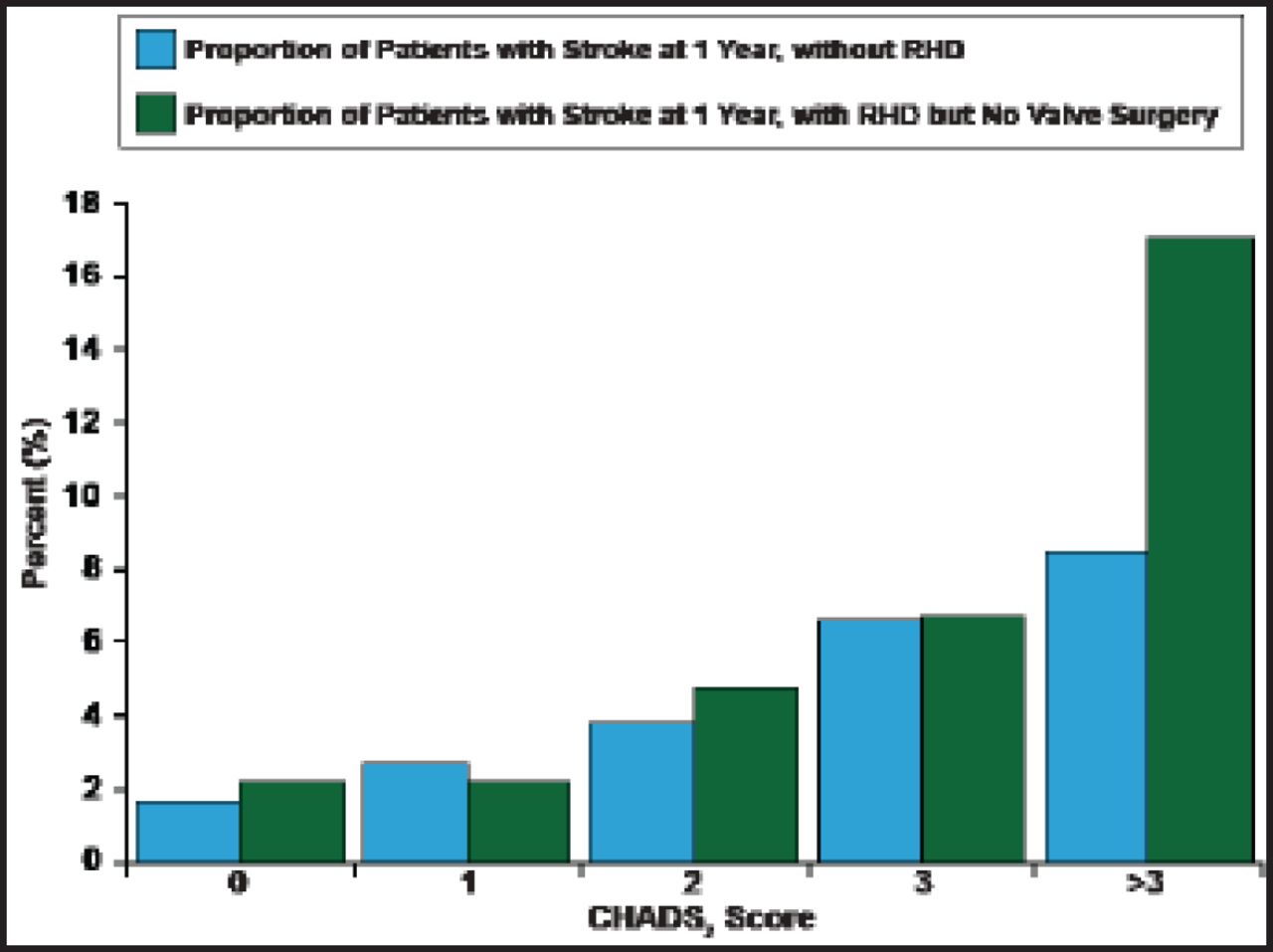
Global CHADS2 -Specific Stroke Rate (1-Year).
Reproduced with permission from J. Healey, MD.
The authors concluded that the 1-year RELY AF registry results underscore the large unmet medical needs and large opportunities for improvement in outcomes for patients with AF. Consistent global application of currently available modalities for diagnosis, risk stratification, and treatment of patients presenting with AF is crucial in reducing the morbidity and mortality of this condition.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.